Introduction
The Breasts
Understanding Cancer
Risk Factors
Screening
Symptoms
Diagnosis
Additional Tests
Staging
Treatment
Breast Reconstruction
Complementary and Alternative Medicine
Nutrition and Physical Activity
Follow-up Care
Sources of Support
The Promise of Cancer Research
National Cancer Institute Information Resources
National Cancer Institute Publications
Introduction
This National Cancer Institute (NCI) booklet (NIH Publication No. 05-1556) has important information about
breast
cancer.* Breast cancer is the most common type of cancer among women in
this country (other than skin cancer). Each year, more than 211,000 American
women learn they have this disease.
You will read about possible causes, screening, symptoms, diagnosis, treatment,
and supportive care. You will also find ideas about how to cope with the
disease.
|
Breast Cancer in Men
Each year, about 1,700 men in this country learn they have breast cancer. Most
information in this booklet applies to men with breast cancer. However, more
specific information about breast cancer in men is available on NCI's Web site
at http://www.cancer.gov and from NCI's Cancer Information Service at
1-800-4-CANCER.
|
Scientists are studying breast cancer to find out more about its causes. And
they are looking for better ways to prevent, find, and treat it.
NCI provides information about cancer, including the publications mentioned in
this booklet. You can order these materials by telephone or on the Internet.
You can also read them online and print your own copy.
*Words that may be new to readers appear in italics. The
"Dictionary 2" section explains these terms. Some words in the "Dictionary" have a "sounds-like" spelling to show how to pronounce them.
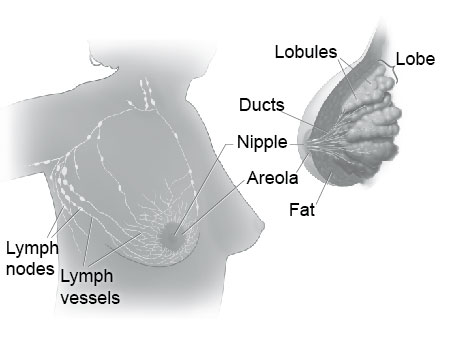
The Breasts
The
breasts
sit on the chest muscles that cover the ribs. Each breast is made
of 15 to 20
lobes.
Lobes contain many smaller
lobules.
Lobules contain groups
of tiny
glands
that can produce milk. Milk flows from the lobules through thin
tubes called
ducts
to the
nipple.
The nipple is in the center of a dark area of
skin called the
areola.
Fat fills the spaces between the lobules and ducts.
The breasts also contain
lymph vessels.
These vessels lead to small, round
organs
called
lymph nodes.
Groups of lymph nodes are near the breast in the
axilla
(underarm), above the collarbone, in the chest behind the breastbone,
and in many other parts of the body. The lymph nodes trap
bacteria,
cancer
cells,
or other harmful substances.
|
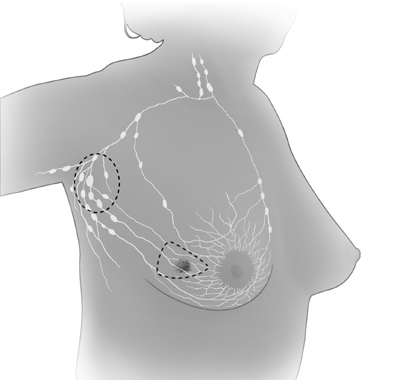
| These pictures show the parts of the breast and the lymph
nodes and lymph vessels near the breast. |
Understanding Cancer
Cancer begins in cells, the building blocks that make up
tissues.
Tissues make
up the organs of the body.
Normally, cells grow and divide to form new cells as the body needs them. When
cells grow old, they die, and new cells take their place.
Sometimes, this orderly process goes wrong. New cells form when the body does
not need them, and old cells do not die when they should. These extra cells can
form a mass of tissue called a growth or
tumor.
Tumors can be
benign
or
malignant:
Benign tumors are not cancer:
-
Benign tumors are rarely life-threatening.
-
Generally, benign tumors can be removed. They usually do not grow back.
-
Cells from benign tumors do not invade the tissues around them.
-
Cells from benign tumors do not spread to other parts of the body.
Malignant tumors are cancer:
-
Malignant tumors are generally more serious than benign tumors. They may be
life-threatening.
-
Malignant tumors often can be removed. But sometimes they grow back.
-
Cells from malignant tumors can invade and damage nearby tissues and organs.
-
Cells from malignant tumors can spread (metastasize)
to other parts of the
body. Cancer cells spread by breaking away from the original
(primary)
tumor
and entering the bloodstream or
lymphatic system. The cells invade other organs
and form new tumors that damage these organs. The spread of cancer is called
metastasis.
When breast cancer cells spread, the cancer cells are often found in lymph
nodes near the breast. Also, breast cancer can spread to almost any other part
of the body. The most common are the bones, liver, lungs, and brain. The new
tumor has the same kind of abnormal cells and the same name as the primary
tumor. For example, if breast cancer spreads to the bones, the cancer cells in
the bones are actually breast cancer cells. The disease is metastatic breast
cancer, not bone cancer. For that reason, it is treated as breast cancer, not
bone cancer. Doctors call the new tumor "distant" or metastatic disease.
Risk Factors
No one knows the exact causes of breast cancer. Doctors often cannot explain
why one woman develops breast cancer and another does not. They do know that
bumping, bruising, or touching the breast does not cause cancer. And breast
cancer is not contagious. You cannot "catch" it from another person.
Research has shown that women with certain
risk factors
are more likely than
others to develop breast cancer. A risk factor is something that may increase
the chance of developing a disease.
Studies have found the following risk factors for breast cancer:
-
Age: The chance of getting breast cancer goes up as a woman gets older. Most
cases of breast cancer occur in women over 60. This disease is not common
before
menopause.
-
Personal history of breast cancer: A woman who had breast cancer in one breast
has an increased risk of getting cancer in her other breast.
-
Family history: A woman's risk of breast cancer is higher if her mother,
sister, or daughter had breast cancer. The risk is higher if her family member
got breast cancer before age 40. Having other relatives with breast cancer (in
either her mother's or father's family) may also increase a woman's risk.
-
Certain breast changes: Some women have cells in the breast that look abnormal
under a microscope. Having certain types of abnormal cells
(atypical hyperplasia
and
lobular carcinoma in situ
[LCIS]) increases the risk of breast
cancer.
-
Gene
changes: Changes in certain genes increase the risk of breast cancer.
These genes include
BRCA1,
BRCA2,
and others. Tests can sometimes show the
presence of specific gene changes in families with many women who have had
breast cancer. Health care providers may suggest ways to try to reduce the risk
of breast cancer, or to improve the detection of this disease in women who have
these changes in their genes. NCI offers publications on gene testing.
-
Reproductive and menstrual history:
-
The older a woman is when she has her first child, the greater her chance of
breast cancer.
-
Women who had their first
menstrual period
before age 12 are at an increased
risk of breast cancer.
-
Women who went through menopause after age 55 are at an increased risk of
breast cancer.
-
Women who never had children are at an increased risk of breast cancer.
-
Women who take
menopausal hormone therapy
with
estrogen
plus
progestin
after
menopause also appear to have an increased risk of breast cancer.
-
Large, well-designed studies have shown no link between abortion or miscarriage
and breast cancer.
-
Race: Breast cancer is diagnosed more often in white women than Latina, Asian,
or African American women.
-
Radiation therapy
to the chest: Women who had radiation therapy to the chest
(including breasts) before age 30 are at an increased risk of breast cancer.
