Health Disparities Among Youth

Despite significant progress in research, practice, and policy, disparities in youth health risk behaviors pdf icon[PDF – 46 KB] persist. Health disparities are preventable differences in the burden of disease, injury, violence, or opportunities to achieve optimal health that are experienced by socially disadvantaged populations.1 Populations can be defined by factors such as race or ethnicity, gender, education or income, disability, geographic location (e.g., rural or urban), or sexual orientation. Health disparities are inequitable and are directly related to the historical and current unequal distribution of social, political, economic, and environmental resources.
Health disparities result from multiple factors, including
- Poverty
- Environmental threats
- Inadequate access to health care
- Individual and behavioral factors
- Educational inequalities
Health disparities are also related to inequities in education. Dropping out of school is associated with multiple social and health problems.2-3 Overall, individuals with less education are more likely to experience a number of health risks, such as obesity, substance abuse, and intentional and unintentional injury, compared with individuals with more education.4 Higher levels of education are associated with a longer life and an increased likelihood of obtaining or understanding basic health information and services needed to make appropriate health decisions.5-7
At the same time, good health is associated with academic success. Higher levels of protective health behaviors and lower levels of health risk behaviors are been associated with higher academic grades among high school students.8 Health risks such as teenage pregnancy, poor dietary choices, inadequate physical activity, physical and emotional abuse, substance abuse, and gang involvement have a significant impact on how well students perform in school.9-13
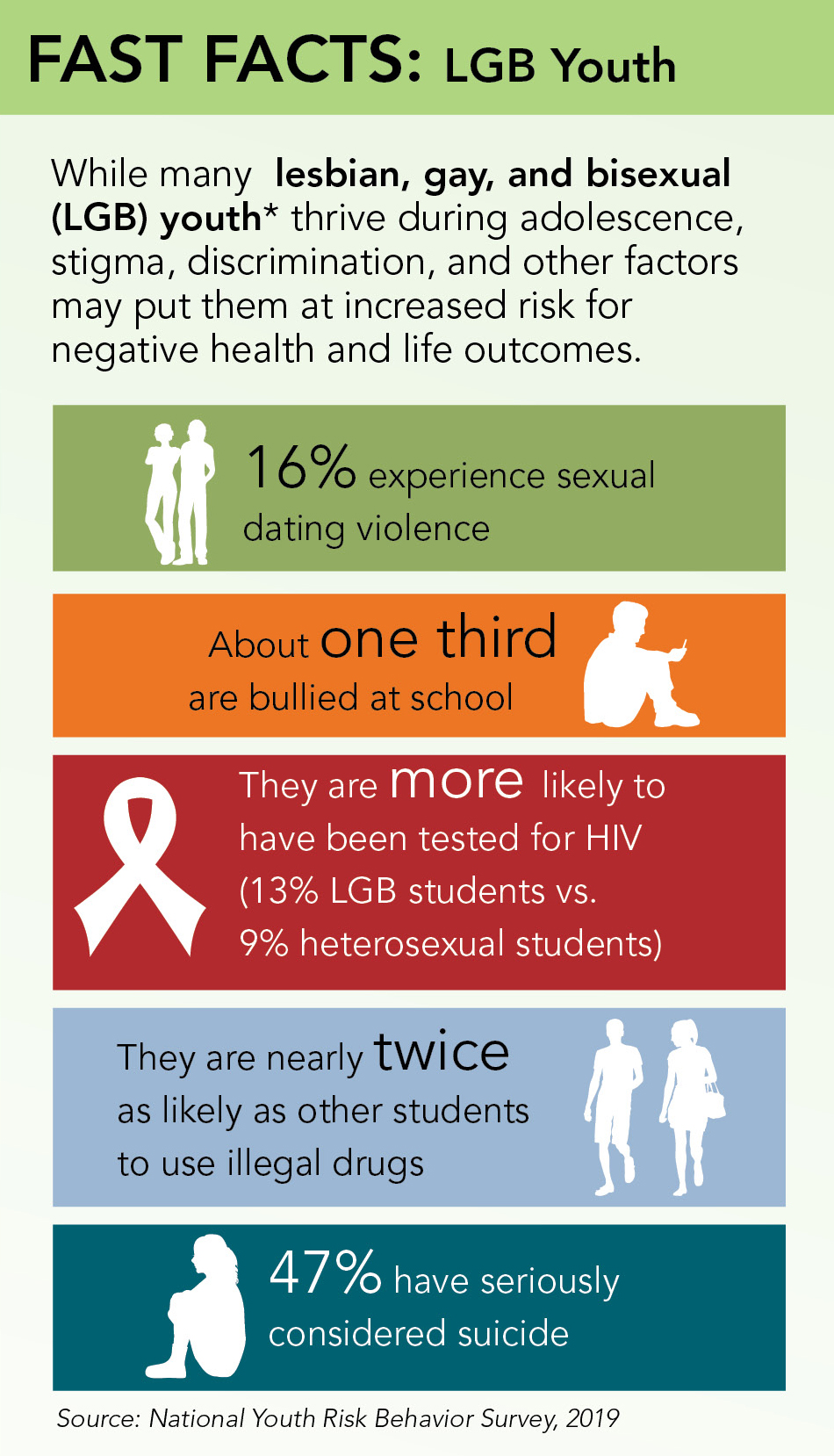
The 2019 Youth Risk Behavior Survey (YRBS) results show the health disparities that exist among sexual minority high school students or students who identify as lesbian, gay or bisexual (LGB); are not sure of their sexual identity; or who report sexual contact with persons of the same sex.
