Department of Health and Human Services
Centers for Disease Control and Prevention
|
|
|||||||||||||
|
|
|
|
|
||||||||||
|
|
|
|
|
|
2008 Atlas of Stroke Hospitalizations Among Medicare Beneficiaries
|
||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||
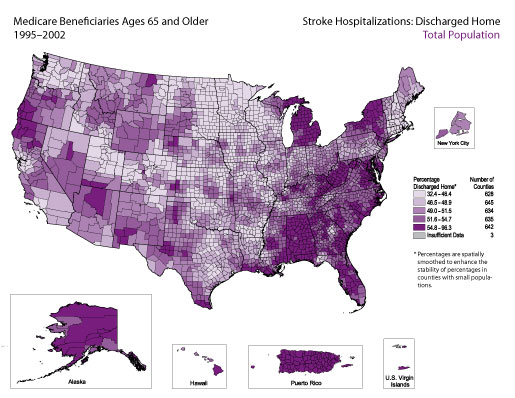
Overall, 51% of Medicare beneficiaries ages 65 and older who were hospitalized for stroke during 1995–2002 were discharged home. The frequency distribution indicates that for the majority of counties, the percentage discharged home was between 40% and 60%. Counties with the highest percentages (i.e., those in the top quintile, in which at least 54.8% of patients hospitalized for stroke were discharged home) were concentrated in parts of New York, Michigan, West Virginia, Alabama, Puerto Rico, and Alaska.
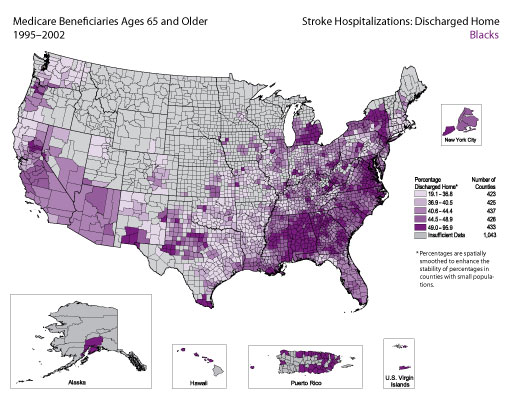
Among black Medicare beneficiaries ages 65 and older who were hospitalized for stroke, 45.2% were discharged home. The frequency distribution indicates that for the majority of counties, the percentage was between 30% and 52%. There did not appear to be a strong geographic pattern. Pockets of counties with the highest percentages (i.e., those in the top quintile, in which at least 49% of patients hospitalized for stroke were discharged home) were observed in New York, Michigan, Virginia, Georgia, Alabama, Mississippi, and Puerto Rico.
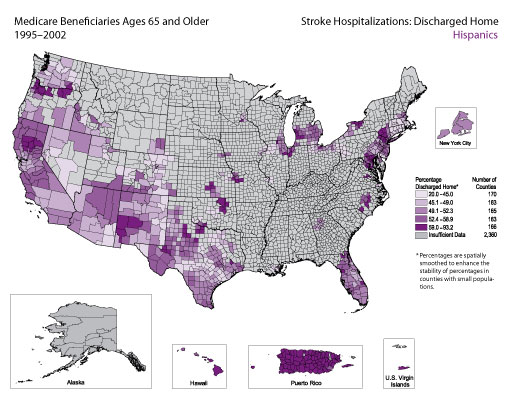
Among Hispanic Medicare beneficiaries ages 65 and older who were hospitalized for stroke, 57.6% were discharged home. The frequency distribution indicates that for the majority of counties, the percentage was between 40% and 60%. Counties with the highest percentages (i.e., those in the top quintile, in which at least 59% of patients hospitalized for stroke were discharged home) were concentrated in Puerto Rico and isolated pockets in New York, Oklahoma, Oregon, and California.
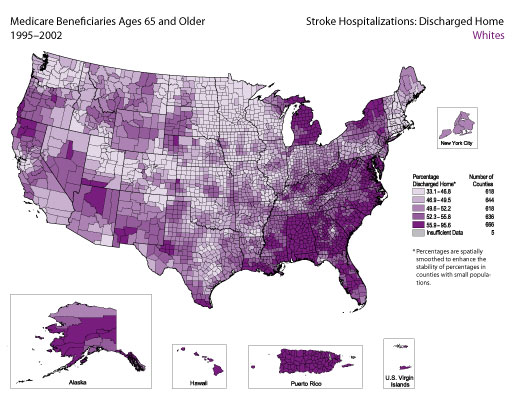
Among white Medicare beneficiaries ages 65 and older who were hospitalized for stroke, 51.6% were discharged home. The frequency distribution indicates that for the majority of counties, the percentage was between 40% and 60%. Counties with the highest percentages (i.e., those in the top quintile, in which at least 55.9% of patients hospitalized for stroke were discharged home) were concentrated in parts of New York, Michigan, West Virginia, Alabama, Puerto Rico, and the southeastern coastal states.
Stroke hospitalizations were defined as those for which the principal diagnosis on the Medicare hospital claim form was cerebrovascular disease, indicated by codes 430–434 and 436–438 according to the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM). Hospitalizations for which the principal diagnosis was transient ischemic attacks (ICD-9-CM code 435) were excluded.