This includes women treated with radiation for
Hodgkin's lymphoma.
Studies show
that the younger a woman was when she received radiation treatment, the higher
her risk of breast cancer later in life.
-
Breast density: Breast tissue may be dense or fatty. Older women whose
mammograms
(breast
x-rays)
show more dense tissue are at increased risk of
breast cancer.
-
Taking
DES
(diethylstilbestrol): DES was given to some pregnant women in the
United States between about 1940 and 1971. (It is no longer given to pregnant
women.) Women who took DES during pregnancy may have a slightly increased risk
of breast cancer. The possible effects on their daughters are under study.
-
Being
overweight
or
obese
after menopause: The chance of getting breast cancer
after menopause is higher in women who are overweight or obese.
-
Lack of physical activity: Women who are physically inactive throughout life
may have an increased risk of breast cancer. Being active may help reduce risk
by preventing weight gain and obesity.
-
Drinking alcohol: Studies suggest that the more alcohol a woman drinks, the
greater her risk of breast cancer.
Other possible risk factors are under study. Researchers are studying the
effect of diet, physical activity, and genetics on breast cancer risk. They are
also studying whether certain substances in the environment can increase the
risk of breast cancer.
Many risk factors can be avoided. Others, such as family history, cannot be
avoided. Women can help protect themselves by staying away from known risk
factors whenever possible.
But it is also important to keep in mind that most women who have known risk
factors do not get breast cancer. Also, most women with breast cancer do not
have a family history of the disease. In fact, except for growing older, most
women with breast cancer have no clear risk factors.
If you think you may be at risk, you should discuss this concern with your
doctor. Your doctor may be able to suggest ways to reduce your risk and can
plan a schedule for checkups.
Screening
Screening
for breast cancer before there are
symptoms
can be important.
Screening can help doctors find and treat cancer early. Treatment is more
likely to work well when cancer is found early.
Your doctor may suggest the following screening tests for breast cancer:
You should ask your doctor about when to start and how often to check for
breast cancer.
To find breast cancer early, NCI recommends that:
-
Women in their 40s and older should have mammograms every 1 to 2 years. A
mammogram is a picture of the breast made with x-rays.
-
Women who are younger than 40 and have risk factors for breast cancer should
ask their health care provider whether to have mammograms and how often to have
them.
Mammograms can often show a breast lump before it can be felt. They also can
show a cluster of tiny specks of
calcium.
These specks are called
microcalcifications.
Lumps or specks can be from cancer,
precancerous
cells, or
other conditions. Further tests are needed to find out if abnormal cells are
present.
If an abnormal area shows up on your mammogram, you may need to have more
x-rays. You also may need a
biopsy.
A biopsy is the only way to tell for sure
if cancer is present. (The "Diagnosis 3" section has more information
on biopsy.)
Mammograms are the best tool doctors have to find breast cancer early. However,
mammograms are not perfect:
-
A mammogram may miss some cancers. (The result is called a "false negative.")
-
A mammogram may show things that turn out not to be cancer. (The result is
called a "false positive.")
-
Some fast-growing tumors may grow large or spread to other parts of the body
before a mammogram detects them.
Mammograms (as well as dental x-rays, and other routine x-rays) use very small
doses of radiation. The risk of any harm is very slight, but repeated x-rays
could cause problems. The benefits nearly always outweigh the risk. You should
talk with your health care provider about the need for each x-ray. You should
also ask for shields to protect parts of your body that are not in the picture.
During a clinical breast exam, your health care provider checks your breasts.
You may be asked to raise your arms over your head, let them hang by your
sides, or press your hands against your hips.
Your health care provider looks for differences in size or shape between your
breasts. The skin of your breasts is checked for a rash, dimpling, or other
abnormal signs. Your nipples may be squeezed to check for fluid.
Using the pads of the fingers to feel for lumps, your health care provider
checks your entire breast, underarm, and collarbone area. A lump is generally
the size of a pea before anyone can feel it. The exam is done on one side, then
the other. Your health care provider checks the lymph nodes near the breast to
see if they are enlarged.
A thorough clinical breast exam may take about 10 minutes.
You may perform monthly breast self-exams to check for any changes in your
breasts. It is important to remember that changes can occur because of aging,
your
menstrual cycle,
pregnancy, menopause, or taking birth control pills or
other
hormones.
It is normal for breasts to feel a little lumpy and uneven.
Also, it is common for your breasts to be swollen and tender right before or
during your menstrual period.
You should contact your health care provider if you notice any unusual changes
in your breasts.
Breast self-exams cannot replace regular screening mammograms and clinical
breast exams. Studies have not shown that breast self-exams alone reduce the
number of deaths from breast cancer.
|
You may want to ask the doctor the following questions about screening:
- Which tests do you recommend for me? Why?
- Do the tests hurt? Are there any risks?
- How much do mammograms cost? Will my health insurance pay for them?
- How soon after the mammogram will I learn the results?
- If the results show a problem, how will you learn if I have cancer?
|
Symptoms
Common symptoms of breast cancer include:
-
A change in how the breast or nipple feels
-
A lump or thickening in or near the breast or in the underarm area
-
Nipple tenderness
-
A change in how the breast or nipple looks
-
A change in the size or shape of the breast
-
A nipple turned inward into the breast
-
The skin of the breast, areola, or nipple may be scaly, red, or swollen. It may
have ridges or pitting so that it looks like the skin of an orange.
-
Nipple discharge (fluid)
Early breast cancer usually does not cause pain. Still, a woman should see her
health care provider about breast pain or any other symptom that does not go
away. Most often, these symptoms are not due to cancer. Other health problems
may also cause them. Any woman with these symptoms should tell her doctor so
that problems can be diagnosed and treated as early as possible.
Diagnosis
If you have a symptom or screening test result that suggests cancer, your
doctor must find out whether it is due to cancer or to some other cause. Your
doctor may ask about your personal and family medical history. You may have a
physical exam. Your doctor also may order a mammogram or other
imaging procedure. These tests make pictures of tissues inside the breast. After the
tests, your doctor may decide no other exams are needed. Your doctor may
suggest that you have a follow-up exam later on. Or you may need to have a
biopsy to look for cancer cells.
Your health care provider feels each breast for lumps and looks for other
problems. If you have a lump, your doctor will feel its size, shape, and
texture. Your doctor will also check to see if it moves easily. Benign lumps
often feel different from cancerous ones. Lumps that are soft, smooth, round,
and movable are likely to be benign. A hard, oddly shaped lump that feels
firmly attached within the breast is more likely to be cancer.
Diagnostic mammograms
are x-ray pictures of the breast. They take clearer, more
detailed images of areas that look abnormal on a screening mammogram. Doctors
use them to learn more about unusual breast changes, such as a lump, pain,
thickening, nipple discharge, or change in breast size or shape. Diagnostic
mammograms may focus on a specific area of the breast. They may involve special
techniques and more views than screening mammograms.
An
ultrasound
device sends out sound waves that people cannot hear. The waves
bounce off tissues. A computer uses the echoes to create a picture. Your doctor
can view these pictures on a monitor. The pictures may show whether a lump is
solid or filled with fluid. A
cyst
is a fluid-filled sac. Cysts are not cancer.
But a solid mass may be cancer. After the test, your doctor can store the
pictures on video or print them out. This exam may be used along with a
mammogram.
Magnetic resonance imaging
(MRI) uses a powerful magnet linked to a computer.
MRI makes detailed pictures of breast tissue. Your doctor can view these
pictures on a monitor or print them on film. MRI may be used along with a
mammogram.
