


Vitamin E Acetate in Bronchoalveolar-Lavage Fluid Associated with EVALI
List of authors.
A list of the members of the Lung Injury Response Laboratory Working Group is provided in the Supplementary Appendix, available at NEJM.org.
Drs. Blount and Karwowski contributed equally to this article.
Abstract
Background
The causative agents for the current national outbreak of electronic-cigarette, or vaping, product use–associated lung injury (EVALI) have not been established. Detection of toxicants in bronchoalveolar-lavage (BAL) fluid from patients with EVALI can provide direct information on exposure within the lung.
Methods
BAL fluids were collected from 51 patients with EVALI in 16 states and from 99 healthy participants who were part of an ongoing study of smoking involving nonsmokers, exclusive users of e-cigarettes or vaping products, and exclusive cigarette smokers that was initiated in 2015. Using the BAL fluid, we performed isotope dilution mass spectrometry to measure several priority toxicants: vitamin E acetate, plant oils, medium-chain triglyceride oil, coconut oil, petroleum distillates, and diluent terpenes.
Results
State and local health departments assigned EVALI case status as confirmed for 25 patients and as probable for 26 patients. Vitamin E acetate was identified in BAL fluid obtained from 48 of 51 case patients (94%) in 16 states but not in such fluid obtained from the healthy comparator group. No other priority toxicants were found in BAL fluid from the case patients or the comparator group, except for coconut oil and limonene, which were found in 1 patient each. Among the case patients for whom laboratory or epidemiologic data were available, 47 of 50 (94%) had detectable tetrahydrocannabinol (THC) or its metabolites in BAL fluid or had reported vaping THC products in the 90 days before the onset of illness. Nicotine or its metabolites were detected in 30 of 47 of the case patients (64%).
Conclusions
Vitamin E acetate was associated with EVALI in a convenience sample of 51 patients in 16 states across the United States. (Funded by the National Cancer Institute and others.)

Methods
Case Definitions
 Case Definitions for Patients with EVALI.
Case Definitions for Patients with EVALI. All case-associated BAL fluid samples were obtained from patients who met EVALI case definitions of the CDC, as determined by state or local health officials (Table 1).13
Biospecimen Collection from Case and Comparator Participants
EVALI Case Patients
BAL fluid was obtained by clinical teams caring for hospitalized patients. The decision to obtain BAL fluid was made by the clinical team on a case-by-case basis to guide clinical management decisions. The CDC requested the assistance of state health departments in acquiring BAL fluid samples. If a patient qualified as having a probable or confirmed diagnosis of EVALI, then BAL fluid was accepted by the CDC for analysis. No other inclusion or exclusion criteria were applied.
The small volumes of BAL fluid in some samples required prioritizing analyses. Vitamin E acetate was prioritized first, followed by dipalmitoylphosphatidylcholine (DPPC), cannabinoids, and then other toxicants. Insufficient clinical data were available to estimate the time between the last use of an e-cigarette product and the bronchoscopy to obtain BAL fluid. Sample collection was conducted according to the routine clinical processes at each institution and was not standardized. Samples were refrigerated or frozen after collection and shipped to the CDC on dry ice. Human-subjects research review was conducted by the CDC, which determined that this information collection did not meet the regulatory definition of research under 45 CFR 46.102(d) and was therefore determined to be a nonresearch public health response activity.
Healthy Comparator Group
BAL fluid had been previously obtained from 99 participants that included nonusers, current exclusive users of nicotine-containing e-cigarette products, and current exclusive cigarette smokers recruited through local media and participant registries at Ohio State University14,15 as part of a tobacco-product study unrelated to the ongoing EVALI investigation. The participants were between the ages of 21 and 45 years and had no major clinical illness or increased risk from bronchoscopy. Inclusion and exclusion criteria for the 52 nonusers, the 18 exclusive users of nicotine-containing e-cigarette products, and the 29 exclusive cigarette smokers have been reported previously.15 The negative smoking status for both the nonusers and users of e-cigarette products was confirmed biochemically by urinary anatabine testing.15 After collection, BAL fluids were transported to the laboratory on wet ice and processed within 30 minutes by centrifugation; cell pellets and supernatant were immediately placed in storage at −80°C.