For each map, the counties are categorized according to quintile; the darkest color represents counties with the highest percentages, and the lightest color represents counties with the lowest percentages. All county-level percentages have been spatially smoothed to enhance the stability in counties with small populations. Counties are categorized as having “insufficient data” if the sum of stroke hospitalizations in the index county plus the neighboring counties is less than 20, the Medicare population is less than 10, or the relative standard error of the estimated percentage is >30%. For more details, see Appendix B.
The frequency distribution in the bottom right corner of each map shows the range of percentages observed among counties on the corresponding map. The vertical dotted lines and the graded color bar along the x-axis illustrate the quintiles into which counties were divided on the basis of these percentages.
The quintiles do not always have equal numbers of counties because many counties have the same percentage of hospitalizations. For a detailed explanation of the methods, see Appendix B.
In the Medicare data sets, the accuracy of codes for Hispanic race and ethnicity is limited because these codes are not reported separately. For example, a person who is white and Hispanic is reported as either white or Hispanic. This reporting practice can result in misclassification of race and ethnicity. According to 1996 data, the probability that the racial/ethnic designation on Medicare claim forms is correct is 96.6% for whites and 95.5% for blacks, but only 19.4% for Hispanics. At the same time, the probability that a person identified as Hispanic in the Medicare data set is actually Hispanic is 98% (Arday SL, Arday DR, Monroe A, Zhang MD. HCFA’s racial and ethnic data: current accuracy and recent improvements. Health Care Financing Review 2000;21[4]:107–16). Together, these data suggest that Hispanics are underreported in the Medicare data sets and that this underreporting could introduce bias into the results presented here.
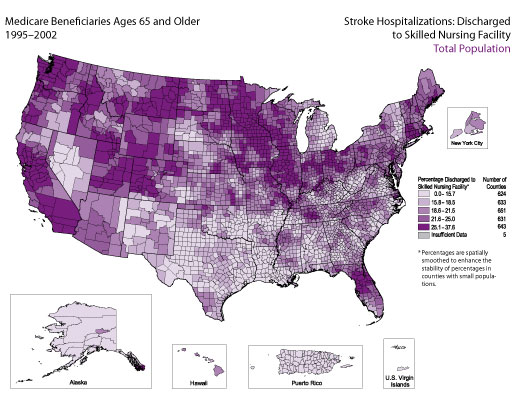
Overall, 21.1% of Medicare beneficiaries ages 65 and older hospitalized for stroke during 1995–2002 were discharged to a skilled nursing facility. The frequency distribution indicates that for the majority of counties, the percentage discharged to a skilled nursing facility was between 12% and 30%. Counties with the highest percentages (i.e., those in which at least 25.1% of patients hospitalized for stroke were discharged to a skilled nursing facility) were located primarily in the midwestern and western states.
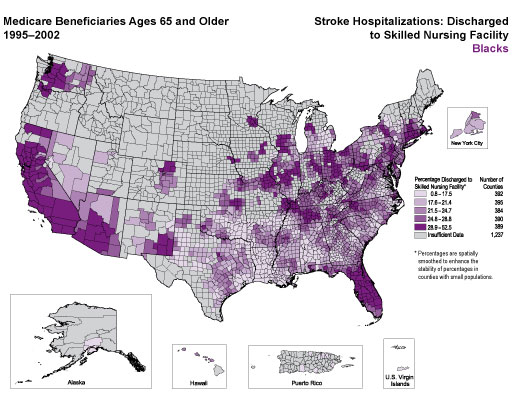
Among black Medicare beneficiaries ages 65 and older who were hospitalized for stroke, 22.3% were discharged to a skilled nursing facility. The frequency distribution indicates that for the majority of counties, the percentage was between 12% and 35%. There did not appear to be a strong geographic pattern. However, concentrations of counties with the highest percentages (i.e., those in which at least 28.9% of patients hospitalized for stroke were discharged to a skilled nursing facility) appeared to be concentrated along the Pacific Coast in parts of California, Arizona, and Washington; were scattered across parts of the Midwest and New England; and were found in Florida.
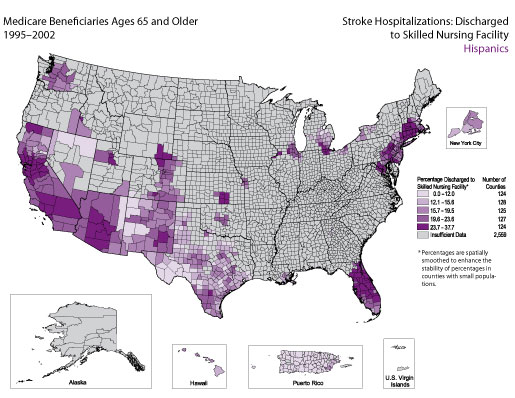
Among Hispanic Medicare beneficiaries ages 65 and older who were hospitalized for stroke, 15.7% were discharged to a skilled nursing facility. The frequency distribution indicates that for the majority of counties, the percentage was between 10% and 25%. Counties with the highest percentages (i.e., those in which at least 23.7% of patients hospitalized for stroke were discharged to a skilled nursing facility) were located primarily in California, Arizona, Florida, Massachusetts, and Connecticut.