Your doctor may refer you to a
surgeon
or breast disease specialist for a
biopsy. Fluid or tissue is removed from your breast to help find out if there
is cancer.
Some suspicious areas can be seen on a mammogram but cannot be felt during a
clinical breast exam. Doctors can use imaging procedures to help see the area
and remove tissue. Such procedures include
ultrasound-guided,
needle-localized,
or
stereotactic biopsy.
Doctors can remove tissue from the breast in different ways:
-
Fine-needle aspiration:
Your doctor uses a thin needle to remove fluid from a
breast lump. If the fluid appears to contain cells, a
pathologist
at a lab
checks them for cancer with a microscope. If the fluid is clear, it may not
need to be checked by a lab.
-
Core biopsy:
Your doctor uses a thick needle to remove breast tissue. A
pathologist checks for cancer cells. This procedure is also called a needle
biopsy.
-
Surgical biopsy: Your surgeon removes a sample of tissue. A pathologist checks
the tissue for cancer cells.
-
An
incisional
biopsy takes a sample of a lump or abnormal area.
-
An
excisional
biopsy takes the entire lump or area.
If cancer cells are found, the pathologist can tell what kind of cancer it is.
The most common type of breast cancer is ductal
carcinoma. Abnormal cells are
found in the lining of the ducts. Lobular carcinoma is another type. Abnormal
cells are found in the lobules.
|
You may want to ask your doctor the following questions before having a biopsy:
- What kind of biopsy will I have? Why?
- How long will it take? Will I be awake? Will it hurt? Will I have
anesthesia? What kind?
- Are there any risks? What are the chances of infection or bleeding after the biopsy?
- How soon will I know the results?
- If I do have cancer, who will talk with me about the next steps? When?
|
Additional Tests
If you are diagnosed with cancer, your doctor may order special lab tests on
the breast tissue that was removed. These tests help your doctor learn more
about the cancer and plan treatment:
-
Hormone receptor test:
This test shows whether the tissue has certain hormone
receptors. Tissue with these receptors needs hormones (estrogen
or
progesterone) to grow.
-
HER2
test: This test shows whether the tissue has a protein called human
epidermal growth factor receptor-2 (HER2) or the
HER2/neu
gene. Having too much
protein or too many copies of the gene in the tissue may increase the chance
that the breast cancer will come back after treatment.
Staging
To plan your treatment, your doctor needs to know the extent (stage) of the disease. The stage is based on the size of the tumor and whether the cancer has spread. Staging may involve x-rays and lab tests. These tests can show whether the cancer has spread and, if so, to what parts of your body. When breast cancer spreads, cancer cells are often found in lymph nodes under the arm (axillary lymph nodes). The stage often is not known until after surgery to remove the tumor in your breast and the lymph nodes under your arm.
These are the stages of breast cancer:
- Stage 0 is carcinoma in situ.
- Lobular carcinoma in situ (LCIS): Abnormal cells are in the lining of a lobule. (See picture of lobule on page 3.) LCIS seldom becomes invasive cancer. However, having LCIS in one breast increases the risk of cancer for both breasts.
- Ductal carcinoma in situ (DCIS): Abnormal cells are in the lining of a duct. DCIS is also called intraductal carcinoma. The abnormal cells have not spread outside the duct. They have not invaded the nearby breast tissue. DCIS sometimes becomes invasive cancer if not treated.
|
| This picture shows ductal carcinoma in situ. |
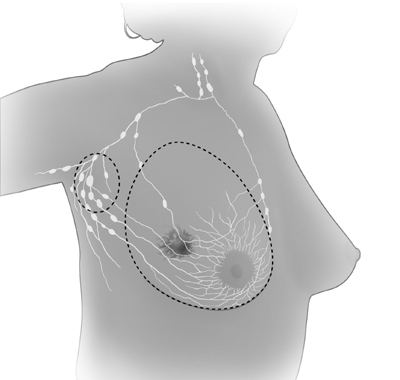
-
Stage I is an early stage of invasive breast cancer. The tumor is no more than 2 centimeters (three-quarters of an inch) across. Cancer cells have not spread beyond the breast.
|
| This picture shows cancer cells spreading outside the duct. The cancer cells are invading nearby tissue inside the breast. |
-
Stage II is one of the following:
- The tumor is no more than 2 centimeters (three-quarters of an inch) across. The cancer has spread to the lymph nodes under the arm.
- The tumor is between 2 and 5 centimeters (three-quarters of an inch to 2 inches). The cancer has not spread to the lymph nodes under the arm.
- The tumor is between 2 and 5 centimeters (three-quarters of an inch to 2 inches). The cancer has spread to the lymph nodes under the arm
- The tumor is larger than 5 centimeters (2 inches). The cancer has not spread to the lymph nodes under the arm.
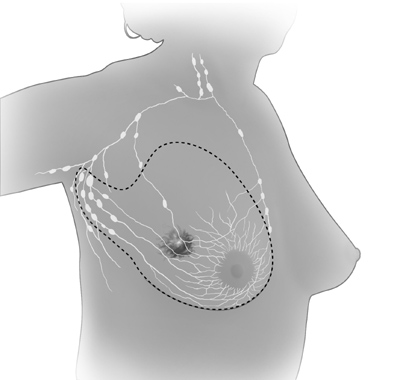
- Stage III is locally advanced cancer. It is divided into Stage IIIA, IIIB, and IIIC.
- Stage IIIA is one of the following:
- The tumor is no more than 5 centimeters (2 inches) across. The cancer has spread to underarm lymph nodes that are attached to each other or to other structures. Or the cancer may have spread to lymph nodes behind the breastbone.
- The tumor is more than 5 centimeters across. The cancer has spread to underarm lymph nodes that are either alone or attached to each other or to other structures. Or the cancer may have spread to lymph nodes behind the breastbone.
- Stage IIIB is a tumor of any size that has grown into the chest wall or the skin of the breast. It may be associated with swelling of the breast or with nodules (lumps) in the breast skin.
- The cancer may have spread to lymph nodes under the arm.
- The cancer may have spread to underarm lymph nodes that are attached to each other or other structures. Or the cancer may have spread to lymph nodes behind the breastbone.
- Inflammatory breast cancer is a rare type of breast cancer. The breast looks red and swollen because cancer cells block the lymph vessels in the skin of the breast. When a doctor diagnoses inflammatory breast cancer, it is at least Stage IIIB, but it could be more advanced.
- Stage IIIC is a tumor of any size. It has spread in one of the following ways:
- The cancer has spread to the lymph nodes behind the breastbone and under the arm.
- The cancer has spread to the lymph nodes above or below the collarbone.
- Stage IV is distant metastatic cancer. The cancer has spread to other parts of the body.
- Recurrent cancer is cancer that has come back (recurred) after a period of time when it could not be detected. It may recur locally in the breast or chest wall. Or it may recur in any other part of the body, such as the bone, liver, or lungs.
 |
Treatment
Many women with breast cancer want to take an active part in making decisions
about their medical care. It is natural to want to learn all you can about your
disease and treatment choices. Knowing more about breast cancer helps many
women cope.
Shock and stress after the diagnosis can make it hard to think of everything you
want to ask your doctor. It often helps to make a list of questions before an
appointment. To help remember what the doctor says, you may take notes or ask
whether you may use a tape recorder. You may also want to have a family member
or friend with you when you talk to the doctor - to take part in the discussion,
to take notes, or just to listen. You do not need to ask all your questions at
once. You will have other chances to ask your doctor or nurse to explain things
that are not clear and to ask for more details.
