0
0 slides
Return to Slide Library
Slides
Outcomes of Interest for Off-Label rFVIIa Use in the Hospital Setting
Four Domains Used To Assess Relevant Studies
Rating the Strength of Evidence From the CER
Characteristics of Comparative Studies on Off-Label rFVIIa Use
Mean Differences in Mortality and Thromboembolic Event Rates by Study and rFVIIa Indication
Evidence of rFVIIa Use for Bleeding Secondary to Body Trauma vs. Usual Care
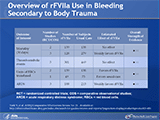
Overview of rFVIIa Use in Bleeding Secondary to Body Trauma
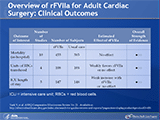
Overview of rFVIIa for Adult Cardiac Surgery: Clinical Outcomes
Increased Risk of Thromboembolic Events With rFVIIa Use for Adult Cardiac Surgery
Summary of Outcomes for Most Common Off-Label, In-Hospital Uses of rFVIIa
Conclusions From Available Evidence
Comparative Effectiveness of Management Strategies for Adults With Gastroesophageal Reflux Disease: An Update
Your slide tray is being processed.


 E-mail Updates
E-mail Updates




![Evidence of rFVIIa Use for Bleeding Secondary to Body Trauma vs. Usual Care
Trauma is the leading cause of death in young men between the ages of 15 and 40. Hemorrhage is the leading cause of early death (within 24–48 hours) in trauma and second only to traumatic brain injury (TBI) as the overall cause of mortality. Hemorrhage after traumatic injury is associated with an acquired coagulopathy known as the “acute coagulopathy of trauma.” The coagulopathy develops when there is tissue injury in combination with hypotension. The severity of coagulopathy increases with increasing injury severity and is associated with worse outcomes. Resuscitation of these patients can worsen the coagulopathy. The dilution of blood due to rapid infusion of crystalloid, the development of hypothermia, and persistent acidosis occur during resuscitation and are known together as the “lethal triad,” which conspires to impede coagulation. Not surprisingly, the conditions which lead to the development of lethal triad are worse in cases of severe hemorrhage, particularly in those cases that require massive transfusions (most frequently defined as the use of 10 or more units of packed red blood cells [RBCs] within 24 hours of injury). This acquired coagulopathy potentiates further bleeding, which in turn leads to further physiologic derangements, increased morbidity, and increased mortality. Unfortunately, blood products that are used to replace lost blood and to treat coagulopathy can carry risks of their own. In particular, studies have highlighted increased risks of acute respiratory distress syndrome (ARDS), multiorgan failure (MOF), and sepsis with higher levels of blood product transfusions. rFVIIa has been investigated in trauma as an adjunct to control bleeding and thereby reduce the above risks.](https://webarchive.library.unt.edu/web/20130228043918im_/http://www.effectivehealthcare.ahrq.gov/ehc/images/slideimgs/t032_s022_w160.png)