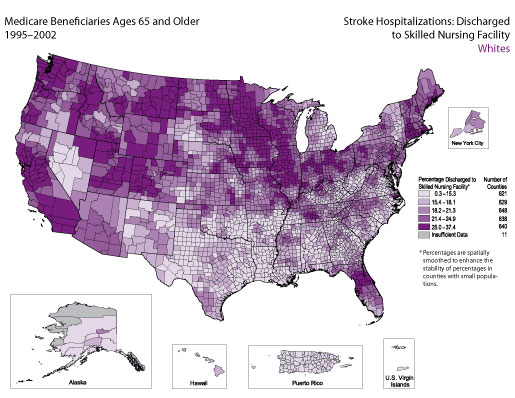
Among white Medicare beneficiaries ages 65 and older who were hospitalized for stroke, 21% were discharged to a skilled nursing facility. The frequency distribution indicates that for the majority of counties, the percentage was between 10% and 30%. Concentrations of counties with the highest percentages (i.e., those in which at least 25% of patients hospitalized for stroke were discharged to a skilled nursing facility) were found primarily in the midwestern and western states.
Stroke hospitalizations were defined as those for which the principal diagnosis on the Medicare hospital claim form was cerebrovascular disease, indicated by codes 430–434 and 436–438 according to the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM). Hospitalizations for which the principal diagnosis was transient ischemic attacks (ICD-9-CM code 435) were excluded.
For each map, the counties are categorized according to quintile; the darkest color represents counties with the highest percentages, and the lightest color represents counties with the lowest percentages. All county-level percentages have been spatially smoothed to enhance the stability in counties with small populations. Counties are categorized as having “insufficient data” if the sum of stroke hospitalizations in the index county plus the neighboring counties is less than 20, the Medicare population is less than 10, or the relative standard error of the estimated percentage is >30%. For more details, see Appendix B.
The frequency distribution in the bottom right corner of each map shows the range of percentages observed among counties on the corresponding map. The vertical dotted lines and the graded color bar along the x-axis illustrate the quintiles into which counties were divided on the basis of these percentages. The quintiles do not always have equal numbers of counties because many counties have the same percentage of hospitalizations. For a detailed explanation of the methods, see Appendix B.
Skilled nursing facilities are defined by Medicare as facilities that meet specific regulatory certification requirements and that primarily provide inpatient skilled nursing care and related services to patients who require medical, nursing, or rehabilitative services but do not provide the level of care or treatment available in a hospital.
In the Medicare data sets, the accuracy of codes for Hispanic race and ethnicity is limited because these codes are not reported separately. For example, a person who is white and Hispanic is reported as either white or Hispanic. This reporting practice can result in misclassification of race and ethnicity. According to 1996 data, the probability that the racial/ethnic designation on Medicare claim forms is correct is 96.6% for whites and 95.5% for blacks, but only 19.4% for Hispanics. At the same time, the probability that a person identified as Hispanic in the Medicare data set is actually Hispanic is 98% (Arday SL, Arday DR, Monroe A, Zhang MD. HCFA’s racial and ethnic data: current accuracy and recent improvements. Health Care Financing Review 2000;21[4]:107–16). Together, these data suggest that Hispanics are underreported in the Medicare data sets and that this underreporting could introduce bias into the results presented here.
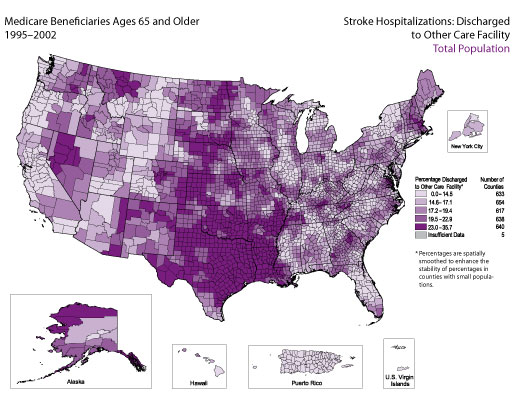
Overall, 17.6% of Medicare beneficiaries ages 65 and older were discharged to a health care facility that was not a skilled nursing facility. The frequency distribution indicates that for the majority of counties, the percentage discharged to a care facility other than a skilled nursing facility was between 12% and 28%. Counties with the highest percentages (i.e., those in which at least 23% of patients hospitalized for stroke were discharged to a health care facility other than a skilled nursing facility) were located mostly in Texas, Oklahoma, Arkansas, and Louisiana, as well as in parts of other states located along the central corridor of the United States.