Your doctor may refer you to a specialist, or you may ask for a referral.
Specialists who treat breast cancer include
surgeons,
medical oncologists,
and
radiation oncologists.
You also may be referred to a
plastic surgeon.
Before starting treatment, you might want a second opinion about your diagnosis
and treatment plan. Many insurance companies cover a second opinion if you or
your doctor requests it. It may take some time and effort to gather medical
records and arrange to see another doctor. You may have to gather your
mammogram films, biopsy slides, pathology report, and proposed treatment plan.
Usually it is not a problem to take several weeks to get a second opinion. In
most cases, the delay in starting treatment will not make treatment less
effective. To make sure, you should discuss this delay with your doctor. Some
women with breast cancer need treatment right away.
There are a number of ways to find a doctor for a second opinion:
-
Your doctor may refer you to one or more specialists. At cancer centers,
several specialists often work together as a team.
-
NCI's Cancer Information Service, at 1-800-4-CANCER, can tell you about nearby
treatment centers. Information Specialists also can provide online assistance
through
LiveHelp 1 at http://www.cancer.gov/cis.
-
A local or state medical society, a nearby hospital, or a medical school can
usually provide the names of specialists.
-
The American Board of Medical Specialties (ABMS) has a list of doctors who have
had training and passed exams in their specialty. You can find this list in the
Official ABMS Directory of Board Certified Medical Specialists. This Directory
is in most public libraries. Also, ABMS offers this information at
http://www.abms.org 4. (Click on "Who's Certified.")
-
NCI provides a helpful fact sheet called "How To Find a Doctor or Treatment
Facility If You Have Cancer."
Women with breast cancer have many treatment options. These include
surgery,
radiation therapy,
chemotherapy,
hormone therapy,
and
biological therapy.
These
options are described below. Many women receive more than one
type of treatment.
The choice of treatment depends mainly on the stage of the disease. Treatment
options by stage are described below.
Your doctor can describe your treatment choices and the expected results. You
may want to know how treatment may change your normal activities. You may want
to know how you will look during and after treatment. You and your doctor can
work together to develop a treatment plan that reflects your medical needs and
personal values.
Cancer treatment is either
local therapy
or
systemic therapy:
-
Local therapy: Surgery and radiation therapy are local treatments. They
remove or destroy cancer in the breast. When breast cancer has spread to other
parts of the body, local therapy may be used to control the disease in those
specific areas.
-
Systemic therapy: Chemotherapy, hormone therapy, and biological therapy
are systemic treatments. They enter the bloodstream and destroy or control
cancer throughout the body. Some women with breast cancer have systemic therapy
to shrink the tumor before surgery or radiation. Others have systemic therapy
after surgery and/or radiation to prevent the cancer from coming back. Systemic
treatments also are used for cancer that has spread.
Because cancer treatments often damage healthy cells and tissues,
side effects
are common. Side effects depend mainly on the type and extent of the treatment.
Side effects may not be the same for each woman, and they may change from one
treatment session to the next.
Before treatment starts, your health care team will explain possible side
effects and suggest ways to help you manage them. NCI provides helpful booklets
about cancer treatments and coping with side effects. These include
Radiation Therapy and You 5,
Chemotherapy and You 6, Biological Therapy 7, and
Eating Hints for
Cancer Patients 8.
At any stage of disease,
supportive care
is available to control pain and other
symptoms, to relieve the
side effects of treatment, and to ease emotional
concerns. Information about such care is available on NCI's Web site at
http://www.cancer.gov/cancertopics/coping 9 and from Information
Specialists at 1-800-4-CANCER or
LiveHelp 1.
You may want to talk to your doctor about taking part in a
clinical trial,
a
research study of new treatment methods. The section on "The Promise of Cancer
Research 10" has more information about clinical trials.
|
You may want to ask your doctor these questions before your treatment begins:
-
What did the hormone receptor test show? What did other lab tests show?
-
Do any lymph nodes show signs of cancer?
-
What is the stage of the disease? Has the cancer spread?
-
What is the goal of treatment? What are my treatment choices? Which do you
recommend for me? Why?
-
What are the expected benefits of each kind of treatment?
-
What are the risks and possible side effects of each treatment? How can side
effects be managed?
-
What can I do to prepare for treatment?
-
Will I need to stay in the hospital? If so, for how long?
-
What is the treatment likely to cost? Will my insurance cover the cost?
-
How will treatment affect my normal activities?
-
Would a clinical trial be appropriate for me?
|
Surgery is the most common treatment for breast cancer. There are several types
of surgery. (See pictures below.) Your doctor can explain each type,
discuss and compare the benefits and risks, and describe how each will change
the way you look:
-
Breast-sparing surgery: An operation to remove the cancer but not the
breast is breast-sparing surgery. It is also called
breast-conserving surgery,
lumpectomy,
segmental mastectomy,
and
partial mastectomy.
Sometimes an
excisional biopsy serves as a lumpectomy because the surgeon removes the whole
lump.
The surgeon often removes the underarm lymph nodes as well. A separate incision
is made. This procedure is called an
axillary lymph node dissection.
It shows
whether cancer cells have entered the lymphatic system.
After breast-sparing surgery, most women receive radiation therapy to the
breast. This treatment destroys cancer cells that may remain in the breast.
-
Mastectomy:
An operation to remove the breast (or as much of the breast
tissue as possible) is a mastectomy. In most cases, the surgeon also removes
lymph nodes under the arm. Some women have radiation therapy after surgery.
Studies have found equal survival rates for breast-sparing surgery (with
radiation therapy) and mastectomy for Stage I and Stage II breast cancer.
Sentinel lymph node biopsy
is a new method of checking for cancer cells in the
lymph nodes. A surgeon removes fewer lymph nodes, which causes fewer side
effects. (If the doctor finds cancer cells in the axillary lymph nodes, an
axillary lymph node dissection usually is done.) Information about ongoing
studies of sentinel lymph node biopsy is in the section on "The
Promise of Cancer Research 10." These studies will learn the lasting effects of
removing fewer lymph nodes.
|
| In breast-sparing surgery, the surgeon removes the tumor in the breast and some
tissue around it. The surgeon may also remove lymph nodes under the arm. The
surgeon sometimes removes some of the lining over the chest muscles below the
tumor. |
|
| In
total
(simple)
mastectomy,
the surgeon removes the whole breast. Some lymph
nodes under the arm may also be removed. |
|
| In
modified radical mastectomy,
the surgeon removes the whole breast, and most
or all of the lymph nodes under the arm. Often, the lining over the chest
muscles is removed. A small chest muscle also may be taken out to make it
easier to remove the lymph nodes. |
You may choose to have
breast reconstruction.
This is
plastic surgery
to
rebuild the shape of the breast. It may be done at the same time as a
mastectomy or later. If you are considering reconstruction, you may wish to
talk with a plastic surgeon before having a mastectomy. More information is in the "Breast Reconstruction 11" section.
The time it takes to heal after surgery is different for each woman. Surgery
causes pain and tenderness. Medicine can help control the pain. Before surgery,
you should discuss the plan for pain relief with your doctor or nurse. After
surgery, your doctor can adjust the plan if you need more relief. Any kind of
surgery also carries a risk of infection, bleeding, or other problems. You
should tell your health care provider right away if you develop any problems.
