Chapter 3Infectious Diseases Related To Travel
Tuberculosis
INFECTIOUS AGENT
Mycobacterium tuberculosis is a rod-shaped, nonmotile, acid-fast bacterium.MODE OF TRANSMISSION
Tuberculosis (TB) transmission occurs when a contagious patient coughs, spreading bacilli through the air. Bovine TB (caused by the closely related Mycobacterium bovis) can be transmitted by consuming contaminated, unpasteurized dairy products from infected cattle.
EPIDEMIOLOGY
Globally, more than 9 million new TB cases and nearly 2 million TB-related deaths occur each year. TB occurs throughout the world, but the incidence varies (see Map 3-15). In the United States, the annual incidence is approximately 4 per 100,000 population, but in some countries in sub-Saharan Africa and Asia, the annual incidence is several hundred per 100,000.
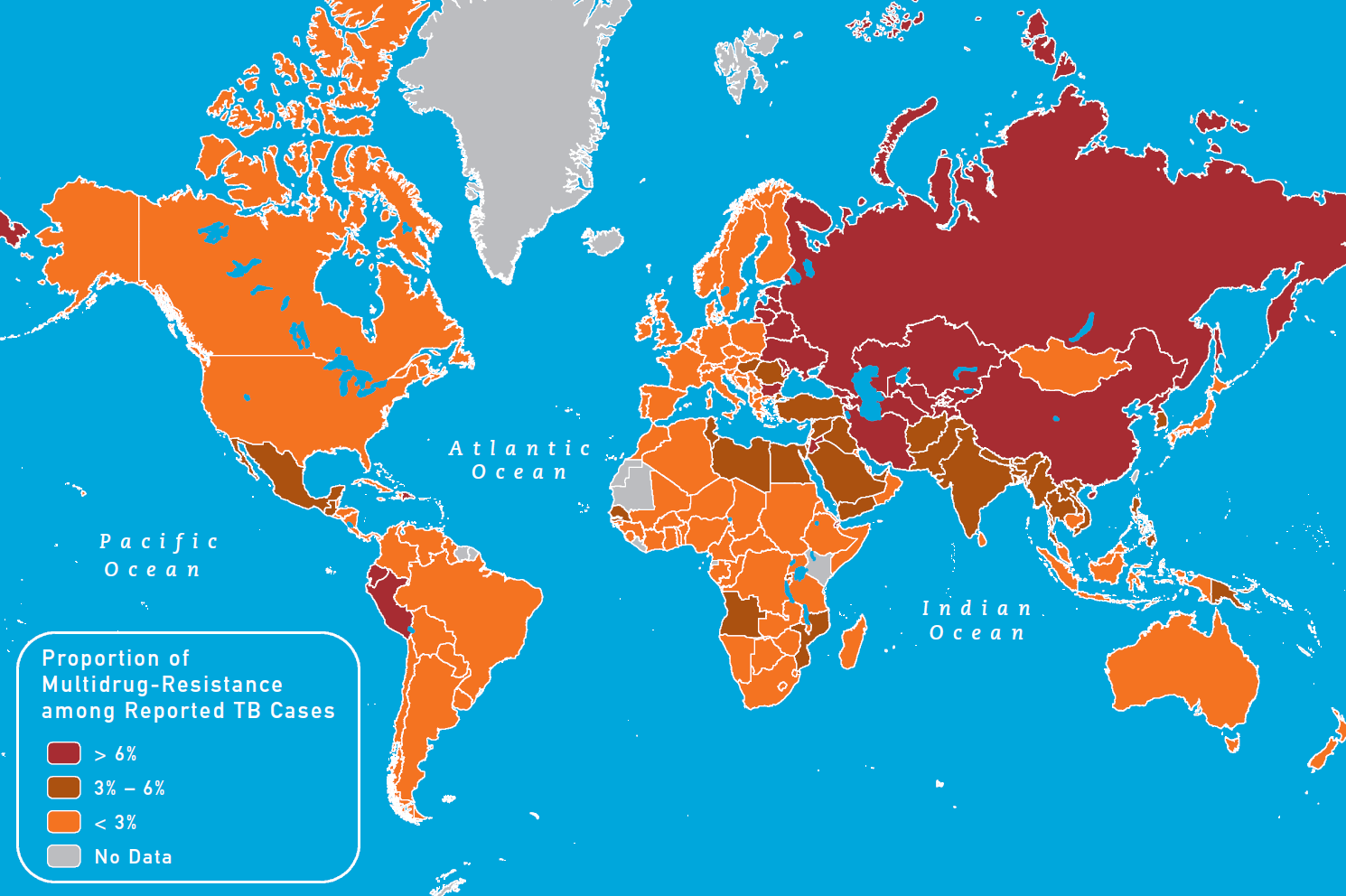
Drug-resistant TB is of increasing concern. Multidrug-resistant (MDR) TB is resistant to the 2 most effective drugs, isoniazid and rifampin. Extensively drug-resistant (XDR) TB is resistant to isoniazid and rifampin, any fluoroquinolone, and at least 1 of 3 injectable second-line drugs (amikacin, kanamycin, or capreomycin). MDR TB is less common than drug-susceptible TB, but nearly 500,000 new cases of MDR TB are diagnosed each year, and some countries have proportions of MDR TB as high as 20% (see Map 3-16). MDR and XDR TB are of particular concern among HIV-infected or other immunocompromised people. As of early 2010, XDR TB had been reported in 58 countries (see Map 3-17).
