
|
|||
|
|
Fatality Assessment and Control Evaluation (FACE) Program |
|
Carpenter Dies After Being Struck by Uncontrolled Concrete Bucket When Crane Tips Over - Ohio |
| |||||||||||||
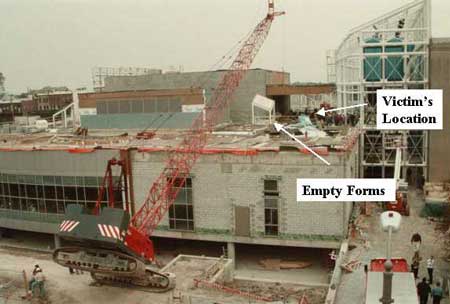
SummaryOn October 13, 1999, a 50-year-old male carpenter (the victim) at a municipal construction site died after he was struck by a loaded concrete bucket during a crane tip-over. The victim was removing forms from a newly constructed concrete wall while a concrete finishing crew was filling empty forms about 15 to 20 feet away (see Photo). Concrete was being hoisted from street level with a crawler-mounted mobile crane and landed under the direction of a roof-top spotter. As the crane operator hoisted a bucket load of concrete, swung it over the roof, and boomed out toward the empty forms, the crane lost stability, tipping toward the victim. When the crane operator realized what was occurring, he radioed a warning to the spotter who relayed the warning to roof-top workers. The victim had started to move when the uncontrolled concrete bucket swung toward him, striking his head and shoulder. Workers notified emergency personnel who responded within 6 minutes. The victim was pronounced dead at the scene. NIOSH investigators concluded that, to help prevent similar occurrences:
IntroductionOn October 13, 1999, a 50-year-old carpenter (the victim) at a municipal construction site died after he was struck by a loaded concrete bucket during a crane tip-over. On October 14, 1999, Ohio FACE staff and staff from NIOSH's Division of Safety Research (DSR) learned of the incident and contacted the Occupational Safety and Health Administration (OSHA) compliance officer assigned to the case. On October 26, 1999, a DSR safety engineer and the Ohio FACE investigator met with the OSHA compliance officer and reviewed the case file. A visit to the incident site was made and photographs and measurements were taken. The employer's Field Safety Officer and the Corporate Safety Director of the construction management company overseeing the project were interviewed. The library expansion project had been initiated about 1½ years prior to the incident. The county had contracted with a construction-management company with 44 years experience to oversee the project and had contracted other firms to perform the construction. Each contractor had safety responsibility for their own employees. However, the management company's Corporate Safety Director routinely visited the jobsite to conduct work observations and inspections. The victim's employer was a 51-year-old construction company employing 300 to 400 workers, depending on market conditions. Twenty-eight employees had been assigned to the library-expansion project and were engaged in various construction activities, including completion of concrete curbs, walls, and walkways for a roof-top green space. The employer had three field safety officers who traveled among various jobsite's conducting training and safety observations. The training program consisted primarily of on-the-job training through toolbox talks and work observations conducted by the job superintendents and safety officers. Job superintendents attended a 10-hour construction safety course. The victim was a journeyman carpenter with 16 years' experience with the company. This was the employer's second fatality. The employer had contracted with a crane rental company to supply the crane along with a certified crane operator of 26-years' experience. Back to TopInvestigationThe Manitowoc West Series 111 crawler-mounted lattice-boom crane had been built in 1998 and had been in use for 2,713 hours at the time of the incident. It was equipped with a computerized load-moment indicator (LMI) which monitored hoisting data and provided a readout of lift conditions for the crane operator. When properly programmed, the LMI activates a warning light when 90% of rated capacity is reached. When 100% of rated capacity is reached, an audible alarm is sounded and boom hoist up-and-down functions are interrupted. At the time of the incident, the crane mounted a 150-foot main boom with a 30-foot, 15-degree-offset jib. It had been set up at street level adjacent to the southwest face of the new library addition and was being used to hoist a 1-cubic-yard capacity concrete bucket from street level to rooftop. Because the rooftop work areas were not visible from the crane cab, bucket loads of concrete were landed under the direction of a spotter located on the roof and communicating with the crane operator by radio. At the time of incident, the bulk of the new structure had been completed and workers were engaged in adding electrical and mechanical systems, finishing the building's interior and constructing a rooftop green space on the new addition. At about 8:30 a.m. on the day of the incident, a concrete-finishing crew including a radio-equipped spotter, 3 concrete finishers, and a laborer, began pouring concrete into empty forms on the rooftop green space located approximately 25 feet above street level. Several loads of concrete were successfully hoisted and poured into forms located near the southwest face of the building between 80 and 106 feet from the crane's center pin (see Figure). According to the concrete truck driver, the bucket was filled to maximum capacity for the first load. Then he had been directed to fill the next three buckets only half-full. After pouring these three loads, the concrete crew moved away from the southwest face to begin filling forms which were a little over 130 feet from the crane's center pin. The crane operator lowered the empty bucket to