You may feel off balance if you've had one or both breasts removed. You may
feel more off balance if you have large breasts. This imbalance can cause
discomfort in your neck and back. Also, the skin where your breast was removed
may feel tight. Your arm and shoulder muscles may feel stiff and weak. These
problems usually go away. The doctor, nurse, or
physical therapist
can suggest
exercises to help you regain movement and strength in your arm and shoulder.
Exercise can also reduce stiffness and pain. You may be able to begin gentle
exercises within days of surgery.
Because nerves may be injured or cut during surgery, you may have numbness and
tingling in your chest, underarm, shoulder, and upper arm. These feelings
usually go away within a few weeks or months. But for some women, numbness does
not go away.
Removing the lymph nodes under the arm slows the flow of
lymph
fluid. The fluid
may build up in your arm and hand and cause swelling. This swelling is
lymphedema.
Lymphedema can develop right after surgery or months to years
later.
You will need to protect your arm and hand on the treated side for the rest of
your life:
-
Avoid wearing tight clothing or jewelry on your affected arm
-
Carry your purse or luggage with the other arm
-
Use an electric razor to avoid cuts when shaving under your arm
-
Have shots, blood tests, and blood pressure measurements on the other arm
-
Wear gloves to protect your hands when gardening and when using strong
detergents
-
Have careful manicures and avoid cutting your cuticles
-
Avoid burns or sunburns to your affected arm and hand
You should ask your doctor how to handle any cuts, insect bites, sunburn, or
other injuries to your arm or hand. Also, you should contact the doctor if your
arm or hand is injured, swells, or becomes red and warm.
If lymphedema occurs, the doctor may suggest raising your arm above your heart
whenever you can. The doctor may show you hand and arm exercises. Some women
with lymphedema wear an elastic sleeve to improve lymph circulation.
Medication, manual lymph drainage (massage), or use of a machine that gently
compresses the arm may also help. You may be referred to a physical therapist
or another specialist.
More information about lymphedema is available on NCI's Web site at http://www.cancer.gov
and from Information Specialists at 1-800-4-CANCER or
LiveHelp 1.
|
You may want to ask your doctor these questions before having surgery:
-
What kinds of surgery can I consider? Is breast-sparing surgery an option for
me? Which operation do you recommend for me? Why?
-
Will my lymph nodes be removed? How many? Why?
-
How will I feel after the operation? Will I have to stay in the hospital?
-
Will I need to learn how to take care of myself or my incision when I get home?
-
Where will the scars be? What will they look like?
-
If I decide to have plastic surgery to rebuild my breast, how and when can that
be done? Can you suggest a plastic surgeon for me to contact?
-
Will I have to do special exercises to help regain motion and strength in my
arm and shoulder? Will a physical therapist or nurse show me how to do the
exercises?
-
Is there someone I can talk with who has had the same surgery I'll be having?
|
Radiation therapy (also called radiotherapy) uses high-energy rays to kill
cancer cells. Most women receive radiation therapy after breast-sparing
surgery. Some women receive radiation therapy after a mastectomy. Treatment
depends on the size of the tumor and other factors. The radiation destroys
breast cancer cells that may remain in the area.
Some women have radiation therapy before surgery to destroy cancer cells and
shrink the tumor. Doctors use this approach when the tumor is large or may be
hard to remove. Some women also have chemotherapy or hormone therapy before
surgery.
Doctors use two types of radiation therapy to treat breast cancer. Some women
receive both types:
-
External radiation: The radiation comes from a large machine outside the
body. Most women go to a hospital or clinic for treatment. Treatments are
usually 5 days a week for several weeks.
-
Internal radiation
(implant radiation): Thin plastic tubes (implants)
that hold a
radioactive
substance are put directly in the breast. The implants
stay in place for several days. A woman stays in the hospital while she has
implants. Doctors remove the implants before she goes home.
Side effects depend mainly on the dose and type of radiation and the part of
your body that is treated.
It is common for the skin in the treated area to become red, dry, tender, and
itchy. Your breast may feel heavy and tight. These problems will go away over
time. Toward the end of treatment, your skin may become moist and "weepy."
Exposing this area to air as much as possible can help the skin heal.
Bras and some other types of clothing may rub your skin and cause soreness. You
may want to wear loose-fitting cotton clothes during this time. Gentle skin
care also is important. You should check with your doctor before using any
deodorants, lotions, or creams on the treated area. These effects of radiation
therapy on the skin will go away. The area gradually heals once treatment is
over. However, there may be a lasting change in the color of your skin.
You are likely to become very tired during radiation therapy, especially in the
later weeks of treatment. Resting is important, but doctors usually advise
patients to try to stay as active as they can.
Although the side effects of radiation therapy can be distressing, your doctor
can usually relieve them.
|
You may want to ask your doctor these questions before having radiation therapy:
-
How will radiation be given?
-
When will treatment start? When will it end? How often will I have treatments?
-
How will I feel during treatment? Will I be able to drive myself to and from
treatment?
-
How will we know the treatment is working?
-
What can I do to take care of myself before, during, and after treatment?
-
Will treatment affect my skin?
-
How will my chest look afterward?
-
Are there any long-term effects?
-
What is the chance that the cancer will come back in my breast?
-
How often will I need checkups?
|
Chemotherapy uses anticancer drugs to kill cancer cells. Chemotherapy for
breast cancer is usually a combination of drugs. The drugs may be given as a
pill or by
injection
into a vein
(IV). Either way, the drugs enter the
bloodstream and travel throughout the body.
Women with breast cancer can have chemotherapy in an outpatient part of the
hospital, at the doctor's office, or at home. Some women need to stay in the
hospital during treatment.
Side effects depend mainly on the specific drugs and the dose. The drugs affect
cancer cells and other cells that divide rapidly:
-
Blood cells: These cells fight infection, help your blood to clot, and
carry oxygen to all parts of the body. When drugs affect your blood cells, you
are more likely to get infections, bruise or bleed easily, and feel very weak
and tired. Years after chemotherapy, some women have developed leukemia (cancer
of the blood cells).
-
Cells in hair roots: Chemotherapy can cause hair loss. Your hair will
grow back, but it may be somewhat different in color and texture.
-
Cells that line the
digestive tract:
Chemotherapy can cause poor
appetite, nausea and vomiting, diarrhea, or mouth and lip sores.
Your doctor can suggest ways to control many of these side effects.
Some drugs used for breast cancer can cause tingling or numbness in the hands
or feet. This problem usually goes away after treatment is over. Other problems
may not go away. In some women, the drugs used for breast cancer may weaken the
heart.
Some anticancer drugs can damage the
ovaries.
The ovaries may stop making
hormones. You may have symptoms of menopause. The symptoms include hot flashes
and vaginal dryness. Your menstrual periods may no longer be regular or may
stop. Some women become
infertile
(unable to become pregnant). For women over
the age of 35,
infertility
is likely to be permanent.
On the other hand, you may remain
fertile
during chemotherapy and be able to
become pregnant. The effects of chemotherapy on an unborn child are not known.
You should talk to your doctor about birth control before treatment begins.
Some breast tumors need hormones to grow. Hormone therapy keeps cancer cells
from getting or using the natural hormones they need. These hormones are
estrogen and progesterone. Lab tests can show if a breast tumor has hormone
receptors. If you have this kind of tumor, you may have hormone therapy.
This treatment uses drugs or surgery:
-
Drugs: Your doctor may suggest a drug that can block the natural
hormone. One drug is
tamoxifen,
which blocks estrogen. Another type of drug
prevents the body from making the female hormone
estradiol.
Estradiol is a form
of estrogen. This type of drug is an
aromatase inhibitor.
If you have not gone
through menopause, your doctor may give you a drug that stops the ovaries from
making estrogen.
