Background
Discontinuity is an unfortunate but necessary reality of hospital care. No provider can stay in the hospital around the clock, so patients will inevitably be cared for by many different providers during hospitalization. Nurses change shift every 8 to 12 hours, and, particularly at teaching institutions, multiple physicians may be responsible for a patient's care at different times of the day. This discontinuity creates opportunities for error when clinical information is not accurately transferred between providers. As one author put it, "for anyone who has watched children playing 'Telephone'…the inherent potential for error in signouts is obvious." The problems posed by handoffs of care have gained more attention since the 2003 implementation of regulations limiting housestaff duty hours, which has led to greater discontinuity among resident physicians.
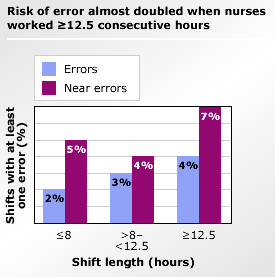
Source: Scott LD, Rogers AE, Hwang WT, Zhang Y. Effects of critical care nurses' work hours on vigilance and patients' safety. Am J Crit Care. 2006;15:30-37. [go to PubMed]
The process of transferring responsibility for care is referred to as the "handoff," with the term "signout" used to refer to the act of transmitting information about the patient. (This Primer will discuss handoffs and signouts in the context of transfers of care during hospitalization. For information about safety issues at the time of hospital discharge, please see the related Patient Safety Primer Adverse Events after Hospital Discharge.)
Handoffs and signouts have been linked to adverse clinical events in settings ranging from the emergency department to the intensive care unit. One study found that being cared for by a covering resident was a risk factor for preventable adverse events; more recently, communication failures between providers have been found to be a leading cause of preventable error in studies of closed malpractice claims affecting emergency physicians and trainees. The seemingly straightforward act of communicating an accurate medication list is a well-recognized source of error. To avert this problem, hospitals are required to "reconcile" medications across the continuum of care. (For more information, see the related Primer "Medication Reconciliation.")
Implementing Structured Handoff and Signout Protocols
Current signout mechanisms are generally ad-hoc, varying from hospital to hospital and unit to unit. Guidelines for safe handoffs focus on standardizing the signout mechanism. The components of a safe and effective signout can be summarized using the acronym ANTICipate:
- Administrative data (eg, patient's name, medical record number, and location) must be accurate.
- New clinical information must be updated.
- Tasks to be performed by the covering provider must be clearly explained.
- Illness severity must be communicated.
- Contingency plans for changes in clinical status must be outlined, to assist cross-coverage in managing the patient overnight.
Several guidelines have been developed for implementing standardized signouts. One trial of a computerized and structured signout system in an academic medical center demonstrated improved efficiency and more time spent in direct patient care after implementation. Innovative signout strategies have incorporated practices from other industries, such as the adaptation of a signout strategy from Formula One auto racing to the handoff from operating room to intensive care unit. In nursing, the SBAR method (Situation-Background-Assessment-Recommendation) has become widely accepted not only as a signout tool but as a structured method for all communications between providers.
Current Context
The Joint Commission requires all health care providers to "implement a standardized approach to handoff communications including an opportunity to ask and respond to questions" (2006 National Patient Safety Goal 2E). The Joint Commission National Patient Safety Goal also contains specific guidelines for the handoff process, many drawn from other high-risk industries:
- interactive communications
- up-to-date and accurate information
- limited interruptions
- a process for verification
- an opportunity to review any relevant historical data
The Accreditation Council for Graduate Medical Education also requires that residency programs maintain formal educational programs in handoffs and care transitions.