|
Home ·
Resources ·
Search ·
Textbook Map ·
OEI Home ·
NHLBI Home
Guidelines on Overweight and Obesity: Electronic Textbook |
|||||||
Determination of Degree of Abdominal ObesityThe presence of excess fat in the abdomen, out of proportion to total body fat, is an independent predictor of risk factors and morbidity. A high waist circumference is associated with an increased risk for type 2 diabetes, dyslipidemia, hypertension, and CVD in patients with a BMI in the range between 25 and 34.9 kg/m2. Relatively accurate measures of total abdominal fat can be made by magnetic resonance imaging (529) or computed tomography (500, 530). These methods, however, are expensive and not readily available for clinical practice. Research with these techniques, nonetheless, has shown that the waist circumference correlates with the amount of fat in the abdomen, and thus is an indicator of the severity of abdominal obesity. In this document the term "waist" circumference is used instead of "abdominal" circumference because it more accurately describes the anatomical site of measurement.
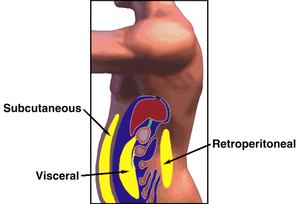
Rationale: Fat
located in the abdominal region is associated with greater health risks than
that in peripheral regions, e.g., the gluteal-femoral area (155-159, 429, 430). Abdominal fat is
described as having three compartments: visceral, retroperitoneal, and
subcutaneous (529, 531, 532). Several
studies suggest that the visceral fat component of abdominal fat is the most
strongly correlated with risk factors (160, 161,
533, 534); other studies, however, indicate that the subcutaneous component
is the most highly correlated with insulin resistance (529, 535, 536).
Therefore, the relative contributions of different components of abdominal fat to overall risk remain to be determined with certainty. Nonetheless, the presence of increased total abdominal fat appears to be an independent risk predictor when the BMI is not markedly increased (537). Therefore, waist or abdominal circumference, as well as BMI, should be measured not only for the initial assessment of obesity, but also as a guide to the efficacy of weight loss treatment. In some populations, waist circumference is a better indicator of relative disease risk than is BMI; examples include Asian Americans or persons of Asian descent living elsewhere. Waist circumference also assumes greater value for estimating risk for obesity-related disease at older ages. The waist-to-hip ratio (WHR) also has been used in a number of epidemiologic studies to show increased risk for diabetes, coronary artery disease, and hypertension (500). However, waist circumference has been found to be a better marker of abdominal fat content than is WHR (85). Whether WHR imparts any independent information about disease risk beyond waist circumference is uncertain, but between the two, the waist circumference appears to carry greater prognostic significance. Therefore, in clinical practice, abdominal fat content should be assessed and followed by measuring waist circumference.
|
||