FORUM
SUBSTANCE ABUSE IN YOUR PATIENTS: BEYOND WHAT IS TAUGHT IN YOUR RESIDENCY
Chair:
Nora D. Volkow, M.D.
Director
National Institute on Drug Abuse
Overview
According to the most recent National Survey on Drug Use and Health, an estimated 19.7 million Americans or 8.1% of the population aged 12 or older were current (past month) illicit drug users and nearly 8 million are in need of treatment. Drug abuse has far-reaching consequences for individuals, families, communities, and society at large. Research has demonstrated that addiction is a disease that can be successfully treated, but not if the symptoms are undetected and the problem undiagnosed. This Forum brings together leading experts in the treatment of drug abuse and addiction to discuss how to recognize drug abuse problems as well as introduce participants to the most recent discoveries about the neurobiology of addiction and how those discoveries are contributing to the development of new, effective addiction treatments.
What They Didn’t Teach You in Residency About Diagnosing & Treating Prescription Opioid Abuse
Herbert D. Kleber, M.D.
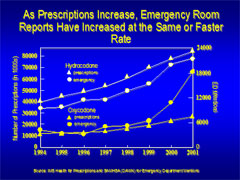
Although prescription opioid abuse is one of the fastest growing drug problems, most psychiatric residents have little exposure to its diagnosis and treatment. Between 1994 and 2001, narcotic analgesic abuse more than doubled. Schedule III products (e.g., Vicodin) are readily available without prescription via the Internet. Schedule II opioids (e.g., Oxycontin) are mainly obtained from prescriptions, doctor shopping, theft from medicine cabinets, and street sales. The greater availability is significantly related to concerns about inadequate treatment of pain and, therefore, increased prescribing during the 1990s, which has continued to the present. Although there is a relatively high prevalence of comorbid chronic pain and substance abuse, most individuals treated for pain with these agents do not become addicted.
Treatment options include: Detoxification to antagonist maintenance (naltrexone, nalmefene, and depot naltrexone), residential therapeutic communities, and abstinence-oriented programs (counseling, and 12 step programs), and maintenance with methadone or buprenorphine.
For individuals who have been addicted for more than a year, detoxification, unless followed by continual treatment such as a narcotic antagonist or residential therapeutic community, is associated with a high relapse rate. These patients are usually better served by maintenance on buprenorphine.
Pharmacotherapy: From Antabuse to Zenova-vax
Thomas Kosten, M.D.
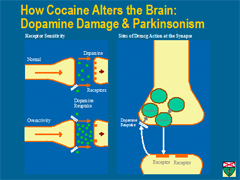
Two new concepts are evolving in our pharmacotherapy of substance abuse—pharmacogenetics and immunotherapy. Both are being applied to the treatment of stimulant dependence. Disulfiram, an inhibitor of dopamine beta hydroxylase (DBH), is being successfully used to treat cocaine dependence, and a specific genetic polymorphism that relates to treatment response has been identified in the promoter region of this gene. This polymorphism leads to a 10–100-fold lower level of the DBH enzyme and is relatively common in about 40 percent of individuals. In these individuals, DBH is substantially inhibited by disulfiram leading to an increase in dopamine release and a reduction in norepinephrine production and release from neurons. This effect appears to reduce cocaine craving and the priming effect of cocaine use that leads to relapse. Immunotherapy has taken the form of an anti-cocaine vaccine that can block the effects of cocaine by retaining it in the bloodstream, where it is inactivated by another enzyme in the blood—cholinesterase. In human laboratory studies and in outpatient clinical trials, this vaccine takes several injections over about 2 months to produce adequate antibodies, but then substantially blocks the effects of cocaine.
Clinical Implications and Applications of Advances in Addiction Research to the Evaluation and Treatment of Adolescents
Paula D. Riggs, M.D.
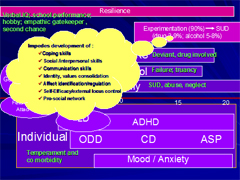
Advances in addiction research highlight the importance of understanding neuro-developmental factors that increase adolescents’ vulnerability to substance use disorders and mental health problems.
Data from Dr. Riggs' recently completed randomized controlled trial of fluoxetine vs. placebo + CBT support the safety and efficacy of integrated, concurrent treatment of a common psychiatric comorbidity (MDD) in adolescents who have active substance use disorders. Preliminary data from this study also show that adolescents with marijuana dependence have greater pre-treatment brain activation in “reward” circuits in response to marijuana cues than to food cues, and greater post-treatment (after 16 weeks’ CBT) brain activation to the same marijuana cues in cortical/pre-frontal areas compared with food cues.
This presentation aims to help understand the key developmental risk factors that increase the risk of mental health problems, substance abuse, and other behavioral pathology in adolescents, along with the clinical implications of scientific advances in our understanding of adolescent brain development and the neuro-developmental processes underpinning addiction and commonly associated psychiatric comorbidity.
What Should All Psychiatry Residents Know About Treating Addiction?
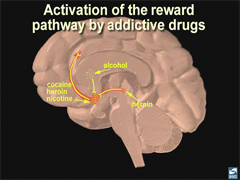
Charles P. O'Brien, M.D., Ph.D.
In this brief presentation the definition of addiction is discussed. An important point is that tolerance and physical dependence are normal responses to repeated use of drugs that affect the central nervous system and are not necessarily a sign of addiction. Drug abuse and addiction are essentially maladaptive memories, a disorder of the reward system, which is activated as the reinforcer of all behavior. There are a large variety of drugs that can be abused, but all have in common the activation of this reward system. In recent years, research has brought us new medication that can be used in combination with psychotherapy. A discussion of the action mechanism of some of these medications is described. The essential goal of addiction treatment is prevention of relapse. Detoxification is only the beginning of treatment but not a treatment by itself. In addition to medications, we have specific forms of psychotherapy. These have been codified in treatment manuals and can be studied in research projects just as the dose of medication can be studied quantitatively. The best treatment for addictive disorders is a combination of psychotherapy and medication. There is absolutely no evidence that medications interfere with psychotherapy or 12-step programs. In fact there is good evidence that they enhance the benefits obtained from these psychosocial interventions.
|