All the participants provided written informed consent before participation. The tobacco-product study involving healthy participants was approved by the institutional review board at Ohio State University.16
Laboratory Analysis
Investigators at the CDC established a list of priority toxicants to measure in BAL fluid: vitamin E acetate, plant oils (identified by measuring long-chain triglycerides), medium-chain triglyceride oil, coconut oil (identified by measuring medium-chain triglycerides), petroleum distillates, and diluent terpenes (including limonene). For these toxicants in BAL fluid, the CDC developed and validated analytic methods that were evaluated for accuracy, precision, analytic sensitivity, and analytic specificity. These methods used isotope dilution mass spectrometry and provided results that met or exceeded the quality criteria of the Clinical Laboratory Improvement Amendments.
The analytic limit of detection (LOD) was calculated on the basis of repeated measures to estimate the standard deviation at zero concentration.17 Results higher than the LOD are reported as positive, and results lower than the LOD are reported as negative. The methods to measure each of the potential toxicants of concern — along with THC and nicotine parent compounds and metabolites and DPPC — are described in Table S1 in the Supplementary Appendix, available with the full text of this article at NEJM.org.18-20 All case and comparator samples of BAL fluid had detectable levels of DPPC, the main phospholipid of lung surfactant; DPPC was used as a marker to indicate that the BAL fluid contained pulmonary epithelial-lining fluid and thus was considered to be an adequate sample for testing.
Data Analysis
Results are presented as percentages of persons in whom BAL fluid samples tested positive for the measured toxicant or metabolite biomarker. Because of the limited volume of BAL fluid, results for all analytes were not available for all participants. Since the analysis of vitamin E acetate was prioritized, results regarding vitamin E acetate are reported for all the participants. Denominators reflect the actual number of participants for whom samples were tested for each analyte.
Results
From August through December 2019, public health laboratories and health departments in 16 states provided BAL fluid samples obtained from 51 patients, including those in Arizona (2), Arkansas (2), California (4), Connecticut (1), Hawaii (1), Illinois (12), Indiana (1), Maryland (4), Michigan (2), Minnesota (5), Missouri (1), North Carolina (2), Texas (2), Utah (3), West Virginia (1), and Wisconsin (8). BAL fluid was acquired from 3 patients with EVALI who later died.
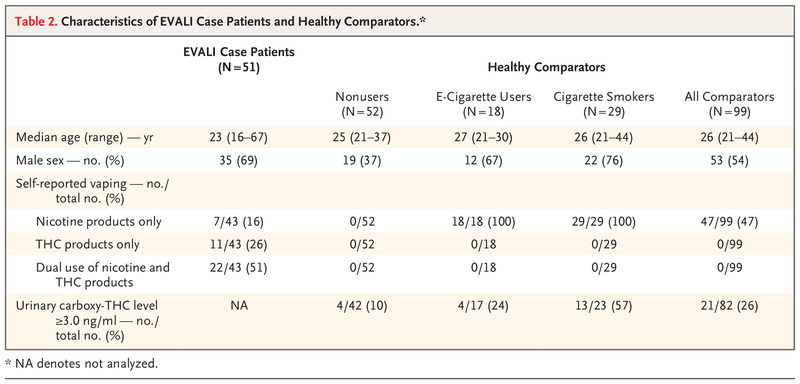 Characteristics of EVALI Case Patients and Healthy Comparators.
Characteristics of EVALI Case Patients and Healthy Comparators. The age and sex of the 51 patients for whom BAL fluid was available were consistent with national data regarding patients with EVALI.7 The median age of the patients was 23 years, and 69% were male (Table 2). Among the patients for whom information was available, 77% reported the use of THC-containing products, 67% reported the use of nicotine-containing products, and 51% reported the use of both types of products. Health departments assigned and reported case status for all patients; of these patients, 25 had been classified as having confirmed EVALI and 26 as having probable EVALI.
Samples from healthy study participants were collected from 2016 through 2019, with 90 of the 99 samples obtained before 2019. The mean (±SD) age in years was 25.4±3.6 for nonusers, 26.5±2.7 for exclusive e-cigarette users, and 27.3±4.9 for exclusive cigarette smokers. Men made up 37%, 67%, and 76%, respectively, of the subgroups. Among the healthy participants, urine THC biomarkers were positive in 25.6%, whereas BAL fluid THC biomarkers were positive in 5.1%. The higher sensitivity of urine than of BAL fluid for the detection of THC biomarkers has been reported previously.21 The prevalence of positive urine THC biomarkers was highest among the participants who reported exclusive cigarette smoking (13 of 23 [57%]). Nicotine or its metabolites were detected in 52% of BAL fluids from the healthy participants. All the BAL fluid samples from this group were negative for all priority toxicants: vitamin E acetate, plant oils, medium-chain triglyceride oil, coconut oil, petroleum distillates, and diluent terpenes.