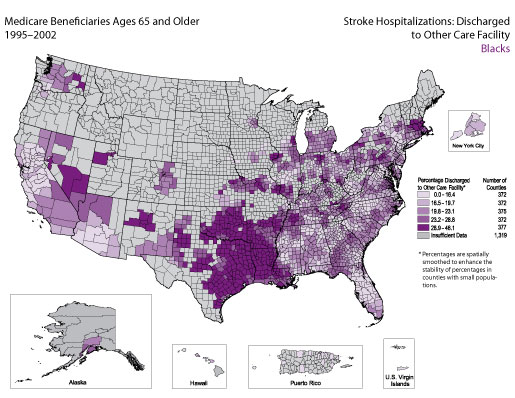
Among black Medicare beneficiaries ages 65 and older who were hospitalized for stroke, 21.6% were discharged to a health care facility that was not a skilled nursing facility. The frequency distribution indicates that for the majority of counties, the percentage was between 12% and 36%. Counties with the highest percentages (i.e., those in which at least 28.9% of patients hospitalized for stroke were discharged to a health care facility other than a skilled nursing facility) were located mostly in Texas, Oklahoma, Arkansas, Louisiana, and the central part of New Mexico.
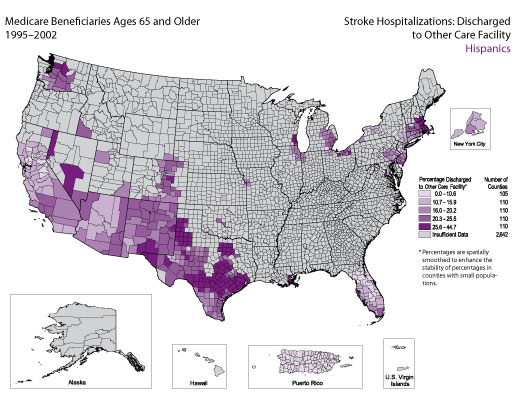
Among Hispanic Medicare beneficiaries ages 65 and older who were hospitalized for stroke, 15.8% were discharged to a health care facility that was not a skilled nursing facility. The frequency distribution indicates that for the majority of counties, the percentage was between 10% and 30%. Counties with the highest percentages (i.e., those in which at least 25.6% of patients hospitalized for stroke were discharged to a health care facility other than a skilled nursing facility) were located mostly in Texas.
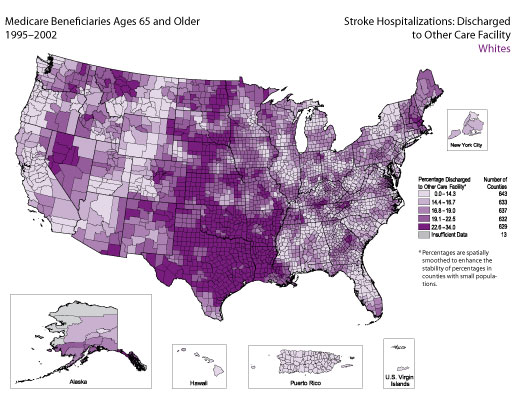
Among white Medicare beneficiaries ages 65 and older who were hospitalized for stroke, 17.1% were discharged to a health care facility that was not a skilled nursing facility. The frequency distribution indicates that for the majority of counties, the percentage was between 12% and 28%. Counties with the highest percentages (i.e., those in which at least 22.6% of patients hospitalized for stroke were discharged to a health care facility other than a skilled nursing facility) were located mostly in Texas, Oklahoma, Arkansas, and Louisiana, as well as in parts of other states located along the central corridor of the United States.
Stroke hospitalizations were defined as those for which the principal diagnosis on the Medicare hospital claim form was cerebrovascular disease, indicated by codes 430–434 and 436–438 according to the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM). Hospitalizations for which the principal diagnosis was transient ischemic attacks (ICD-9-CM code 435) were excluded.
For each map, the counties are categorized according to quintile; the darkest color represents counties with the highest percentages, and the lightest color represents counties with the lowest percentages. All county-level percentages have been spatially smoothed to enhance the stability in counties with small populations. Counties are categorized as having “insufficient data” if the sum of stroke hospitalizations in the index county plus the neighboring counties is less than 20, the Medicare population is less than 10, or the relative standard error of the estimated percentage is >30%. For more details, see Appendix B.
The frequency distribution in the bottom right corner of each map shows the range of percentages observed among counties on the corresponding map. The vertical dotted lines and the graded color bar along the x-axis illustrate the quintiles into which counties were divided on the basis of these percentages.
The quintiles do not always have equal numbers of counties because many counties have the same percentage of hospitalizations. For a detailed explanation of the methods, see Appendix B.
Care facilities other than skilled nursing facilities are defined by Medicare as intermediate care, short-term care, or other types of facilities.
In the Medicare data sets, the accuracy of codes for Hispanic race and ethnicity is limited because these codes are not reported separately. For example, a person who is white and Hispanic is reported as either white or Hispanic. This reporting practice can result in misclassification of race and ethnicity. According to 1996 data, the probability that the racial/ethnic designation on Medicare claim forms is correct is 96.6% for whites and 95.5% for blacks, but only 19.4% for Hispanics. At the same time, the probability that a person identified as Hispanic in the Medicare data set is actually Hispanic is 98% (Arday SL, Arday DR, Monroe A, Zhang MD. HCFA’s racial and ethnic data: current accuracy and recent improvements. Health Care Financing Review 2000;21[4]:107–16). Together, these data suggest that Hispanics are underreported in the Medicare data sets and that this underreporting could introduce bias into the results presented here.
