|
|
 |
|
|
Chapter One
Overview of Title V and Title XIX
To improve the health of all mothers and
children consistent with the applicable health
status goals and national health objectives
established by the Secretary under the Public
Health Service Act for the year 2000, there
are authorized to be appropriated $850,000,000
for fiscal year 2001 and each fiscal year thereafter.
-- Introduction to §501 of the Social
Security Act

A. The Title V MCH Block Grant Program
B. The Medicaid Program
C. Comparing the Title V Program
and Medicaid: At a Glance
D. Coordination Between Title V
and Title XIX
E. The Importance of Interagency
Agreements
One of Medicaid’s
critical roles is to provide financial coverage
for important preventive and primary care services
and specialty services for those eligible; Title
V is essential to help translate those funds
into a system of care that is accessible. This
chapter outlines the respective roles of the
Title V MCH Block Grant and the Medicaid programs
and the ways through which partnerships can
be forged between them. Print and electronic
resources that can aid in strengthening such
partnerships are provided in Appendix A and
are available online at MCH
Library: State MCH-Mediciad Coordination (Title
V and Title XIX Interagency Agreements).
A.
The Title V MCH Block Grant
Program
Beginning with its enactment in 1935 as part
of the Social Security Act (§§501-510),
the goal of Title V echoes that of the U.S.
Department of Health and Human Services (HHS),
Health Resources and Services Administration
(HRSA), Maternal and Child Health Bureau (MCHB)
[then the Children’s Bureau], “to
serve all children, to try to work out standards
of care and protection which shall give to every
child [a] fair chance in the world” (Julia
Lathrop, first Chief of the Children’s
Bureau, 1912).
This legislation allows for specific MCH programs
to provide a base to build upon, with the goal
of improving the health of all women, children,
youth, and families; indeed, Title V remains
the only Federal program with this broad of
a mandate.
During its seventy years of implementation
Title V has undergone many refinements
such as conversion into a block grant
program as well as increased flexibility
and accountability. (Specific legislative
changes affecting both Title V and Title
XIX will be discussed in Chapter Two) |
Title V remains the only Federal
program that focuses solely on improving
the health of all mothers and children. |
|
As a result of these changes, Title V has cemented
itself as a foundation to identify and address
emerging health services needs and to measure
performance of such efforts. States have a large
degree of flexibility in determining priorities
and allocating Federal funds in order to address
the needs of their populations more appropriately.
This flexibility has allowed States to develop
effective and cost-efficient approaches in services
provided; they can address local needs through
tailored programs and policies and then evaluate
and replicate such new program models.
On a national level the Title V MCH Services
Block Grant is charged with:
- Promoting coordination of activities authorized
under Title V and Title XIX, especially Early
and Periodic Screening, Diagnostic, and Treatment
(EPSDT) services (under Title XIX) as well
as other related activities funded by the
Departments of Agriculture, Education, and
HHS.
- Disseminating preventive health care information
to the States.
- Collecting, maintaining, and disseminating
information on the health status and health
service needs of mothers and children (in
conjunction with the National Center for Health
Statistics).
- Providing technical assistance to Congress;
assisting States in developing care coordination
services; distributing a national directory
listing State toll-free numbers of programs
and providers who offer services under Title
V and Title XIX.
Funding
As a permanently authorized discretionary Federal
grant program, Title V is currently authorized
at $850 million. The actual funding has fluctuated
since 1992; see Appendix D for a summary
of recent Title V Block Grant appropriations.
It requires that every $4 of Federal Title V
money be matched by at least $3 of State or
local funds. The program also requires that
a minimum of 30 percent of Title V funds to
states be used to support services for children
with special health care needs (CSHCN) and that
a minimum of 30 percent be used to provide preventive
and primary care services for children. States
may spend no more than 10 percent of Title V
funds on administrative costs.
Title V is administered by the Maternal and
Child Health Bureau. The Title V MCH Services
Block Grant consists of two major funding
categories: (1) the formula grants
to the States and (2) competitive, discretionary
grants for (a) demonstration, research, and
training projects (Special Projects of Regional
and National Significance or SPRANS grants)
and (b) grants focused on development and expansion
of integrated services at the community level
(Community Integrated Service Systems or CISS
grants).
