
Treatment Option Overview
Key Points for This Section
- There are different types of treatment for patients with AIDS-related lymphoma.
- Treatment of AIDS-related lymphoma combines treatment of the lymphoma with treatment for AIDS.
- Three types of standard treatment are used:
- New types of treatment are being tested in clinical trials.
- Patients may want to think about taking part in a clinical trial.
- Patients can enter clinical trials before, during, or after starting their cancer treatment.
- Follow-up tests may be needed.
There are different types of treatment for patients with AIDS-related lymphoma.
Different types of treatment are available for patients with AIDS-related lymphoma. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Treatment of AIDS-related lymphoma combines treatment of the lymphoma with treatment for AIDS.
Patients with AIDS have weakened immune systems and treatment can cause further damage. For this reason, patients who have AIDS-related lymphoma are usually treated with lower doses of drugs than lymphoma patients who do not have AIDS.
Highly-active antiretroviral therapy (HAART) is used to slow progression of HIV (which is a retrovirus). Treatment with HAART may allow some patients to safely receive anticancer drugs in standard or higher doses. Medicine to prevent and treat infections, which can be serious, is also used.
AIDS-related lymphoma usually grows faster than lymphoma that is not AIDS-related and it is more likely to spread to other parts of the body. In general, AIDS-related lymphoma is harder to treat.
For more information about AIDS and its treatment, please see the AIDSinfo Web site.
Three types of standard treatment are used:
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid (intrathecal chemotherapy), an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). Combination chemotherapy is treatment using more than one anticancer drug. The way the chemotherapy is given depends on the type and stage of the cancer being treated.
Intrathecal chemotherapy may be used in patients who are more likely to have lymphoma in the central nervous system (CNS).

Colony-stimulating factors are sometimes given together with chemotherapy. This helps lessen the side effects chemotherapy may have on the bone marrow.
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy. External radiation therapy uses a machine outside the body to send radiation toward the cancer. Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer. The way the radiation therapy is given depends on the type and stage of the cancer being treated.
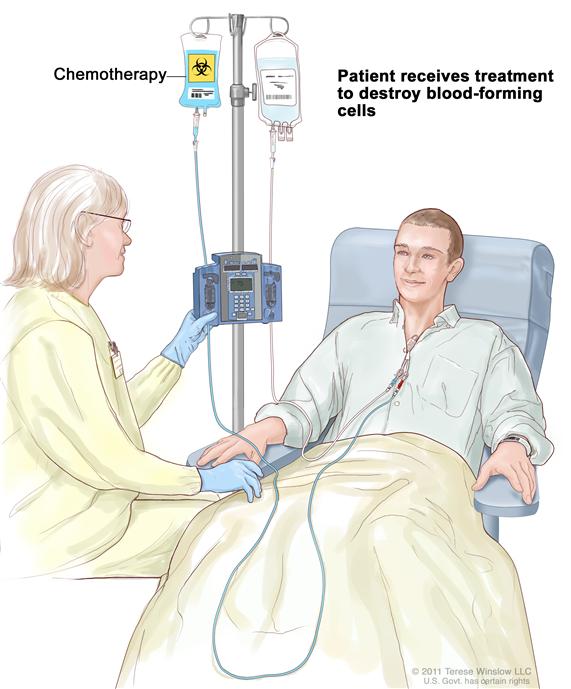
High-dose chemotherapy with stem cell transplant
High-dose chemotherapy with stem cell transplant is a way of giving high doses of chemotherapy and replacing blood -forming cells destroyed by the cancer treatment. Stem cells (immature blood cells) are removed from the blood or bone marrow of the patient or a donor and are frozen and stored. After the chemotherapy is completed, the stored stem cells are thawed and given back to the patient through an infusion. These reinfused stem cells grow into (and restore) the body's blood cells.


New types of treatment are being tested in clinical trials.
This summary section describes treatments that are being studied in clinical trials. It may not mention every new treatment being studied. Information about clinical trials is available from the NCI Web site.
Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack specific cancer cells without harming normal cells. Monoclonal antibody therapy is one type of targeted therapy being studied in the treatment of AIDS-related lymphoma.
Monoclonal antibody therapy is a cancer treatment that uses antibodies made in the laboratory from a single type of immune system cell. These antibodies can identify substances on cancer cells or normal substances that may help cancer cells grow. The antibodies attach to the substances and kill the cancer cells, block their growth, or keep them from spreading. Monoclonal antibodies are given by infusion. These may be used alone or to carry drugs, toxins, or radioactive material directly to cancer cells.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. See the Treatment Options section that follows for links to current treatment clinical trials. These have been retrieved from NCI's listing of clinical trials.
Follow-up tests may be needed.
Some of the tests that were done to diagnose the cancer or to find out the stage of the cancer may be repeated. Some tests will be repeated in order to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests. This is sometimes called re-staging.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back). These tests are sometimes called follow-up tests or check-ups.
 Back to Top
Back to Top