 Frequency of Detection of Priority Toxicants in EVALI Case Patients and in Healthy Comparators.
Frequency of Detection of Priority Toxicants in EVALI Case Patients and in Healthy Comparators.  Exposure History and Clinical Characteristics of Three Patients with Probable Diagnosis of EVALI without Evidence of Vitamin E Acetate in BAL Fluid.
Exposure History and Clinical Characteristics of Three Patients with Probable Diagnosis of EVALI without Evidence of Vitamin E Acetate in BAL Fluid. Among the patients with EVALI, vitamin E acetate was detected in BAL fluid samples from 48 of 51 (94%) (Table 3). In 1 patient, BAL fluid had detectable levels of coconut oil in addition to vitamin E acetate; in another patient, BAL fluid contained limonene (a diluent terpene) with no detectable vitamin E acetate or THC. Samples from all the other patients were negative for the other priority toxicants: plant oils, medium-chain triglyceride oil, coconut oil, petroleum distillates, and diluent terpenes. Table 4 provides a clinical description of the 3 patients with EVALI who had no detectable vitamin E acetate; all of these 3 patients were classified as having probable cases. THC or its metabolites were detected in BAL fluid samples from 40 of 47 patients (85%) with EVALI. A total of 9 of 11 patients who reported no use of THC-containing e-cigarette products in the 90 days before the onset of illness had detectable THC or its metabolites in their BAL fluid. Among the patients who had available laboratory data or who reported product use, 47 of 50 (94%) had detectable THC or its metabolites in BAL fluid or reported vaping THC products in the 90 days before the onset of illness. Nicotine or its metabolites were detected in 30 of 47 (64%) BAL fluid samples from case patients.
Discussion
In our study, the detection of vitamin E acetate in BAL fluid in most of the patients with EVALI provides evidence that e-cigarette, or vaping, products can deliver vitamin E acetate to respiratory epithelial-lining fluid, the presumed site of injury in the lung. In this convenience sample, the finding that 48 of 51 patients with lung injury had vitamin E acetate in their BAL fluid is noteworthy. By contrast, vitamin E acetate was not detected in any BAL fluid collected from 99 healthy participants, including 18 e-cigarette users. In addition, the absence of other toxicants (plant oils, medium-chain triglyceride oil, coconut oil, petroleum distillates, and diluent terpenes) in BAL fluids from nearly all patients with EVALI provides evidence against the role of any of these toxicants as a primary cause of EVALI. Whether limonene or coconut oil (found in the BAL fluid of 1 patient each) may have some toxicologic effect is unclear.
Vitamin E acetate was not detected in the BAL fluid obtained from three patients with probable EVALI. Since EVALI is a diagnosis of exclusion for which there is no confirmatory diagnostic test, we could not confirm case status for these three patients. The EVALI case definition is intentionally sensitive, which raises the likelihood that a patient’s illness could be misattributed to EVALI. The alternative diagnoses that are listed in Table 4 could reasonably explain the lung injury in these patients. Of note, the two patients who were successfully interviewed by public health officials denied vaping THC products. Reliable information on the time interval from the last use of an e-cigarette product until bronchoscopy is not available, so we cannot assess the likelihood that vitamin E acetate may have already been cleared from the lung in these patients. The detection of vitamin E acetate and other oils can be impaired by inadequate mixing of BAL fluid. Because BAL fluid was collected and processed in the local hospital setting according to its own protocols, we could not confirm that samples were adequately mixed. Patient 2 (as described in Table 4) reported the daily use of flavored nicotine products and had positive results for limonene (which is found in flavored nicotine solutions) in BAL fluid. Whether limonene has a toxicologic effect is unclear.22,23
Vitamin E acetate is commonly used as a dietary supplement and in skin creams. It is common in multivitamins and is enzymatically cleaved to vitamin E during absorption.24,25 Although the ingestion and dermal application of vitamin E acetate have not generally been associated with adverse health effects, the safety of inhaling vitamin E acetate has received little attention. Vitamin E acetate is the ester of vitamin E (α-tocopherol) and acetic acid. The structure shows a long aliphatic tail that can penetrate a layer of surfactant to align the molecule in parallel with phospholipids26 (Fig. S1). Phosphatidylcholines undergo transition from a gel to a liquid crystalline phase when exposed to increasing amounts of tocopherols, such as vitamin E acetate.26,27 Transitioning to a liquid crystalline phase25 would cause the surfactant to lose its ability to maintain the surface tension that is necessary to support respiration in the lung,26,28,29 thus providing a possible mechanism by which vitamin E acetate could cause respiratory dysfunction.