Funding Category 1: Title V MCH Block/Formula
Grants to the 59 States and jurisdictions are
awarded according to a formula based on (1)
the historical share awarded to each State in
1981 and (2) the remaining amount is distributed
based on the number of children in a State who
are at or below the Federal Poverty Level (FPL)
in relation to national figures. These grants
focus on the creation of Federal/State partnerships
to provide service systems to meet challenges
facing MCH, including:
- Reducing infant mortality and the incidence
of disabling conditions among children.
- Increasing the number of children appropriately
immunized against disease.
- Increasing the percentage of low-income
children who receive health assessments and
follow-up diagnostic and treatment (i.e.,
EPSDT) services.
- Coordinating activities of the Title V
programs with those of Medicaid (specifically
EPSDT), WIC, and other health and developmental
disability programs.
- Providing and ensuring access to:
- Comprehensive perinatal health care
for women.
- Preventive and primary child and adolescent
health care services (including nutritional
and developmental services).
- Comprehensive health care, including
long-term care services, for CSHCN.
- Access to rehabilitation services for
children under 16 years of age who are
blind and disabled and receive benefits
under Title XVI, to the extent medical
assistance for such services is not provided
under Title XIX.
- Facilitating the development of family-centered,
community-based, and culturally competent
comprehensive care for CSHCN and their families.
- Putting into community practice national
preventive health standards and guidelines
(e.g., Bright Futures Guidelines for Health
Supervision of Infants, Children, and Adolescents.)
- Providing information to parents about
health care practitioners who provide services
under Title V and Title XIX.
Data from annual Block Grant applications and
reports submitted by all States, territories,
and the District of Columbia are collected and
available through the Title
V Information System. This Web site
allows for searching on key measures and indicators
of maternal and child health, both nationally
and by State.
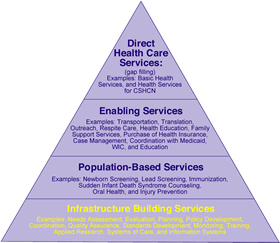
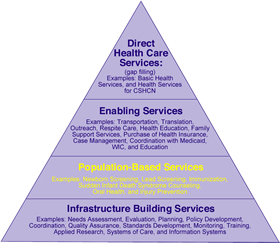
| Services provided to
mothers and children by the Title V MCH
Block Grants are represented in the MCH
Pyramid of Health Services (see Appendix
D for a detailed view of the pyramid).
This pyramid consists of four levels
of service and funding that build upon
each other and provide comprehensive coverage.
Once a State determines its MCH priorities,
it allocates resources to activities that
specifically address those priorities.
The collective effort of all States, in
all levels of the pyramid, contributes
to the national health of mothers and
children. |
 |
Funding Category 2: Federally
administered discretionary grants are
awarded on a competitive basis to a variety
of applicants and extend the Federal partnership
for mothers and children to include such groups
as health professionals, health organizations,
communities, institutions of higher learning,
and others. These grants consist of:
- Special Projects of Regional
and National Significance (SPRANS)
that include MCH research; training grants;
genetic disease testing, counseling, and information
dissemination; hemophilia diagnostic and treatment
centers; and other special MCH improvement
projects that support a broad range of innovative
strategies.
- Community Integrated Service
Systems (CISS) discretionary grants
that seek to reduce infant mortality and improve
the health of mothers and children –
including those living in rural areas and
those with special health care needs –
by funding projects for the development and
expansion of integrated services at the community
level. These systems are public/private partnerships
of health-related and other relevant community
organizations and individuals working collaboratively
to use local resources to address community-identified
health problems. Such projects include home
health visiting programs; projects to increase
participation of health care providers under
Title V and Title XIX programs; integrated
MCH service delivery systems; MCH centers
providing pregnancy, preventive, and primary
care services; MCH projects to serve rural
populations; and outpatient and community-based
services programs for CSHCN.
Division of Funding
The varied funding streams of the Title V Block
Grant work in concert to fulfill the charge
of improving the health of all women and children.
The formula that binds these grants together,
last amended by the Omnibus Budget Reconciliation
Act (OBRA-1989), sets forth that of the funds
authorized for Title V:
- CISS grants account for 12.75 percent of
appropriated funds in excess of $600 million.
- SPRANS grants account for approximately
15 percent of appropriated funds up to $600
million as well as 15 percent of the amount
that remains above the $600 million after
CISS funds are set-aside.
