Error processing SSI file
|
|
 |
|
|
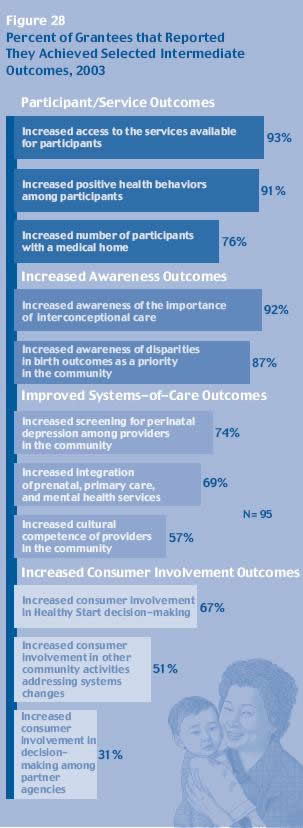
INTERMEDIATE PROGRAM OUTCOMES
| Having provided a snapshot
of individual program components, it is
important to reflect on the Healthy Start
program as a whole. Figure 28 indicates
the percentage of grantees that selfreported
achievements in 11 intermediate outcomes
based on the Healthy Start logic model
(see appendix). They are grouped into
four categories: participant/service outcomes,
increased awareness outcomes, systems-of-care
outcomes, and consumer involvement outcomes.
Grantees were more likely to report improvements
in services than systems-related activities.
This is consistent with the finding that
grantees devoted the majority of their
grant funding to the services components,
with the average allocation being 80 percent
to services and 20 percent to systems.
Grantees also were more likely to report
that they achieved outcomes related to
increasing awareness than increasing consumer
involvement. The former targeted providers
and the general public, while the latter
targeted consumers, perhaps signifying
that there are greater challenges in reaching
consumers than other populations.
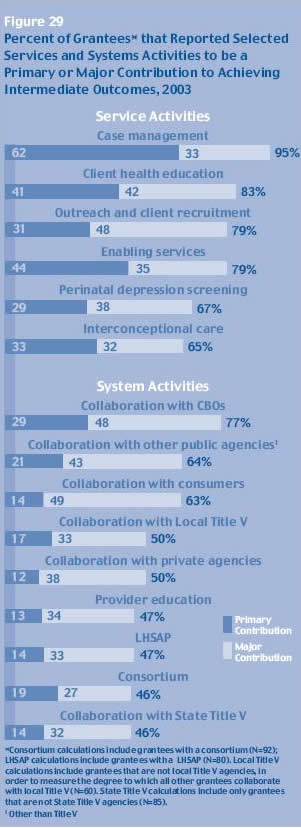
To understand the extent to which particular
program activities contributed to achieving
the intermediate outcomes, the survey
asked grantees to rate the perceived contribution
of seven services-related and eight systems-related
Healthy Start activities. For each activity,
grantees indicated whether it made a primary
contribution, a major contribution, a
moderate contribution, a minor contribution,
or no contribution at all. Grantees were
more likely to report that services activities
made a primary or major contribution to
achieving their intermediate program outcomes.
Case management was perceived to make
the largest contribution, followed by
client health education. Far fewer grantees
reported that systems activities made
a primary or major contribution, in particular,
provider education, consortia, local health
system action plan, and collaboration
with State Title V agencies. |
 [D] [D]
|
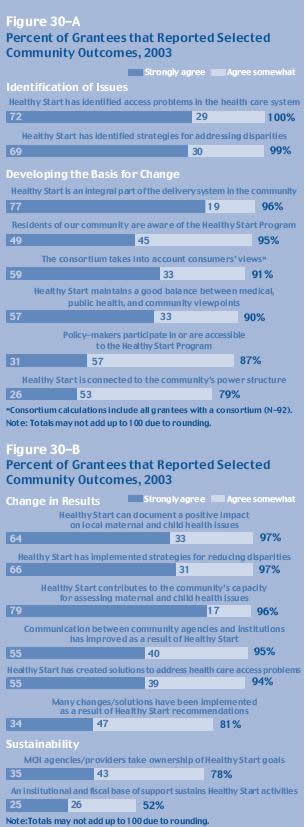
| In addition to reflecting
on their projects’ inter-mediate
outcomes and relative contributions of
program components, grantees commented
on 16 statements concerning Healthy Start’s
relationships to the communities in which
they are based. These statements represented
a continuum of program change, beginning
with the identification of issues, progressing
to building capacity for change, seeing
tangible results, and finally, offering
evidence of sustainable change. It was
expected that grantees would be at different
points along this trajectory and, indeed,
found that grantees were more likely to
report outcomes within the first three
stages of systems change than in the final
stage of sustainability.
All grantees (100 percent) expressed
agreement that Healthy Start has identified
access problems in the health care system
and 99 percent agreed that Healthy Start
has identified strategies for addressing
disparities. In addition, a large majority
of grantees agreed that Healthy Start
has made progress in developing the basis
for change. In particular, grantees reported
the project was an integral part of the
service delivery system in the community
(96 percent) and that community residents
are aware of the project (95 percent).
Grantees were less likely to report that
policymakers participate in or are accessible
to the Healthy Start project (87 percent);
and that Healthy Start is connected to
the community’s power structure
(79 percent) such as local government
representatives and decision-makers within
local institutions. |
 [D] [D]
|
| The
majority of grantees agreed that the Healthy
Start project yielded actual changes in
results. Of the six items in this domain,
at least 94 percent of the grantees agreed
(either strongly or somewhat) with five
of them. Grantees were less likely to
report that many changes/solutions have
been implemented as a result of Healthy
Start recommendations (81 percent).
The final stage of the trajectory is
sustainability. A relatively smaller number
of grantees agreed that maternal and child
health agencies/providers take ownership
of Healthy Start goals (78 percent), or
that an institutional and fiscal base
of support sustains Healthy Start activities
(52 percent).
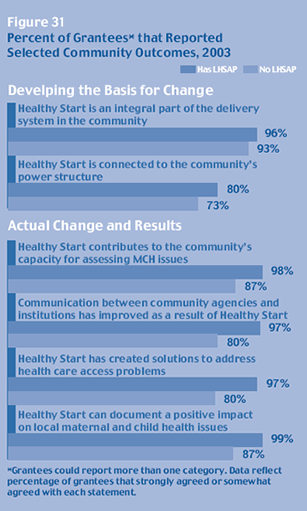
The presence of a LHSAP has a significant
effect on the assessment of the effect
of the Healthy Start project on the community.
Projects with a LHSAP were more likely
to agree (either strongly or somewhat)
that Healthy Start is connected to the
community’s power structure, has
led to improved communications among agencies
in the community, has contributed to the
community’s capacity for needs assessment,
has created solutions to access problems,
and can document a positive impact. These
results suggest that a LHSAP may help
Healthy Start grantees move along the
trajectory toward having a lasting effect
on their communities. |
 [D] [D]
|
| The
existence of a Local Health System Action
Plan or a sustainability plan did not result
in any significant associations with regard
to grantee perceptions of their project’s
effects on bringing about sustainable change.
This result may not be too surprising in
light of the findings which showed that
most grantees with a sustainability plan
did not have any resources in place to absorb
their services – and thus would not
have an institutional or fiscal base of
support to sustain Healthy Start activities.
Although grantees may be building a foundation
for sustainable change, these results suggest
that grantees perceive substantial barriers
to sustaining the Healthy Start program
in the absence of Federal funding. |
 [D] [D]
|
next page: Appendix
|