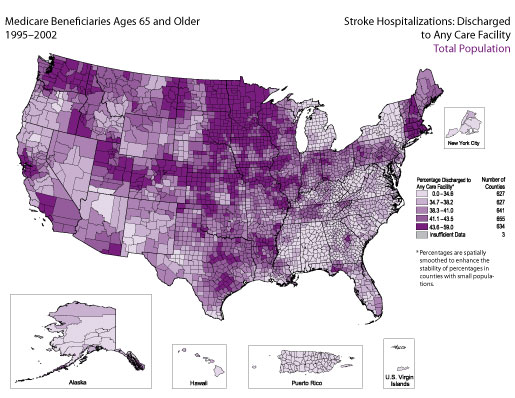
Overall, 38.7% of Medicare beneficiaries ages 65 and older during 1995–2002 were discharged to some type of health care facility (e.g., skilled nursing facility, intermediate care facility, other short-term general hospital, other type of institution). The frequency distribution indicates that for the majority of counties, the percentage discharged to any care facility was between 30% and 50%. Counties with the highest percentages (i.e., those in which at least 43.6% of patients hospitalized for stroke were discharged to any type of health care facility) were located primarily in the north-central section of the United States, New England, and parts of the West.
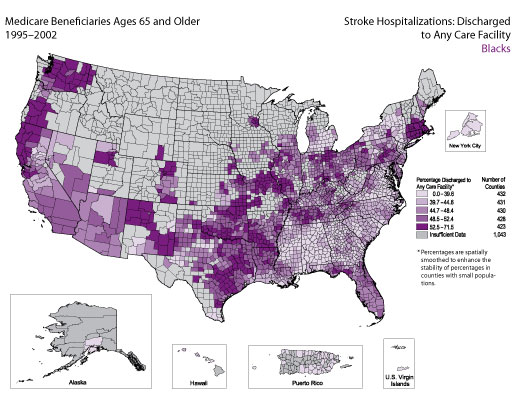
Among black Medicare beneficiaries ages 65 and older who were hospitalized for stroke, 43.9% were discharged to some type of health care facility (e.g., skilled nursing facility, intermediate care facility, other short-term general hospital, other type of institution). The frequency distribution indicates that for the majority of counties, the percentage was between 35% and 56%. Counties with the highest percentages (i.e., those in which at least 52.5% of patients hospitalized for stroke were discharged to any type of health care facility) were located primarily in Connecticut, Massachusetts, Missouri, Arkansas, Oklahoma, Texas, New Mexico, Washington, western Oregon, and northern California.
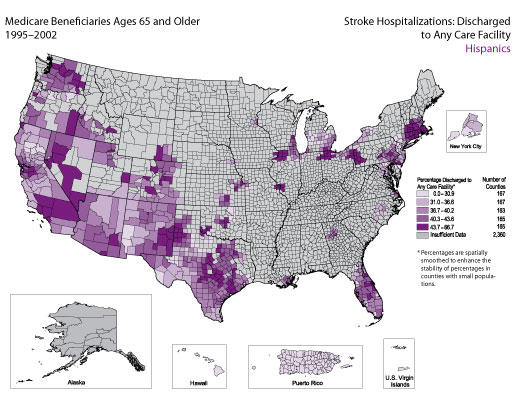
Among Hispanic Medicare beneficiaries ages 65 and older who were hospitalized for stroke, 31.5% were discharged to some type of health care facility (e.g., skilled nursing facility, intermediate care facility, other short-term general hospital, other type of institution). The frequency distribution indicates that for the majority of counties, the percentage was between 30% and 46%. Pockets of counties with the highest percentages (i.e., those in which at least 43.7% of patients hospitalized for stroke were discharged to any type of health care facility) were located primarily in Massachusetts, Connecticut, Pennsylvania, Ohio, Illinois, Texas, New Mexico, Nevada, California, and Washington.
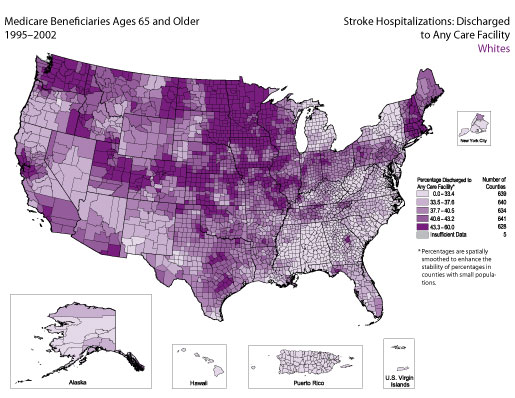
Among white Medicare beneficiaries ages 65 and older who were hospitalized for stroke, 38.1% were discharged to some type of health care facility (e.g., skilled nursing facility, intermediate care facility, other short-term general hospital, other type of institution). The frequency distribution indicates that for the majority of counties, the percentage was between 30% and 48%. Counties with the highest percentages (i.e., those in which at least 43.3% of patients hospitalized for stroke were discharged to any type of health care facility) were located primarily in the north-central section of the United States, New England, and parts of the West.