Travelers who anticipate possible prolonged exposure to TB (such as those who would spend time in hospitals, prisons, or homeless shelters) or those who stay for years in an endemic country should have a 2-step tuberculin skin test (TST) or a single interferon-γ release assay (IGRA), either the QuantiFERON TB test (Gold or Gold In-Tube versions) or T-SPOT.TB test, before leaving the United States (see Chapter 3, Perspectives: Tuberculin Skin Testing of Travelers). If the predeparture test result is negative, a single TST or IGRA should be repeated 8–10 weeks after returning from travel. Because people with HIV infection or other immunocompromising conditions are more likely to have an impaired response to the test, travelers should inform their physicians about such conditions. Except for travelers with impaired immunity, travelers who have already been infected are unlikely to be reinfected.
The risk of TB transmission on an airplane does not appear to be higher than in any other enclosed space. To prevent TB transmission on airplanes, people who have infectious TB should not travel by commercial airplanes or other commercial conveyances. The World Health Organization (WHO) has issued guidelines for notifying passengers who might have been exposed to TB aboard airplanes. Passengers concerned about possible exposure to TB should see their primary health care provider for evaluation.
Bovine TB (M. bovis) is a risk in travelers who consume unpasteurized dairy products in countries where M. bovis in cattle is common. Mexico is a common place of infection for US travelers.
Map 3-15. Estimated TB incidence rates, 20091
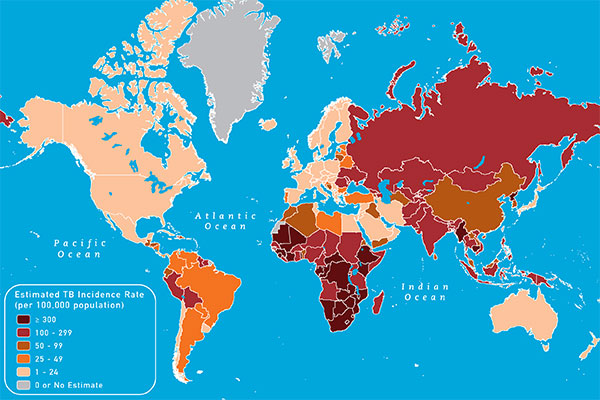
View Larger Map PDF Version (printable)
1Data from World Health Organization. Global tuberculosis control: WHO report 2010. Geneva: World Health Organization; 2010.
Map 3-16. Proportion of MDR TB among new TB cases, 20091

View Larger Map PDF Version (printable)
1Data from the World Health Organization’s Global tuberculosis database. Available from: www.who.int/tb/country/data/download/en/index.html.
Map 3-17. Distribution of countries and territories reporting at least one case of XDR TB as of 20101

View Larger Map PDF Version (printable)
1Data from the World Health Organization’s Global tuberculosis database. Available from: www.who.int/tb/country/data/download/en/index.html.
CLINICAL PRESENTATION
TB disease can affect any organ but most commonly occurs in the lungs (70%–80%). Common TB symptoms include prolonged cough, fever, anorexia, weight loss, night sweats, and hemoptysis. The most common types of extrapulmonary disease include lymphadenitis, pleuritis, bone and joint disease, meningitis, and genitourinary disease.
Infection is manifested by a positive TST or IGRA result, which usually occurs 8–10 weeks after exposure. Overall, only 5%–10% people progress from infection to disease during their lifetime. In the remainder, the infection remains in a latent state (latent TB infection or LTBI). However, the risk of progression is much higher in immunosuppressed people (8%–10% per year in HIV-infected people not receiving antiretroviral therapy). In recent years, people who are receiving tumor necrosis factor α inhibitors to treat rheumatoid arthritis and other chronic inflammatory conditions have also been found to be at increased risk for disease progression. LTBI is an asymptomatic condition, and people with LTBI do not transmit TB. Progression to disease can occur weeks to decades after initial infection.
DIAGNOSIS
Diagnosis of TB disease is confirmed by culturing M. tuberculosis from sputum or other respiratory specimens for pulmonary TB and from other affected body tissues or fluids for extrapulmonary TB. On average, it takes about 2 weeks to culture and identify M. tuberculosis, even with rapid culture techniques. A preliminary diagnosis of TB can be made when acid-fast bacilli are seen on sputum smear or in other body tissues or fluids. However, microscopy cannot distinguish between M. tuberculosis and nontuberculous mycobacteria. This is particularly problematic in countries such as the United States where the incidence is low. Nucleic acid amplification tests are more rapid than culture and specific for M. tuberculosis. They are also more sensitive than the acid-fast bacilli smear but less sensitive than culture. A diagnosis of TB disease can be made by using clinical criteria in the absence of microbiologic confirmation. LTBI is diagnosed by a positive TST or IGRA.