- The formula grants to the States account
for approximately 85 percent of appropriated
funds up to $600 million as well as 85 percent
of the amount that remains above the $600
million after CISS funds are set-aside.
Services
Through these funding mechanisms, Title V programs
serve as the foundation for identifying and
addressing emerging health service needs, gaps
in service delivery, and successful programs
and resources within the MCH community. Title
V funding allows for the creation and maintenance
of a cost-effective infrastructure upon which
to build successful public and private health
services. In addition, Title V programs support
population-based services such as newborn screening,
lead poisoning prevention, injury and violence
prevention, and sudden infant death syndrome
(SIDS) awareness activities. Title V programs
assist families in using resources
available to them by working with Medicaid and
the State Children’s Health Insurance
Program (SCHIP) to inform and enroll these groups
in available programs. Title V programs also
fund preventive and primary care services, promote
home visiting and school-based health programs,
and help in coordinating services.
| Title V supported programs provide
prenatal health services to more than
2 million women, and primary and preventive
health care to more than 17 million
children, including almost 1 million
CSHCN. |
|
Title V historically has had more flexibility
in its use of funds than individual entitlement
programs (in which spending is determined
through eligibility criteria, not by a specific
level of funding). This has permitted Title
V programs to improve the infrastructure
of the health care system, while Medicaid
funds medical assistance for some of the
populations that MCH programs serve. Currently,
the Title V MCH Block Grant funds programs
that serve over 33 million individuals. |
B.
The Medicaid Program
Medicaid, authorized by Title XIX of the SSA
in 1965 as a joint Federal/State entitlement
program, pays for medical assistance to both
“categorically” and “medically”
eligible groups with limited resources (see
next page for a description of these eligibility
groups). It provides health and mental health
care coverage for children and families with
low incomes, long-term health care services
for seniors and people with disabilities, and
provides gap funding for seniors who qualify
for both Medicare and Medicaid.
| Programmatically operating under broad
Federal standards, States are given flexibility
to determine eligibility requirements, set
service standards, set payment rates, and
administer their State programs. |
| Medicaid is the largest source of
funding for health care services for
America’s poorest and most vulnerable
people. |
|
More than 52 million people received Medicaid-supported
services in 2004, including 26 percent of all
children, 50 percent of low-income children, 37
percent of pregnant women, and 20 percent of persons
with disabilities; State and Federal Medicaid
funds for such services topped $305 billion in
that year. In light of these numbers, Medicaid
is the largest funding source for health services
for the country’s most financially strained
populations.
In recent years, the Medicaid program has faced
significant fiscal challenges. The Deficit Reduction
Act of 2005 (DRA) was signed by the President
on February 8, 2006 to address program spending.
Over the course of the next 5 years the DRA
calls for net reductions of $4.8 billion; over
the next 10 years, $26.1 billion. The DRA gives
States flexibility to reconfigure benefits and
cost sharing for certain populations; some early
analysis predicts that changes contained in
the DRA may shift costs to Medicaid beneficiaries
and could limit specific coverage and services.
Reductions planned for in the DRA would be offset
by certain areas of increased spending and coverage
including the Family Opportunity Act and relief
related to Hurricane Katrina.
Based on National Health Care Expenditure Data
from CMS, Office of the Actuary, Medicaid finances
approximately 17 percent of all personal health
care spending in the country, including 37 percent
of all births, 17 percent of all hospital care,
12 percent of health professional services,
17 percent of prescription drug costs, and 48
percent of nursing care costs. (See Appendix
D for a breakdown of Medicaid spending).
Eligibility
While States have substantial control over
Medicaid eligibility for their constituents,
there are set Federally-determined mandatory
Medicaid “categorically needy” eligibility
groups targeted for matching funds, including:
- Persons who meet requirements for Temporary
Assistance for Needy Families (TANF).
- Children under 19 and whose family income
is at or below 100 percent of the FPL.
- Children under 6 years and pregnant women
whose family income is at or below 133 percent
of the FPL. (Only services related to pregnancy,
complications of pregnancy, delivery, and
postpartum care are covered for eligible women).
- Supplemental Security Income (SSI) recipients
(or in States that rely on more restrictive
Medicaid eligibility requirements that pre-date
SSI, this group includes the aged, blind,
and disabled who meet criteria that were in
place in the State’s approved Medicaid
plan as of January 1, 1972).