Data from the YRBS Data Summary & Trends Report pdf icon[PDF - 31 MB] reveal that sexual minority youth experience significantly higher levels of violence in school, bullying and sexual violence, and face significantly higher risks for suicide, depression, and substance use than their heterosexual peers. These trends are consistent with previous studies that show LGBTQ students are at a disproportionately higher risk for poor academic performance and negative health outcomes related to
- sexual behaviors,
- experiences of violence,
- substance use, and
- mental health, including suicide.
Comprehensive, community-wide prevention efforts can provide protection and reduce the health risks and negative experiences of LGBTQ students. To thrive in their schools and communities, all students, including LGBTQ students, need to feel socially, emotionally, and physically safe and supported. Everyone has a role to play in helping youth become healthy adults. Connectedness – or social bonds – to peers, teachers, schools, or community organizations is key. Working together, families, parents, schools, health and community organizations can address health risk behaviors and experiences by providing sexual health education, sexual health services, and safe and supportive environments to help LGBTQ students thrive.
- chart icon
- file chart line solid icon
- users solid icon
- chart icon
- school solid icon
- clipboard check solid icon
- people icon
- clipboard check solid icon
The National HIV/AIDS Strategy: Updated to 2020external icon
- CDC. Community Health and Program Services (CHAPS): Health Disparities Among Racial/Ethnic Populations. Atlanta: U.S. Department of Health and Human Services; 2008
- McCarty C, Mason W, Kosterman R, Hawkins J, Lengua L, McCauley E. Adolescent school failure predicts later depression among girls. Journal of Adolescent Health 2008;43:180–187.
- Ellickson P, Saner H, McGuigan K. Profiles of violent youth: substance use and concurrent problems. American Journal of Public Health 1997;87(6):985–991.4
- U.S. Department of Health and Human Services. Healthy People 2010 Objectives: Educational and Community Based Programs; 2000.
- Liao Y, McGee D, Kaufman J, Cao G, Cooper R. Socioeconomic status and morbidity in the last years of life. American Journal of Public Health 1999;89(4):569–572.
- Jemal A, Thun M, Ward E, Henley J, Cokkinides V, Murray T. Mortality from leading causes by education and race in the United States, 2001. American Journal of Preventive Medicine 2008;34(1):1–8.e7.
- Breese P, Burman W, Goldberg S, Weis S. Education level, primary language, and comprehension of the informed consent process. Journal of Empirical Research on Human Research Ethics 2007;2(4):69–79.
- Rasberry CN, Tiu GF, Kann L, McManus T, Michael SL, Merlo CL, Lee SM, Bohm MK, Annor F, Ethier K. Health-related behaviors and academic achievement among high school students—United States, 2015. MMWR Morb Mortal Wkly Rep 2917;66:922-927.
- Choi Y. Academic achievement and problem behaviors among Asian Pacific Islander American adolescents. Journal of Youth Adolescence 2007;(36)4:403–415.
- Stuart S, Sachs M, Lidicker J, Brett S, Wright A, Libonati J. Decreased scholastic achievement in overweight middle school students. Obesity 2008;16(7):1535–1538.
- Valois RF, MacDonald JM, Bretous L, Fischer MA, Drane JW. Risk factors and behaviors associated with adolescent violence and aggression. American Journal of Health Behavior 2002;26(6):454–464.
- Chomitz V, Slining M, McGowan R, Mitchell S, Dawson G, Hacker K. Is there a relationship between physical fitness and academic achievement? Positive results from public school children in the Northeastern United States. Journal of School Health 2009;79(1):30-37.
- Field T, Diego M, Sanders CE. Exercise is positively related to adolescents’ relationships and academics. Adolescence 2001;36(141):105-110.