Another potential harmful effect of vitamin E acetate that may contribute to lung injury occurs when it is heated in e-cigarette products. Heating vitamin E acetate in these devices may create ketene by splitting off the acetate group from some or all of the vitamin E acetate.30 Ketene is a reactive compound that has the potential to be a lung irritant, depending on concentration. The CDC is currently examining ways to quantify ketene and its effects in BAL fluid.
Data that have been reported to date indicate that vitamin E acetate in the supply of THC-containing products and use among patients with EVALI aligns with the timing of the 2019 EVALI outbreak. In Minnesota, 10 of 10 products seized by law enforcement during 2018, before the EVALI outbreak, did not contain vitamin E acetate, whereas 20 of 20 THC-containing products seized by law enforcement during September 2019, at the peak of the outbreak, contained vitamin E acetate.31 This finding is consistent with laboratory measurements and trade websites, which suggests that the addition of vitamin E acetate to product fluid began to appear in the illicit market in late 2018 or early 2019 and gained popularity in 2019.
Pure THC oil has a viscosity like that of vitamin E acetate. Cutting THC oil with vitamin E acetate has been reported to be common in the illicit market.9-11 The FDA reports that most case-associated THC product fluids contain vitamin E acetate, at an average concentration of 50% by weight, ranging from 23 to 88%.8 By contrast, the FDA detected no vitamin E acetate in 197 case-associated nicotine products analyzed to date. The viscosity of vitamin E acetate makes it undesirable as an additive to nicotine solutions; the propylene glycol and vegetable glycerin in nicotine solutions create a fluid with a much lower viscosity than that of vitamin E acetate.
Additional studies (including studies in animals) are in progress to examine the respiratory effects of inhaling aerosolized vitamin E acetate and will provide information on whether vitamin E acetate in isolation causes lung injury.32 Research analyzing the aerosol and gases generated by case-associated product fluids is ongoing.
This study has several limitations. First, it is possible that vitamin E acetate may be a marker for exposure to alternative toxicants. Such an alternative toxicant would need to meet at least three criteria: correlate with the presence of vitamin E acetate in BAL fluid, be in widespread use across the United States, and have been added to THC product fluids in 2019 or substantially increased in concentration in 2019 to match the timing of the outbreak. We have not been able to identify a toxicant that meets these three requirements but continue to study this possibility. Second, the contribution to injury of aerosol constituents formed from the heating of vitamin E acetate, especially at higher voltages, requires further examination. Until aerosolized constituents are better characterized, it is possible that one or more of them could act alone or synergistically with other compounds such as vitamin E acetate to increase the risk of EVALI. Third, sample collection was performed as part of routine clinical care and thus was not standardized. Fourth, the timing and burden of exposure to the potential toxicants in relation to the BAL sample acquisition could not be assessed. Finally, this study reports data for case patients and healthy comparators from an independent cross-sectional study, which limits insights because samples were collected at a single point in time, and the possibility of unknown confounding remains.
Vitamin E acetate may play a role in EVALI, a conclusion supported by the high detection rate of vitamin E acetate in BAL fluid from case patients who live in 16 states across the United States and the absence of vitamin E acetate in samples obtained from a healthy comparison group, by the absence of other priority toxicants in nearly all BAL fluid samples from case patients, by a biologically plausible mechanism for lung injury associated with vitamin E acetate, and by the temporal alignment between EVALI and the use of vitamin E acetate in the illicit marketplace. Results from studies in animals can provide information on whether exposure to vitamin E acetate alone can directly cause the lung injury seen in patients with EVALI.
Supplementary Material
References (32)
1. Centers for Disease Control and Prevention. Outbreak of lung injury associated with e-cigarette use, or vaping. December 12, 2019 (https://www.cdc.gov/tobacco/basic_information/e-cigarettes/severe-lung-disease.html?s_cid=osh-stu-home-spotlight-006).
2. Siegel DA, Jatlaoui TC, Koumans EH, et al. Update: interim guidance for health care providers evaluating and caring for patients with suspected e-cigarette, or vaping, product use associated lung Injury — United States, October 2019. Am J Transplant 2019;19:3420-3428.