-
Surgery: If you have not gone through menopause, you may have surgery to
remove your ovaries. The ovaries are the main source of the body's estrogen. A
woman who has gone through menopause does not need surgery. (The ovaries
produce less estrogen after menopause.)
The side effects of hormone therapy depend largely on the specific drug or type
of treatment. Tamoxifen is the most common hormone treatment. In general, the
side effects of tamoxifen are similar to some of the symptoms of menopause. The
most common are hot flashes and vaginal discharge. Other side effects are
irregular menstrual periods, headaches, fatigue, nausea, vomiting, vaginal
dryness or itching, irritation of the skin around the vagina, and skin rash.
Not all women who take tamoxifen have side effects.
It is possible to become pregnant when taking tamoxifen. Tamoxifen may harm the
unborn baby. If you are still menstruating, you should discuss birth control
methods with your doctor.
Serious side effects of tamoxifen are rare. However, it can cause blood clots
in the veins. Blood clots form most often in the legs and in the lungs. Women
have a slight increase in their risk of stroke.
Tamoxifen can cause cancer of the uterus. Your doctor should perform regular
pelvic exams. You should tell your doctor about any unusual vaginal bleeding
between exams.
When the ovaries are removed, menopause occurs at once. The side effects are
often more severe than those caused by natural menopause. Your health care
provider can suggest ways to cope with these side effects.
Biological therapy helps the
immune system
fight cancer. The immune system is
the body's natural defense against disease.
Some women with breast cancer that has spread receive a biological therapy
called Herceptin® (trastuzumab).
It is a
monoclonal antibody. It is made in the
laboratory and binds to cancer cells.
Herceptin is given to women whose lab tests show that a breast tumor has too
much of a specific protein known as HER2. By blocking HER2, it can slow or stop
the growth of the cancer cells.
Herceptin is given by vein. It may be given alone or with chemotherapy.
The first time a woman receives Herceptin, the most common side effects are
fever and chills. Some women also have pain, weakness, nausea, vomiting,
diarrhea, headaches, difficulty breathing, or rashes. Side effects usually
become milder after the first treatment.
Herceptin also may cause heart damage. This may lead to heart failure.
Herceptin can also affect the lungs. It can cause breathing problems that
require a doctor at once. Before you receive Herceptin, your doctor will check
for your heart and lungs. During treatment, your doctor will watch for signs of
lung problems.
|
You may want to ask your doctor these questions before having chemotherapy,
hormone therapy, or biological therapy:
-
What drugs will I be taking? What will they do?
-
If I need hormone treatment, would you recommend drugs or surgery to remove my
ovaries?
-
When will treatment start? When will it end? How often will I have treatments?
-
Where will I go for treatment? Will I be able to drive home afterward?
-
What can I do to take care of myself during treatment?
-
How will we know the treatment is working?
-
Which side effects should I tell you about?
-
Will there be long-term effects?
|
Your treatment options depend on the stage of your disease and these factors:
-
The size of the tumor in relation to the size of your breast
-
The results of lab tests (such as whether the breast cancer cells need hormones
to grow)
-
Whether you have gone through menopause
-
Your general health
Below are brief descriptions of common treatments for each stage. Other
treatments may be appropriate for some women. Clinical trials can be an option
at all stages of breast cancer. "The Promise of Cancer Research 10" section
has information about clinical trials.
Stage 0
Stage 0 breast cancer refers to lobular carcinoma in situ (LCIS) or ductal
carcinoma in situ (DCIS):
-
LCIS: Most women with LCIS do not have treatment. Instead, the doctor may
suggest regular checkups to watch for signs of breast cancer.
Some women take tamoxifen to reduce the risk of developing breast cancer.
Others may take part in studies of promising new preventive treatments.
Having LCIS in one breast increases the risk of cancer for both breasts. A very
small number of women with LCIS try to prevent cancer with surgery to remove
both breasts. This is a
bilateral prophylactic mastectomy. The surgeon usually
does not remove the underarm lymph nodes.
-
DCIS: Most women with DCIS have breast-sparing surgery followed by radiation
therapy. Some women choose to have a total mastectomy. Underarm lymph nodes are
not usually removed. Women with DCIS may receive tamoxifen to reduce the risk
of developing invasive breast cancer.
Stages I, II, IIIA, and Operable IIIC
Women with Stage I, II, IIIA, and operable (can treat with surgery) IIIC breast
cancer may have a combination of treatments. Some may have breast-sparing
surgery followed by radiation therapy to the breast. This choice is common for
women with Stage I or II breast cancer. Others decide to have a mastectomy.
With either approach, women (especially those with Stage II or IIIA breast
cancer) often have lymph nodes under the arm removed. The doctor may suggest
radiation therapy after mastectomy if cancer cells are found in 1 to 3 lymph
nodes under the arm, or if the tumor in the breast is large. If cancer cells
are found in more than 3 lymph nodes under the arm, the doctor usually will
suggest radiation therapy after mastectomy.
The choice between breast-sparing surgery (followed by radiation therapy) and
mastectomy depends on many factors:
-
The size, location, and stage of the tumor
-
The size of the woman's breast
-
Certain features of the cancer
-
How the woman feels about saving her breast
-
How the woman feels about radiation therapy
-
The woman's ability to travel to a radiation treatment center
Some women have chemotherapy before surgery. This is
neoadjuvant therapy
(treatment before the main treatment). Chemotherapy before surgery may shrink a
large tumor so that breast-sparing surgery is possible. Women with large Stage
II or IIIA breast tumors often choose this treatment.
After surgery, many women receive
adjuvant therapy.
Adjuvant therapy is
treatment given after the main treatment to increase the chances of a cure.
Radiation treatment can kill cancer cells in and near the breast. Women also
may have systemic treatment such as chemotherapy, hormone therapy, or both.
This treatment can destroy cancer cells that remain anywhere in the body. It
can prevent the cancer from coming back in the breast or elsewhere.
Stages IIIB and Inoperable IIIC
Women with Stage IIIB (including inflammatory breast cancer) or inoperable
Stage IIIC breast cancer usually have chemotherapy. (Inoperable cancer means it
cannot be treated with surgery.)
If the chemotherapy shrinks the tumor, the doctor then may suggest further
treatment:
-
Mastectomy: The surgeon removes the breast. In most cases, the lymph
nodes under the arm are removed. After surgery, a woman may receive radiation
therapy to the chest and underarm area.
-
Breast-sparing surgery: The surgeon removes the cancer but not the
breast. In most cases, the lymph nodes under the arm are removed. After
surgery, a woman may receive radiation therapy to the breast and underarm area.
-
Radiation therapy instead of surgery: Some women have radiation therapy
but no surgery. The doctor also may recommend more chemotherapy, hormone therapy, or both. This
therapy may help prevent the disease from coming back in the breast or
elsewhere.
Stage IV
In most cases, women with Stage IV breast cancer have hormone therapy,
chemotherapy, or both. Some also may have biological therapy. Radiation may be
used to control tumors in certain parts of the body. These treatments are not
likely to cure the disease, but they may help a woman live longer.
Many women have supportive care along with anticancer treatments. Anticancer
treatments are given to slow the progress of the disease. Supportive care helps
manage pain, other symptoms, or side effects (such as nausea). It does not aim
to extend a woman's life. Supportive care can help a woman feel better
physically and emotionally. Some women with advanced cancer decide to have only
supportive care.
Recurrent Breast Cancer
Recurrent cancer is cancer that has come back after it could not be detected.