TREATMENT
People with LTBI can be treated to prevent progression to TB disease. American Thoracic Society (ATS)/CDC guidelines for treatment of LTBI recommend 9 months of isoniazid as the preferred treatment and suggest that 4 months of rifampin is a reasonable alternative. Travelers who suspect that they have been exposed to TB should inform their health care provider of the possible exposure and receive medical evaluation. CDC and ATS have published guidelines for targeted testing and treatment of LTBI. Recent data from WHO suggest that drug resistance is relatively common in some parts of the world. Travelers who have TST or IGRA conversion associated with international travel should consult experts in infectious diseases or pulmonary medicine.
TB disease is treated with a multiple-drug regimen for 6–9 months (usually isoniazid, rifampin, ethambutol, and pyrazinamide for 2 months, followed by isoniazid and rifampin for 4 months) if the TB is not MDR TB. MDR TB treatment is more difficult, requiring 4–6 drugs for 18–24 months; it should be managed by an expert in MDR TB. ATS/CDC/Infectious Diseases Society of America have published guidelines on TB treatment.
PREVENTIVE MEASURES FOR TRAVELERS
Travelers should avoid exposure to known TB patients in crowded environments (such as hospitals, prisons, or homeless shelters). Travelers who will be working in hospitals or health care settings where TB patients are likely to be encountered should be advised to consult infection control or occupational health experts about procedures for obtaining personal respiratory protective devices (such as N-95 respirators), along with respirator selection and training.
Based on WHO recommendations, Bacillus Calmette-Guérin (BCG) vaccine is used once at birth in most developing countries to reduce the severe consequences of TB in infants and children. However, BCG vaccine has variable efficacy in preventing the adult forms of TB and interferes with testing for LTBI with the TST. Therefore, BCG is not routinely recommended for use in the United States. Recently, some experts have advocated BCG vaccination for people who are likely to be exposed to MDR or XDR TB patients in settings where the TB infection control measures recommended in the United States are not fully implemented. BCG may offer some protection in this circumstance; however, people who receive BCG vaccination must follow all recommended TB infection control precautions to the extent possible. Additionally, IGRA is preferred over the TST for pre- and post-travel testing in people vaccinated with BCG.
To prevent infections due to M. bovis, travelers should also avoid eating or drinking unpasteurized dairy products.
BIBLIOGRAPHY
- American Thoracic Society and CDC. Diagnostic standards and classification of tuberculosis in adults and children. Am J Respir Crit Care Med. 2000 Apr;161(4 Pt 1):1376–95.
- American Thoracic Society and CDC. Targeted tuberculin testing and treatment of latent tuberculosis infection. Am J Respir Crit Care Med. 2000 Apr;161(4 Pt 2):S221–47.
- CDC. The role of BCG vaccine in the prevention and control of tuberculosis in the United States. A joint statement by the Advisory Council for the Elimination of Tuberculosis and the Advisory Committee on Immunization Practices. MMWR Recomm Rep. 1996 Apr 26;45(RR-4):1–18.
- CDC. Treatment of tuberculosis. MMWR Recomm Rep. 2003 Jun 20;52(RR-11):1–77.
- CDC. Updated guidelines for using interferon gamma release assays to detect Mycobacterium tuberculosis infection, United States. MMWR Recomm Rep. 2010.
- Jensen PA, Lambert LA, Iademarco MF, Ridzon R. Guidelines for preventing the transmission of Mycobacterium tuberculosis in health-care settings, 2005. MMWR Recomm Rep. 2005 Dec 30;54(RR-17):1–141.
- National Tuberculosis Controllers Association and CDC. Guidelines for the investigation of contacts of persons with infectious tuberculosis. MMWR Recomm Rep. 2005 Dec 16;54(RR-15):1–47.
- World Health Organization. Anti-tuberculosis drug resistance in the world: fourth global report. Geneva: World Health Organization; 2008. Available from: http://www.who.int/tb/publications/2008/drs_report4_26feb08.pdf.
- World Health Organization. Global tuberculosis control: WHO report 2010. Geneva: World Health Organization; 2010. Available from: http://www.who.int/tb/publications/global_report/2010/en/index.html.
- World Health Organization. Multidrug and extensively drug-resistant TB (M/XDR-TB): 2010 global report on surveillance and response. Geneva: World Health Organization; 2010. Available from: http://www.who.int/tb/features_archive/m_xdrtb_facts/en/index.html.
- World Health Organization. Tuberculosis and air travel: guidelines for prevention and control. Geneva: World Health Organization; 2008. Available from: http://www.who.int/tb/publications/2008/WHO_HTM_TB_2008.399_eng.pdf.
Contact Us:
- Centers for Disease Control and Prevention
1600 Clifton Rd
Atlanta, GA 30333 - 800-CDC-INFO
(800-232-4636)
TTY: (888) 232-6348 - New Hours of Operation
8am-8pm ET/Monday-Friday
Closed Holidays - Contact CDC-INFO

{kind=link}
{kind=link}
{kind=link}