- Recipients of Title IV adoption or foster
care assistance.
- Special protected groups (e.g., people
who lose cash assistance because of work earnings
or increased Social Security benefits) and
certain Medicare beneficiaries.
Other “categorically related” or
“optional” groups may also be covered
(at the determination of the State). These groups
include:
- Pregnant women and infants 0-1 years whose
family income is less than 185 percent (or
an amount determined by the State) of the
FPL.
- Children under 21 who meet TANF requirements
and are recipients of SSI payments.
- Low-income institutionalized persons.
- Low-income women who are screened for breast
or cervical cancer.
- “Optionally targeted low-income children”
(covered under SCHIP) and low-income people
infected with tuberculosis.
- “Medically needy” persons.
- Aged, blind, or disabled adults whose income
is at or below the FPL.
Medicaid is a prime source of funding for children
and members of low-income working families.
Nearly 65 percent of Medicaid beneficiaries
are in working families. While historically
States have had the ability to impose nominal
deductibles, co-insurance, or co-payments on
certain Medicaid services and beneficiaries,
the DRA of 2005 allows States to charge premiums
and co-payments of up to 20 percent of the medical
service’s cost for certain groups with
a family income above 150 percent of the FPL.
Cost sharing for individuals with a family income
below 100 percent of the FPL remains nominal.
Co-payments of up to 10 percent of the cost
of the services can be charged for beneficiaries
(including children) with incomes between 100-150
percent of the FPL. Regardless of the family
income, cost sharing and premiums for all Medicaid
beneficiaries can not exceed 5 percent of the
family income.
Medicaid is administered as a partnership between
the States and the Centers for Medicare and
Medicaid Services (CMS), which also has authority
over the State Children’s Health Insurance
Program (SCHIP), Medicare, and health insurance
portability standards. SCHIP allows States to
expand Medicaid, create their own separate State
insurance programs, or a combination of both.
SCHIP also provides Federal funds for States
to expand eligibility to cover: (1) mainly low-income
children who do not qualify for Medicaid and
(2) beneficiaries during the Medicaid presumptive
eligibility period.
Services
Title XIX allows States to receive matching
Federal funds for providing certain mandatory
and optional services to most categorically
needy populations. State Medicaid programs generally
cover hospital services (inpatient and outpatient);
services provided by physicians, midwives, and
certified nurse practitioners; laboratory services
and x-rays; nursing home and home health care
services for persons aged 21 and above; EPSDT
services for persons under age 21; family planning
services and supplies; and rural health clinic
and Federally qualified health center services.
Optional services often include prescription
drugs, prosthetic devices, hearing aids, and
dental care.
The DRA of 2005 gives States the ability to
provide “benchmark” coverage. This
would include the Federal Employee Health Benefits
Plan’s Blue Cross Blue Shield benefits,
State employees’ health coverage, or the
largest State HMO’s coverage. The DRA
of 2005 also includes coverage determined by
CMS to be “appropriate” for the
State’s unique populations. However, States
are still required to provide EPSDT benefits.
In addition to choosing which optional services
are covered under Medicaid, under broad Federal
guidelines States have the authority to set
the duration of such services. The duration
of Medicaid services must be of sufficient length
to accomplish the goals of the benefits and
must not discriminate among those covered based
on diagnosis or medical condition. As Medicaid’s
comprehensive and preventive child health program
for individuals under the age of 21, EPSDT preventive
care services must be provided by the States
during beneficiaries’ well-child visits
to identify physical (including vision, hearing,
and dental) and mental conditions. States also
must provide other necessary health care, diagnosis
services, treatment, and other measures to correct
or ameliorate defects as well as physical and
mental illnesses and conditions discovered by
the screening services. States must facilitate
access to rural health clinic and federally-qualified
health center (FQHC) services.
Medicaid is an entitlement program; it provides
health insurance based on the program’s
eligibility criteria, not by a capped level
of funding. Medicaid services are handled as
a vendor payment program, with States paying
providers on a fee-for-service basis or through
prepayment services. Payments to providers must
be at a set rate and must be considered payment
in full. Deductibles or co-payments may be charged
on some Medicaid services and benefits; additional
payments may be made to hospitals that serve
large numbers of Medicaid patients.