Treatment for the recurrent disease depends mainly on the location and extent
of the cancer. Another main factor is the type of treatment the woman had
before.
If breast cancer comes back only in the breast after breast-sparing surgery,
the woman may have a mastectomy. Chances are good that the disease will not
come back again.
If breast cancer recurs in other parts of the body, treatment may involve
chemotherapy, hormone therapy, or biological therapy. Radiation therapy may
help control cancer that recurs in the chest muscles or in certain other areas
of the body.
Treatment can seldom cure cancer that recurs outside the breast. Supportive
care is often an important part of the treatment plan. Many patients have
supportive care to ease their symptoms and anticancer treatments to slow the
progress of the disease. Some receive only supportive care to improve their
quality of life.
Breast Reconstruction
Some women who plan to have a mastectomy decide to have breast reconstruction. Other women prefer to wear a breast form
(prosthesis). Others decide to do nothing. All of these options have pros and cons. What is right for one woman may not be right for another. What is important is that nearly every woman treated for breast cancer has choices.
Breast reconstruction may be done at the same time as the mastectomy, or later on. If you are thinking about breast reconstruction, you should talk to a plastic surgeon before the mastectomy, even if you plan to have your reconstruction later on.
There are many ways to reconstruct the breast. Some women choose to have implants. Implants may be made of saline or silicone. The safety of silicone breast implants has been under review by the Food and Drug Administration (FDA) for several years. If you are thinking about having silicone implants, you may want to talk with your doctor about the FDA findings. Your doctor can tell you if silicone implants are an option. You also can read information from the FDA on breast implants at
http://www.fda.gov/cdrh/breastimplants/.
You also may have
breast reconstruction with tissue that the plastic surgeon moves from another part of your body. Skin, muscle, and fat can come from your lower abdomen, back, or buttocks. The surgeon uses this tissue to create a breast shape.
Which type of reconstruction is best depends on your age, body type, and the type of surgery you had. The plastic surgeon can explain the risks and benefits of each type of reconstruction.
|
You may want to ask your doctor these questions about breast reconstruction:
- What is the latest information about the safety of silicone breast implants?
- Which type of surgery would give me the best results? How will I look afterward?
- When can my reconstruction begin?
- How many surgeries will I need?
- What are the risks at the time of surgery? Later?
- Will I have scars? Where? What will they look like?
- If tissue from another part of my body is used, will there be any permanent changes where the tissue was removed?
- What activities should I avoid? When can I return to my normal activities?
- Will I need follow-up care?
- How much will reconstruction cost? Will my health insurance pay for it?
|
Complementary and Alternative Medicine
Some women with breast cancer use
complementary and alternative medicine
(CAM):
-
An approach is generally called complementary medicine when it is used along
with standard treatment.
-
An approach is called alternative medicine when it is used instead of standard
treatment.
|
You may want to ask the doctor these questions before you decide to use CAM:
- What benefits can I expect from this approach?
- What are its risks?
- Do the expected benefits outweigh the risks?
- What side effects should I watch for?
- Will the approach change the way my cancer treatment works? Could this be harmful?
- Is this approach under study in a clinical trial? If so, who sponsors the trial?
- Will my health insurance pay for this approach?
|
Acupuncture,
massage therapy, herbal products, vitamins or special diets,
visualization, meditation, and spiritual healing are types of CAM.
Many women say that CAM helps them feel better. However, some types of CAM may
change the way standard treatment works. These changes could be harmful. And
some types of CAM could be harmful even if used alone.
Some types of CAM are expensive. Health insurance may not cover the cost.
NCI offers a booklet called
Thinking About Complementary and Alternative Medicine: A Guide for People with Cancer 12.
You also may request materials from the Federal Government's National Center
for Complementary and Alternative Medicine. You can reach their clearinghouse
toll-free at 1-888-644-6226 (voice) and 1-866-464-3615 (TTY). In addition, you
can visit the Center's Web site at http://www.nccam.nih.gov,
or send an email to info@nccam.nih.gov.
Nutrition and Physical Activity
It is important for women with breast cancer to take care of themselves. Taking
care of yourself includes eating well and staying as active as you can.
You need the right amount of calories to maintain a good weight. You also need
enough protein to keep up your strength. Eating well may help you feel better
and have more energy.
Sometimes, especially during or soon after treatment, you may not feel like
eating. You may be uncomfortable or tired. You may find that foods do not taste
as good as they used to. In addition, the side effects of treatment (such as
poor appetite, nausea, vomiting, or mouth sores) can make it hard to eat well.
Your doctor, dietitian, or other health care provider can suggest ways to deal
with these problems. Also, the NCI booklet
Eating Hints for Cancer Patients 8 has
many useful ideas and recipes.
Many women find they feel better when they stay active. Walking, yoga,
swimming, and other activities can keep you strong and increase your energy.
Exercise may reduce nausea and pain and make treatment easier to handle. It
also can help relieve stress. Whatever physical activity you choose, be sure to
talk to your doctor before you start. Also, if your activity causes you pain or
other problems, be sure to let your doctor or nurse know about it.
Follow-up Care
Follow-up care after treatment for breast cancer is important. Recovery is
different for each woman. Your recovery depends on your treatment, whether the
disease has spread, and other factors.
Even when the cancer seems to have been completely removed or destroyed, the
disease sometimes returns because undetected cancer cells remained somewhere in
the body after treatment. Your doctor will monitor your recovery and check for
recurrence of the cancer.
You should report any changes in the treated area or in your other breast to
the doctor right away. Tell your doctor about any health problems, such as
pain, loss of appetite or weight, changes in menstrual cycles, unusual vaginal
bleeding, or blurred vision. Also talk to your doctor about headaches,
dizziness, shortness of breath, coughing or hoarseness, backaches, or digestive
problems that seem unusual or that don't go away. Such problems may arise
months or years after treatment. They may suggest that the cancer has returned,
but they can also be symptoms of other health problems. It is important to
share your concerns with your doctor so problems can be diagnosed and treated
as soon as possible.
Follow-up exams usually include the breasts, chest, neck, and underarm areas.
Since you are at risk of getting cancer again, you should have mammograms of
your preserved breast and your other breast. You probably will not need a
mammogram of a reconstructed breast or if you had a mastectomy without
reconstruction. Your doctor may order other imaging procedures or lab tests.
Facing Forward Series: Life After
Cancer Treatment 13 is an NCI booklet for people who have completed their
treatment. It answers questions about follow-up care and other concerns. It has
tips for making the best use of medical visits. It also suggests ways to talk
with the doctor about creating a plan of action for recovery and future health.
Sources of Support
Learning you have breast cancer can change your life and the lives of those close to you. These changes can be hard to handle. It is normal for you, your family, and your friends to have many different and sometimes confusing feelings.
You may worry about caring for your family, keeping your job, or continuing daily activities. Concerns about treatments and managing side effects, hospital stays, and medical bills are also common. Doctors, nurses, and other members of the health care team can answer questions about treatment, working, or other activities. Meeting with a social worker, counselor, or member of the clergy can be helpful if you want to talk about your feelings or concerns. Often, a social worker can suggest resources for financial aid, transportation, home care, or emotional support.
Friends and relatives can be very supportive. Also, you may find it helps to discuss your concerns with others who have cancer. Women with breast cancer often get together in support groups to share what they have learned about coping with their disease and the effects of their treatment. It is important to keep in mind, however, that each woman is different. Ways that one woman deals with cancer may not be right for another. You may want to ask your health care provider about advice you receive from other women with breast cancer.