3. Lozier MJ, Wallace B, Anderson K, et al. Update: demographic, product, and substance-use characteristics of hospitalized patients in a nationwide outbreak of e-cigarette, or vaping, product use-associated lung injuries — United States, December 2019. MMWR Morb Mortal Wkly Rep 2019;68:1142-1148.
4. Henry TS, Kligerman SJ, Raptis CA, Mann H, Sechrist JW, Kanne JP. Imaging findings of vaping-associated lung injury. AJR Am J Roentgenol 2019 October 8 (Epub ahead of print).
5. Butt YM, Smith ML, Tazelaar HD, et al. Pathology of vaping-associated lung injury. N Engl J Med 2019;381:1780-1781.
6. New York State Department of Health. New York State Department of Health announces update on investigation into vaping-associated pulmonary illnesses: department warns against use of black market vaping products: lab test results show high levels of vitamin E acetate, now focus of investigation. September 5, 2019 (https://www.health.ny.gov/press/releases/2019/2019-09-05_vaping.htm).
7. Moritz ED, Zapata LB, Lekiachvili A, et al. Update: characteristics of patients in a national outbreak of e-cigarette, or vaping, product use-associated lung injuries — United States, October 2019. MMWR Morb Mortal Wkly Rep 2019;68:985-989.
8. Food and Drug Administration. Lung illnesses associated with use of vaping products: information for the public, FDA actions, and recommendations. October 4, 2019 (https://www.fda.gov/news-events/public-health-focus/lung-illnesses-associated-use-vaping-products#Analysis).
9. Downs D. Vape pen lung injury: here’s what you need to know. December 12, 2019 (https://www.leafly.com/news/health/vape-pen-lung-disease-advice-consumers).
10. Downs D, Howard D, Barcott B. Journey of a tainted vape cartridge: from China’s labs to your lungs. Leafly. September 24, 2019 (https://www.leafly.com/news/politics/vape-pen-injury-supply-chain-investigation-leafly).
11. Eisenberg Z, Moy D, Lam V, Cheng C, Richard J, Burack B. Contaminant analysis of illicit vs regulated market extracts. San Francisco: Anresco Laboratories, October 26, 2019 (https://cannabis.anresco.com/analysis-of-illicit-vs-regulated-market-extracts).
12. Blount BC, Karwowski MP, Morel-Espinosa M, et al. Evaluation of bronchoalveolar lavage fluid from patients in an outbreak of e-cigarette, or vaping, product use–associated lung injury — 10 states, August–October 2019. MMWR Morb Mortal Wkly Rep 2019;68:1040-1041.
13. Centers for Disease Control and Prevention. Smoking and tobacco use: for state and local health departments. December 12, 2019 (https://www.cdc.gov/tobacco/basic_information/e-cigarettes/severe-lung-disease/health-departments/index.html#primary-case-def).
14. Tsai M, Song MA, McAndrew C, et al. Electronic versus combustible cigarette effects on inflammasome component release into human lung. Am J Respir Crit Care Med 2019;199:922-925.
15. Song MA, Freudenheim JL, Brasky TM, et al. Biomarkers of exposure and effect in the lungs of smokers, non-smokers and electronic cigarette users. Cancer Epidemiol Biomarkers Prev 2019 December 17 (Epub ahead of print).
16. Ohio State University Institutional Review Board. Effects of electronic cigarette use on the lungs. OSU-2015C0088; NCT02596685. 2019 (https://clinicaltrials.gov/ct2/show/NCT02596685?term=NCT02596685&draw=1&rank=1).
17. Taylor JK. Quality assurance of chemical measurements. New York: Lewis Publishers, 1987.
18. Cao Z, Schmitt TC, Varma V, Sloper D, Beger RD, Sun J. Evaluation of the performance of Lipidyzer platform and its application in the lipidomics analysis in mouse heart and liver. J Proteome Res 2019 July 26 (Epub ahead of print).
19. Orsavova J, Misurcova L, Ambrozova JV, Vicha R, Mlcek J. Fatty acids composition of vegetable oils and its contribution to dietary energy intake and dependence of cardiovascular mortality on dietary intake of fatty acids. Int J Mol Sci 2015;16:12871-12890.
20. Chambers DM, Blount BC, McElprang DO, Waterhouse MG, Morrow JC. Picogram measurement of volatile n-alkanes (n-hexane through n-dodecane) in blood using solid-phase microextraction to assess nonoccupational petroleum-based fuel exposure. Anal Chem 2008;80:4666-4674.