street level and the concrete truck driver filled it to half capacity. The crane operator signaled the driver to fill the bucket to full capacity and after the bucket was full, the crane operator hoisted it, swung it over the roof and toward the empty forms at the direction of the spotter. At some point during the lift, the victim arrived on the rooftop after a work break and began stripping forms from a completed wall about 15 feet away from the concrete crew's location. As the crane operator moved the bucket toward the empty forms by lowering the boom (i.e., increasing swing radius), witnesses at street level observed the crane start to wobble and then slowly tip forward toward the building. The crane operator, realizing that the crane had lost stability and was tipping over toward the workers, radioed to the spotter to clear the area. He attempted to recover the crane by booming in (i.e., decreasing swing radius) but was unsuccessful. The finishing crew cleared the area, calling warnings to other roof-top workers located nearby. The victim apparently heard the warnings and was attempting to move when the bucket, swinging out of control, struck his head and shoulder. Workers notified emergency personnel who responded within 6 minutes. The victim was pronounced dead at the scene. Evaluation of the crane configuration, the distance of the intended landing site from the crane's center pin, and the manufacturer's load chart indicate that the crane's recommended capacity had been exceeded. Back to TopCause of DeathThe county's deputy coroner established the cause of death as blunt head and chest injuries. Recommendations and DiscussionRecommendation #1: Employers, crane owners, and operators should ensure that cranes are operated within their safe capacities as recommended by the crane manufacturer's load chart.Discussion: Measurements conducted after the incident indicate that the intended landing site for the loaded concrete bucket was approximately 132 feet from the crane's center pin. The manufacturer's load chart lists a capacity of 3,620 lbs. for this radius (see Appendix). The hoisted load at the time of the incident including the headache ball, 50 feet of load line, rigging fixtures, and the loaded concrete bucket was estimated to be 5110 lbs., 1,490 lbs. above the recommended load chart capacity (see Appendix for a complete tally of hoisted weights). The operator could not see the landing spot; the earlier lifts had been landed near the center of the building (see Figure). Although the concrete crew moved away from the roof edge when they relocated, they also moved to the south. From the crane operator's perspective at street level, this new location may have appeared to be closer to the crane (i.e., shorter radius). After the incident, the crane operator stated that he had been "working back toward the crane" at the time of the tip over (i.e., the landing locations getting closer to the crane's center pin as work continued). Because of these circumstances, the crane operator may have believed that the crane would be operating at a shorter radius where the crane would have greater lifting capacity. As mentioned previously, the crane was equipped with a computerized LMI designed to interrupt the hoist operation when hoisted loads reached 100% of manufacturer's rating. After the incident, the operator stated that the LMI had been indicating about 2700 lbs. during the morning's lifts. The LMI was examined and tested by manufacturer's representatives and found to be indicating false readings. Load-moment indicators and similar instruments may offer protection against injury and loss from crane overloads by providing information of load parameters to guide the judgment of a competent operator. However, their use cannot be substituted for the judgment of a qualified operator with knowledge of the hoisted loads, swing radius, and load chart information.
| ||||||||||||||
 |

|
| Figure.
Southwest Corner of Library |
Hoisted Load Tally
headache ball from police photo .................................................................... 650 lbs.
shackle & hook from OSHA field notes ......................................................... 30 lbs.
50 feet of load line @ 2 lbs, per foot ................................................................ 100 lbs.
bucket + cured concrete from consultant evaluation ................................... 4330 lbs.
hoisted load ........................................................................................................ 5110 lbs.
Rated Capacities from Load Chart (75% of tipping)
Swing Radius |
Manufacturer's Rated Capacity |
130 feet |
3970 lbs |
135 feet |
3620 lbs |
Note: The load chart does not list a capacity for a radius of 132 feet. Recommended practice for safe hoisting dictates use of the capacity at the next greater swing radius.[3]
The FACE investigation project is the cornerstone of the overall NIOSH program to prevent occupational fatalities. The objectives for this effort include the investigation of occupational fatalities to assess and characterize the circumstances of these events in order to develop succinct descriptive and evaluative reports for distribution to occupational safety and health groups across the country. This work is being conducted by the FACE investigation team. It is expected that the reports alone will have a major impact by better defining the causal factors behind occupational fatalities, calling national attention to the problem, and providing insights into the prevention efforts that are needed. However, the program does not determine fault or place blame on companies or individual workers.