A percentage of these payments, called the
Federal Medical Assistance Percentage (FMAP),
is covered by Federal funds based on a formula
comparing each State’s average per capita
income with the national average. This amount
varies from 50 percent to 83 percent and is
determined annually; in FY 2003 the average
was 56.6 percent nationally. States with a higher
per capita income are reimbursed at a smaller
percentage of their costs.
Medicaid expenditures are increasing at a rapid
rate due in part to rising medical and long-term
care services, increases in Medicaid populations,
and increasingly more numerous and expensive
prescription drugs. At the current rate of expansion,
Medicaid expenditures are expected to top $425
billion by FY 2008. States are looking for ways
to reduce Medicaid spending such as limiting
prescription spending, reducing provider payments
and recipient benefits, and limiting eligibility.
C.
Comparing the Title V Program and Medicaid:
At a Glance
Title V was authorized in 1935; Medicaid in
1965. Both programs are complex in their own
right and during the span of their existence
have become even more so. Many of the details
that make each program unique have been discussed
in the preceding sections, yet blur amidst complex
regulations and ever-changing policy.
See Title
V Information System for a history
and current legislation on the Title V MCH Block
Grant or Medicaid
for a summary of the Medicaid program. For MCH
data sources, see Data.
Additional resources are also available in Appendix
A and at MCH
Library: State MCH-Mediciad Coordination (Title
V and Title XIX Interagency Agreements).
Highlights of the Title V and Medicaid programs
are presented in the following chart to aid
in obtaining a clearer view of each program’s
mandates, requirements, foci, and strengths.
| Title
V and Medicaid, Compared |
|
|
Title
V |
Medicaid |
|
Authorized By |
Sections 501-510, SSA, in 1935 |
Sections 1901-1936, SSA, in 1965 |
|
Administered By |
U.S. Department of Health and Human
Services (HHS), Health Resources Services
Administration (HRSA), Maternal and Child
Health Bureau (MCHB). |
U.S. Department of Health and Human
Services (HHS), Centers for Medicare and
Medicaid Services (CMS), Center for Medicaid
and State Operations (CMSO). |
|
Overarching Goal |
To improve the health of all
women, children, youth, and families. |
To pay for medical assistance to both
“categorically” and “medically”
eligible children and families with low
incomes. |
|
Funding Mechanism |
Discretionary Federal “block”
grant. |
Joint Federal/State entitlement program. |
|
Funding and/or Beneficiary
Requirements |
Funding Requirements:
• Every $4 of Federal funds must be
matched by at least $3 of State/ local
funds.
• At least 30% of funds must support
CSHCN.
• At least 30% of funds must support
preventive and primary care services for
children.
• No more than 10% of funds can be used
for administration. |
FMAP Requirements:
• Federal funds (the “Federal Medicaid
matching rate”) are provided for services/administration
dependant on State per capita income (from
50-83% with average of 57%).
Eligibility groups include:
• “Mandatory” categorically needy persons
(pregnant women and infants at or below
133% FPL).
• “Optional” categorically needy persons
(pregnant women and infants with incomes
between 133%-185% FPL).
• Medically needy persons (who qualify
for coverage because of high medical expenses). |
| Title
V and Medicaid, Compared (continued) |
|
|
Title
V |
Medicaid |
|
People Served and/or
Covered |
Title V provides services
to:
• Over 33 million women and children
total, consisting of:
• 2.5 million pregnant woman
• 3.9 million infants less
than 1 year
• 22.5 million children 1
to 22 years
• 1.4 million CSCHN
• Of the 33 million individuals:
• 1.1 million are Medicaid-eligible
pregnant women
• 1.4 million are Medicaid-eligible
infants under 1 year old
• 6.9 million are Medicaid-eligible
children 1-22 years old.
• 0.5 million are Medicaid-eligible
CSHCN. |
Medicaid covers:
• 52 million people total (2004 data),
consisting of:
• 26% of all children,
• 50% of low-income children
• 37% of pregnant women
• 20% of persons with disabilities |
|
Legislative Reform/
Program Services |
• Omnibus Budget Reconciliation Act
(OBRA-1981):
• Incorporated five other smaller, related
programs into Title V.
• Granted States increased spending
flexibility.
• Required each State Title V agency
to participate “in the arrangement and
carrying out of the coordination agreements
…related to coordination of care and services
under this title and Title XIX” [§505(2)(F)(ii)].
• OBRA-1989: provided stricter application,
spending, and reporting requirements.