21. Rotolo MC, Pellegrini M, Martucci P, et al. Cannabinoids determination in bronchoalveolar lavages of cannabis smokers with lung disease. Clin Chem Lab Med 2019;57:498-503.
22. National Center for Biotechnology Information. PubChem database: limonene, CID=22311 (https://pubchem.ncbi.nlm.nih.gov/compound/Limonene).
23. Larsen ST, Hougaard KS, Hammer M, et al. Effects of R-(+)- and S-(-)-limonene on the respiratory tract in mice. Hum Exp Toxicol 2000;19:457-466.
24. Desmarchelier C, Tourniaire F, Prévéraud DP, et al. The distribution and relative hydrolysis of tocopheryl acetate in the different matrices coexisting in the lumen of the small intestine during digestion could explain its low bioavailability. Mol Nutr Food Res 2013;57:1237-1245.
25. Reboul E. Vitamin E bioavailability: mechanisms of intestinal absorption in the spotlight. Antioxidants (Basel) 2017;6(4):E95-E95.
26. Kamal MA, Raghunathan VA. Modulated phases of phospholipid bilayers induced by tocopherols. Biochim Biophys Acta 2012;1818:2486-2493.
27. Massey JB, She HS, Pownall HJ. Interaction of vitamin E with saturated phospholipid bilayers. Biochem Biophys Res Commun 1982;106:842-847.
28. Zuo YY, Veldhuizen RA, Neumann AW, Petersen NO, Possmayer F. Current perspectives in pulmonary surfactant — inhibition, enhancement and evaluation. Biochim Biophys Acta 2008;1778:1947-1977.
29. Casals C, Cañadas O. Role of lipid ordered/disordered phase coexistence in pulmonary surfactant function. Biochim Biophys Acta 2012;1818:2550-2562.
30. Wu D, O’Shea DF. Potential for release of pulmonary toxic ketene from vaping pyrolysis of vitamin E acetate. ChemRxiv. December 6, 2019 (https://chemrxiv.org/articles/Potential_for_Release_of_Pulmonary_Toxic_Ketene_from_Vaping_Pyrolysis_of_Vitamin_E_Acetate/10058168).
31. Taylor J, Wiens T, Peterson J, et al. Characteristics of e-cigarette, or vaping, products used by patients with associated lung injury and products seized by law enforcement — Minnesota, 2018 and 2019. MMWR Morb Mortal Wkly Rep 2019;68:1096-1100.
32. National Institutes of Health. Notice of Special Interest (NOSI): availability of administrative and revision supplements to expand vaping research and understand EVALI — Notice Number: NOT-HL-19-724. November 6, 2019 (https://grants.nih.gov/grants/guide/notice-files/NOT-HL-19-724.html).
Citing Articles (132)
Comments (2)
EVALI denotes electronic-cigarette, or vaping, product use–associated lung injury, HIV human immunodeficiency virus, and PCR polymerase chain reaction.
This criterion is defined as the use of an electronic device (e.g., electronic nicotine-delivery system, e-cigarette, vaporizer, or other device) or dabbing to inhale substances (e.g., nicotine, marijuana, tetrahydrocannabinol [THC], THC concentrates, cannabidiol, synthetic cannabinoids, flavorings, and other substances).
NA denotes not analyzed.
The listed toxicants were detected in bronchoalveolar-lavage fluid obtained from 51 patients with EVALI in 16 states from August through December 2019 and in 99 healthy comparators.
AFB denotes acid-fast bacilli, BAL bronchoalveolar lavage, and CT computed tomography.
Figures/Media
- Case Definitions for Patients with EVALI.*
Case Definitions for Patients with EVALI. - Characteristics of EVALI Case Patients and Healthy Comparators.*
Characteristics of EVALI Case Patients and Healthy Comparators. - Frequency of Detection of Priority Toxicants in EVALI Case Patients and in Healthy Comparators.*
Frequency of Detection of Priority Toxicants in EVALI Case Patients and in Healthy Comparators. - Exposure History and Clinical Characteristics of Three Patients with Probable Diagnosis of EVALI without Evidence of Vitamin E Acetate in BAL Fluid.*
Exposure History and Clinical Characteristics of Three Patients with Probable Diagnosis of EVALI without Evidence of Vitamin E Acetate in BAL Fluid.