Stroke hospitalizations were defined as those for which the principal diagnosis on the Medicare hospital claim form was cerebrovascular disease, indicated by codes 430–434 and 436–438 according to the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM). Hospitalizations for which the principal diagnosis was transient ischemic attacks (ICD-9-CM code 435) were excluded.
For each map, the counties are categorized according to quintile; the darkest color represents counties with the highest percentages, and the lightest color represents counties with the lowest percentages. All county-level percentages have been spatially smoothed to enhance the stability in counties with small populations. Counties are categorized as having “insufficient data” if the sum of stroke hospitalizations in the index county plus the neighboring counties is less than 20, the Medicare population is less than 10, or the relative standard error of the estimated percentage is >30%. For more details, see Appendix B.
The frequency distribution in the bottom right corner of each map shows the range of percentages observed among counties on the corresponding map. The vertical dotted lines and the graded color bar along the x-axis illustrate the quintiles into which counties were divided on the basis of these percentages. The quintiles do not always have equal numbers of counties because many counties have the same percentage of hospitalizations. For a detailed explanation of the methods, see Appendix B.
In the Medicare data sets, the accuracy of codes for Hispanic race and ethnicity is limited because these codes are not reported separately. For example, a person who is white and Hispanic is reported as either white or Hispanic. This reporting practice can result in misclassification of race and ethnicity. According to 1996 data, the probability that the racial/ethnic designation on Medicare claim forms is correct is 96.6% for whites and 95.5% for blacks, but only 19.4% for Hispanics. At the same time, the probability that a person identified as Hispanic in the Medicare data set is actually Hispanic is 98% (Arday SL, Arday DR, Monroe A, Zhang MD. HCFA’s racial and ethnic data: current accuracy and recent improvements. Health Care Financing Review 2000;21[4]:107–16). Together, these data suggest that Hispanics are underreported in the Medicare data sets and that this underreporting could introduce bias into the results presented here.
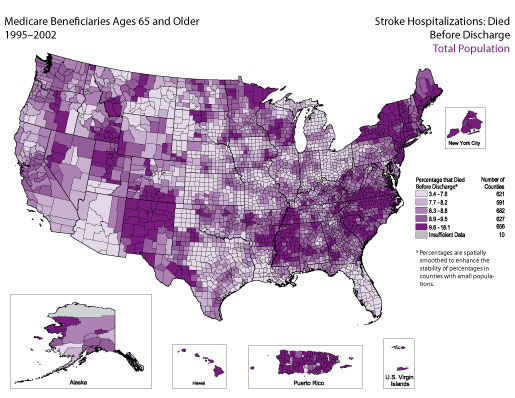
Among Medicare beneficiaries ages 65 and older who were hospitalized for stroke during 1995–2002, 8.8% died before they were discharged. The frequency distribution indicates that for the majority of counties, the percentage of deaths before discharge was between 6% and 11%. Counties with the highest percentages (i.e., those in which at least 9.6% of patients hospitalized for stroke died before being discharged) were scattered throughout the United States, with concentrations in the Northeast, New Mexico, Puerto Rico, parts of the Southeast, and parts of the West.
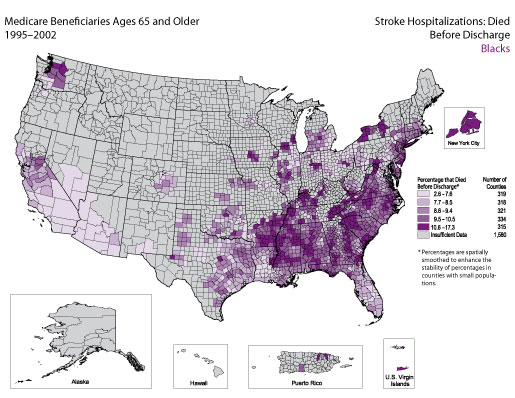
Among black Medicare beneficiaries ages 65 and older who were hospitalized for stroke, 9% died before they were discharged. The frequency distribution indicates that for the majority of counties, the percentage was between 6% and 13%. There did not appear to be a strong geographic pattern. However, pockets of counties with the highest percentages (i.e., those in which at least 10.6% of patients hospitalized for stroke died before being discharged) were observed in New York, South Carolina, Tennessee, Alabama, Mississippi, and Arkansas.
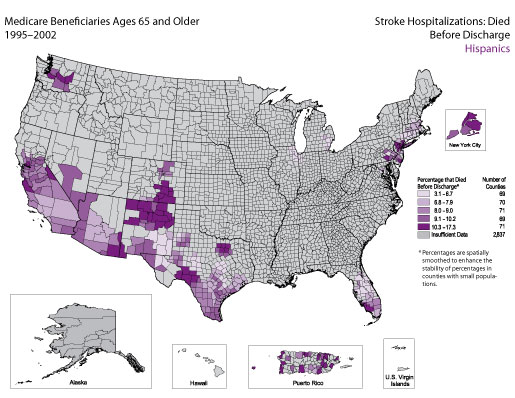
Among Hispanic Medicare beneficiaries ages 65 and older who were hospitalized for stroke, 9.1% died before they were discharged. The frequency distribution indicates that for the majority of counties, the percentage was between 5% and 12%. There did not appear to be a strong geographic pattern. However, pockets of counties with the highest percentages (i.e., those in which at least 10.3% of patients hospitalized for stroke died before being discharged) were found primarily in the Southwest.