• 1998: Title V Information System developed
to collect and report data. |
• Personal Responsibility and Work Opportunity
Reconciliation Act (1996): restricted
eligibility for SSI coverage for certain
populations.
• Balanced Budget Act (BBA) (1997):
reinstated eligibility for those children
and those included under SCHIP.
• Ticket to Work and Work Incentives
Improvement Act (1999): provided a sliding
scale payment income-based premium.
• Medicare, Medicaid, and SCHIP Benefits
Improvement and Protection Act (BIPA)
(2000): allowed for additional payments
to hospitals serving large Medicaid populations.
• Deficit Reduction Act (DRA) (2005):
scheduled to create $39 billion in Medicaid
reductions from 2006-2010 by shifting
costs to beneficiaries and limiting certain
services for low-income recipients. |
D.
Coordination Between Title V and Title XIX
The MCH Services Block Grant and Medicaid both
play a key role in improving access and health
outcomes for children, youth, and families.
Coordination and partnerships between the two
programs is key in achieving this purpose. “Through
the Title V Maternal and Child Health Block
Grant to States Program, core public health
functions for mothers and children are strengthened,
State MCH needs are assessed, and gaps in services
are identified so that statewide systems of
health care for all mothers and children, regardless
of race, ethnicity, or culture, are ensured.
The outcomes of these MCH efforts are captured
as evidence of progress and to provide accountability
to the States and the nation as a whole.”
[cited from Learn
More Title V Today ]. Title V programs
help to provide a structure and assistance in
using that funding to support a system that
those persons can use. Medicaid provides health
care coverage, including preventive, primary
and some specialty services, to those persons
who are eligible.
Specific details of the two programs are distinct.
The Title V Block Grant administers a set amount
of grant funding to the States, which are given
great flexibility in deciding innovative ways
to meet the program’s mission of improving
the health of all women and children, including
those eligible for Medicaid. Title V is thus
a public health program to be used by State
Health Agencies to meet State-determined goals
and objectives consistent with the National
Healthy People 2010 goals. Title V programs
assess the needs of their populations and then
plan and ensure that adequate policies and programs
are in place to address those needs.
Title V programs have great expertise in providing
an infrastructure and access to services that
Medicaid in turn can build upon. Title V programs
have knowledge in developing model programs
and materials that can be used by Medicaid;
Title V personnel are also skilled in providing
outreach and enrollment services to Medicaid
beneficiaries thus enabling access on behalf
of Title XIX.
Medicaid, on the other hand, often serves as
a health insurance program that purchases or
provides reimbursement for preventive services
and primary care to persons of limited income,
with disabilities, or of advanced age who meet
specific requirements. As such, Medicaid deals
with a specific sub-set of the Title V population.
Medicaid often relies on Title V programs to
provide access to and delivery of health and
mental health services.
Partnerships between Title V and Medicaid have
had a long history of providing increased services
and preventing duplication of effort. Such coordination
is the result of a long and well-planned series
of legislative decisions that mandate that the
two programs work together (these legislative
mandates are examined in the next chapter).
By tying the two together through mutual requirements,
the potential for a dynamic synergy has been
established.
E.
The Importance of Interagency Agreements
Interagency Agreements (IAAs) [required in
§509(a)(2) and referenced to in §1902(a)(11)(b)],
can serve as a major resource in coordinating
activities and providing mutual support between
the two agencies (or divisions within an agency
in the State department of health) that administer
the two programs. As required by Federal mandate
the IAAs must (1) utilize Title V agencies (or
their grantees) who can furnish care and service
to Medicaid beneficiaries, (2) make “appropriate”
provisions to reimburse Title V agencies (or
their grantees) for covered services provided,
and (3) provide for sharing of information and
education on pediatric vaccinations and delivery
of immunization services.
IAAs are crucial for several reasons. They
provide a formal structure delineating the programmatic
and administrative responsibilities of each
agency. They also provide for continuity in
implementing policies over time. Finally, they
build in a system of communication and accountability
between programs. Bolstered by these IAAs, strong
partnerships have been established on the State
level that address, and often go beyond, the
legislative requirements. Through such partnerships,
Title V programs are often not highly visible
to the general public because their goal is
to collaborate with Medicaid staff to ensurelinkage
among multiple programs (Title V, Medicaid,
and others) to provide a seamless system
of care for beneficiaries.