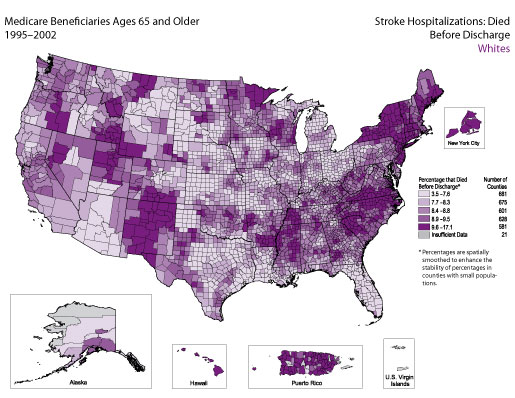
Among white Medicare beneficiaries ages 65 and older who were hospitalized for stroke, 8.7% died before they were discharged. The frequency distribution indicates that for the majority of counties, the percentage was between 7% and 11%. There did not appear to be a strong geographic pattern. However, pockets of counties with the highest percentages (i.e., those in which at least 9.6% of patients hospitalized for stroke died before being discharged) were located in the Northeast, New Mexico, Puerto Rico, parts of the Southeast, and parts of the West.
Stroke hospitalizations were defined as those for which the principal diagnosis on the Medicare hospital claim form was cerebrovascular disease, indicated by codes 430–434 and 436–438 according to the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM). Hospitalizations for which the principal diagnosis was transient ischemic attacks (ICD-9-CM code 435) were excluded.
For each map, the counties are categorized according to quintile; the darkest color represents counties with the highest percentages, and the lightest color represents counties with the lowest percentages. All county-level percentages have been spatially smoothed to enhance the stability in counties with small populations. Counties are categorized as having “insufficient data” if the sum of stroke hospitalizations in the index county plus the neighboring counties is less than 20, the Medicare population is less than 10, or the relative standard error of the estimated percentage is >30%. For more details, see Appendix B.
The frequency distribution in the bottom right corner of each map shows the range of percentages observed among counties on the corresponding map. The vertical dotted lines and the graded color bar along the x-axis illustrate the quintiles into which counties were divided on the basis of these percentages.
The quintiles do not always have equal numbers of counties because many counties have the same percentage of hospitalizations. For a detailed explanation of the methods, see Appendix B.
In the Medicare data sets, the accuracy of codes for Hispanic race and ethnicity is limited because these codes are not reported separately. For example, a person who is white and Hispanic is reported as either white or Hispanic. This reporting practice can result in misclassification of race and ethnicity. According to 1996 data, the probability that the racial/ethnic designation on Medicare claim forms is correct is 96.6% for whites and 95.5% for blacks, but only 19.4% for Hispanics. At the same time, the probability that a person identified as Hispanic in the Medicare data set is actually Hispanic is 98% (Arday SL, Arday DR, Monroe A, Zhang MD. HCFA’s racial and ethnic data: current accuracy and recent improvements. Health Care Financing Review 2000;21[4]:107–16). Together, these data suggest that Hispanics are underreported in the Medicare data sets and that this underreporting could introduce bias into the results presented here.
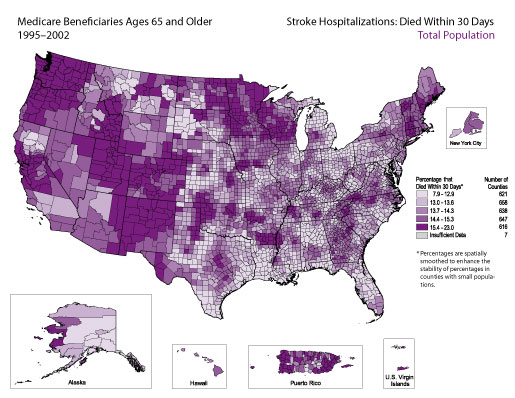
Overall, 13.9% of Medicare beneficiaries ages 65 and older who were hospitalized for stroke during 1995–2002 died within 30 days of being admitted to the hospital. The frequency distribution indicates that for the majority of counties, the percentage was between 12% and 17%. There did not appear to be a strong geographic pattern. However, counties with the highest percentages (i.e., those in which at least 15.4% of patients hospitalized for stroke died within 30 days) were located primarily in the western half of the United States and Puerto Rico.
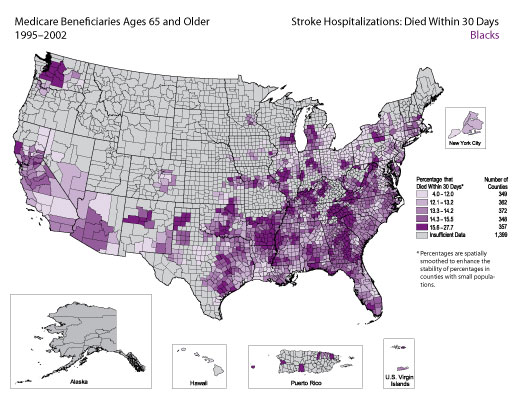
Among black Medicare beneficiaries ages 65 and older who were hospitalized for stroke, 12.9% died within 30 days of being admitted to the hospital. The frequency distribution indicates that for the majority of counties, the percentage was between 10% and 18%. Pockets of counties with the highest percentages (i.e., those in which at least 15.6% of patients hospitalized for stroke died within 30 days) were located primarily in parts of the Southeast, the Delta Region, and Washington.
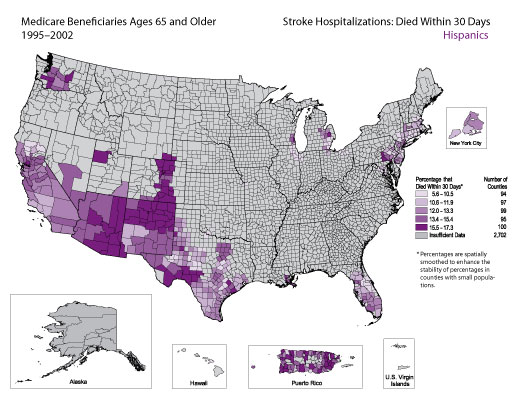
Among Hispanic Medicare beneficiaries ages 65 and older who were hospitalized for stroke, 13% died within 30 days of being admitted to the hospital. The frequency distribution indicates that for the majority of counties, the percentage was between 9% and 20%. There did not appear to be a strong geographic pattern. However, counties with the highest percentages (i.e., those in which at least 15.5% of patients hospitalized for stroke died within 30 days) were located mainly in Arizona, New Mexico, Colorado, and Puerto Rico.
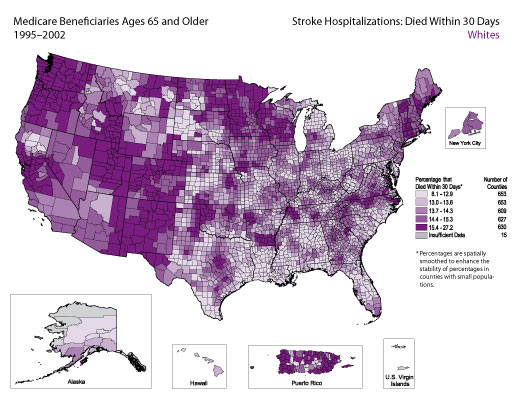
Among white Medicare beneficiaries ages 65 and older who were hospitalized for stroke, 13.9% died within 30 days of being admitted to the hospital. The frequency distribution indicates that for the majority of counties, the percentage was between 12% and 17%. There did not appear to be a strong geographic pattern. However, counties with the highest percentages (i.e., those in which at least 15.4% of patients hospitalized for stroke died within 30 days) were located primarily in the western half of the United States and Puerto Rico.
Stroke hospitalizations were defined as those for which the principal diagnosis on the Medicare hospital claim form was cerebrovascular disease, indicated by codes 430–434 and 436–438 according to the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM). Hospitalizations for which the principal diagnosis was transient ischemic attacks (ICD-9-CM code 435) were excluded.
For each map, the counties are categorized according to quintile; the darkest color represents counties with the highest percentages, and the lightest color represents counties with the lowest percentages. All county-level percentages have been spatially smoothed to enhance the stability in counties with small populations. Counties are categorized as having “insufficient data” if the sum of stroke hospitalizations in the index county plus the neighboring counties is less than 20, the Medicare population is less than 10, or the relative standard error of the estimated percentage is >30%. For more details, see Appendix B.
The frequency distribution in the bottom right corner of each map shows the range of percentages observed among counties on the corresponding map. The vertical dotted lines and the graded color bar along the x-axis illustrate the quintiles into which counties were divided on the basis of these percentages.
The quintiles do not always have equal numbers of counties because many counties have the same percentage of hospitalizations. For a detailed explanation of the methods, see Appendix B.
In the Medicare data sets, the accuracy of codes for Hispanic race and ethnicity is limited because these codes are not reported separately. For example, a person who is white and Hispanic is reported as either white or Hispanic. This reporting practice can result in misclassification of race and ethnicity. According to 1996 data, the probability that the racial/ethnic designation on Medicare claim forms is correct is 96.6% for whites and 95.5% for blacks, but only 19.4% for Hispanics. At the same time, the probability that a person identified as Hispanic in the Medicare data set is actually Hispanic is 98% (Arday SL, Arday DR, Monroe A, Zhang MD. HCFA’s racial and ethnic data: current accuracy and recent improvements. Health Care Financing Review 2000;21[4]:107–16). Together, these data suggest that Hispanics are underreported in the Medicare data sets and that this underreporting could introduce bias into the results presented here.
| Back to Top |
Page last reviewed: April 9, 2008
Page last modified: April 9, 2008
Content source: Division for Heart Disease and Stroke
Prevention,
National Center for Chronic Disease Prevention and
Health Promotion
|
|
|
||||||||||||
|
 Section
Three: Maps of Stroke
Hospitalizations by Discharge Status and Race/Ethnicity
Section
Three: Maps of Stroke
Hospitalizations by Discharge Status and Race/Ethnicity