While these IAAs and the partnerships they
establish vary by State, there are many common
strategies in which Title V works with Medicaid
to increase access to care. These strategies
can be organized in terms of the four-tiered
MCH Pyramid of Health Services (explained more
fully on page 6), beginning from the base up
with Infrastructure Building Services.
Methods Through Which Title V and
Medicaid Coordinate
Infrastructure
Building Services: These include
evaluation, policy development, coordination,
standards development, training, and information
systems. |
 |
- Title V provides funding and experience
for development and implementation of
model programs that benefit Medicaid
beneficiaries.
- Title V and Medicaid develop jointly
agreed upon policies and standards of
care for Medicaid beneficiaries (especially
relevant with EPSDT services).
- Title V provides expertise to Medicaid
in analyzing utilization patterns and
recommending ideas for services provided
such as more effective treatment services
or options for families.
- On a State level, Medicaid utilizes
Title V population data collected through
such systems as the Title V Information
System to provide key population and
service statistics, performance and
outcome measures, and benchmarks.
- Medicaid uses materials developed
by Title V grantees, either directly
or with modifications for Medicaid audiences.
- Title V and Medicaid collaborate
in planning activities such as designing
benefit packages, application forms,
enrollment procedures, and referral
and follow-up protocols.
|
Population-based
Services: These include screenings,
immunizations, oral health, nutrition
and outreach, and public education. |
 |
- Title V programs and Medicaid perform
EPSDT services for infants, children,
and adolescents, including CSHCN.
- Title V programs coordinate services
such as lead screening and referral
to Title V programs for additional evaluation
and management, if necessary.
- Title V programs provide public education
to Medicaid beneficiaries on nutrition
and oral health issues, stressing the
need for such services from an early
age.
|
Enabling Services:
These include outreach, health education,
family support services, case
management, and coordination with Medicaid.
|
 |
- Title V programs provide outreach
and enrollment services to eligible
beneficiaries, allowing Medicaid funds
to pay for those services.
- Medicaid performs outreach to audiences
traditionally supported by Title V programs
and vice-versa.
- Title V agencies administer programs
that support Medicaid beneficiaries,
not only to ensure enrollment but to
track and/or provide follow-up treatment.
- Medicaid utilizes Title V programs
for care coordination and assistance
in accessing treatment services (e.g.,
facilitating transportation).
|
Direct Health
Care Services: These include basic
health services and health services for
CSHCN. |
 |
- Title V pays for gap-filling services
to Medicaid beneficiaries.
- Title V provides funds for services
needed by uninsured children and pregnant
women and for necessary services not
covered by Medicaid or other sources.
- Medicaid coordinates with Title V
programs to pay for community specialists
who provide appropriate care for CSHCN.
|
While these strategies vary widely, they are
powerful examples of how States partner Title
V and Medicaid services; all such strategies
rely on unique strengths that each program brings
to the table. Title V has a broad, inclusive
definition of health care that includes prevention
and early intervention services; its programs
have experience in working with and coordinating
broad networks of service providers and public
health experts. In addition, Title V has the
experience with surveillance of health status
and has data systems in place to collect and
monitor data. Title V programs also have knowledge
of services that insurance plans don’t
cover as well as what services Medicaid beneficiaries
need. Finally, Title V programs already have
“best practice” performance guidelines
such as the Bright Futures Guidelines for
Health Supervision of Infants, Children, and
Adolescents that directly relate to the
services required by Medicaid.
One of Medicaid’s greatest strengths
is due to its extensive funding. Next to education
it is the second largest category of State spending
and is the largest source of Federal funding
to the States. Nationally, Medicaid covers 1
in every 5 children and as such plays a critical
role in insuring the country’s 34 million
low income children and parents. At the same
time, Medicaid plays a critical role in addressing
the needs of over 13 million persons with disabilities
and persons over age 65. By operating on both
Federal and State funds under the FMAP plan,
States have a degree of support during both
strong and weak economic times and are encouraged
to invest in the Medicaid program while utilizing
partnerships such as those with Title V programs.
The partnerships established between Title
V programs and Medicaid are much more than lists
of services and strengths. Title V programs
play a key partnership role in developing services
for Medicaid. Such partnerships are essential;
Title V and Title XIX programs are much more
effective working collaboratively. The interagency
agreements provide the bridge to link these
powerful programs together.
|