Several organizations offer special programs for women with breast cancer. Women who have had the disease serve as trained volunteers. They may talk with or visit women with breast cancer, provide information, and lend emotional support. They often share their experiences with breast cancer treatment, breast reconstruction, and recovery.
You may be afraid that changes to your body will affect not only how you look but also how other people feel about you. You may worry that breast cancer and its treatment will affect your sexual relationships. Many couples find it helps to talk about their concerns. Some find that counseling or a couples' support group can be helpful.
Information Specialists at 1-800-4-CANCER and at LiveHelp 1
(http://www.cancer.gov) can help you locate programs, services, and publications. Also, you may want to read the NCI fact sheet
"National Organizations That Offer Services to People With Cancer and Their Families 14."
The Promise of Cancer Research
Doctors all over the country are conducting many types of clinical trials
(research studies in which people volunteer to take part). They are studying
new ways to prevent, detect, diagnose, and treat breast cancer. Some are also
studying therapies that may improve the quality of life for women during or
after cancer treatment.
Clinical trials are designed to answer important questions and to find out
whether new approaches are safe and effective. Research already has led to
advances and researchers continue to search for more effective methods for
dealing with cancer.
Women who join clinical trials may be among the first to benefit if a new
approach is effective. And even if people in a trial do not benefit directly,
they still make an important contribution by helping doctors learn more about
breast cancer and how to control it. Although clinical trials may pose some
risks, researchers do all they can to protect their patients.
If you are interested in being part of a clinical trial, talk with your doctor.
Trials are available for all stages of breast cancer. You may want to read the NCI booklet Taking Part in Cancer Treatment Research Studies 15. It explains how clinical trials are carried out and explains their possible benefits and risks.
NCI's Web site includes a section on clinical trials at http://www.cancer.gov/clinicaltrials.
It has general information about clinical trials as well as detailed
information about specific ongoing studies of breast cancer. Information
Specialists at 1-800-4-CANCER or at
LiveHelp 1 at http://www.cancer.gov/cis can
answer questions and provide information about clinical trials.
Scientists are looking for drugs that may prevent breast cancer. For example,
they are testing several different drugs that lower hormone levels or prevent a
hormone's effect on breast cells.
In one large study, the drug tamoxifen reduced the number of new cases of
breast cancer among women who were at an increased risk of the disease. Doctors
are studying whether the drug raloxifene is as effective as tamoxifen. This
study is called STAR (Study of Tamoxifen and Raloxifene). Results will be
available in late 2006.
At this time, mammograms are the most effective tool we have to detect changes
in the breast that may be cancer. In women at high risk of breast cancer,
researchers are studying the combination of mammograms and ultrasound.
Researchers are also exploring
positron emission tomography
(PET) and other
ways to make detailed pictures of breast tissue.
In addition, researchers are studying
tumor markers.
Tumor markers may be found
in blood, in urine, or in fluid from the breast (nipple
aspirate).
High amounts
of these substances may be a sign of cancer. Some markers may be used to check
breast cancer patients for signs of disease after treatment. At this time,
however, no tumor marker test is reliable enough to be used routinely to detect
breast cancer.
Ductal lavage
also is under study. This technique collects cells from breast
ducts. A liquid flows through a catheter (very thin, flexible tube) into the
opening of a milk duct on the nipple. The liquid and breast cells are withdrawn
through the tube. A pathologist checks the cells for cancer or changes that may
suggest an increased risk of cancer.
Researchers are studying many types of treatment and their combinations:
-
Surgery: Different types of surgery are being combined with other treatments.
-
Radiation therapy: Doctors are studying whether radiation therapy can be used
instead of surgery to treat cancer in lymph nodes. They are looking at the
effectiveness of radiation therapy to a larger area around the breast. In women
with early breast cancer, doctors are studying whether radiation therapy to a
smaller part of the breast may be helpful.
-
Chemotherapy: Researchers are testing new anticancer drugs and doses. They are
working with drugs and combinations of drugs. They are looking at new drug
combinations before surgery. They are also looking at new ways of combining
chemotherapy with hormone therapy or radiation therapy.
-
Hormone therapy: Researchers are testing several types of hormone therapy,
including aromatase inhibitors.
-
Biological therapy: New biological treatments also are under study. For
example, researchers are studying cancer
vaccines
that help the immune system
kill cancer cells.
In addition, researchers are looking at ways to lessen the side effects from
treatment, such as lymphedema from surgery. They are looking at ways to reduce
pain and improve quality of life. One method under study is sentinel lymph node
biopsy. Today, surgeons have to remove many lymph nodes under the arm and check
each of them for cancer. Researchers are studying whether checking only the
node to which cancer is most likely to spread (sentinel lymph node) will allow
them to predict whether cancer has spread to other nodes. If this new procedure
works as well as standard treatment, surgeons may be able to remove fewer lymph
nodes. This could reduce lymphedema for many patients.
National Cancer Institute Information Resources
You may want more information for yourself, your family, and your doctor. The
following National Cancer Institute (NCI) services are available to help you.
Telephone
The NCI's Cancer Information Service (CIS) provides accurate, up-to-date
information on cancer to patients and their families, health professionals, and
the general public. Information Specialists translate the latest scientific
information into understandable language and respond in English, Spanish, or on
TTY equipment. Calls to the CIS are free.
Telephone: 1-800-4-CANCER
(1-800-422-6237) TTY: 1-800-332-8615
Internet
The NCI's Web site (http://www.cancer.gov) provides information
from numerous NCI sources. It offers current information on cancer prevention,
screening, diagnosis, treatment, genetics, supportive care, and ongoing
clinical trials. It has information about NCI's research programs and funding
opportunities, cancer statistics, and the Institute itself. Information
Specialists provide live, online assistance through
LiveHelp 1 at http://www.cancer.gov/cis.
National Cancer Institute Publications
National Cancer Institute (NCI) publications can be ordered by writing to the
address below:
Publications Ordering Service
National Cancer Institute
Suite 3035A
6116 Executive Boulevard, MSC 8322
Bethesda, MD 20892-8322
Many NCI publications can be viewed, downloaded, and ordered from
http://www.cancer.gov/publications 16 on the Internet. In addition, people
in the United States and its territories may order these and other NCI
publications by calling the NCI's Cancer Information Service at 1-800-4-CANCER.
Publications About Breast Changes and Breast Cancer
What You Need To Know About™ Breast Cancer 17
(also available in Spanish: Lo que usted necesita saber sobre™ el cáncer de
seno 18)
Understanding Breast Changes: A
Health Guide for Women 19
"Cambios en el seno y el riesgo de
desarrollar cancer 20"
Publications About Cancer Treatment and Support
Surgery Choices for Women with
Early-Stage Breast Cancer 21
Radiation Therapy and You: A Guide
to Self-Help During Cancer Treatment 5 (also available in
Spanish: La radioterapia y usted: Una guía de autoayuda durante el tratamiento
del cáncer)
Chemotherapy and You: A Guide to
Self-Help During Cancer Treatment 6 (also available in Spanish:
La quimioterapia y usted: Una guía de autoayuda durante el tratamiento del
cáncer)
Biological Therapy: Treatments That Use
Your Immune System to Fight Cancer 7
Eating Hints for Cancer Patients: Before, During
& After Treatment 8 (also available in Spanish: Consejos de
alimentación para pacientes con cáncer: Antes, durante y después del
tratamiento)
Understanding Cancer Pain 22 (also
available in Spanish: El dolor relacionado con el cáncer 23)
Pain Control: A Guide for People with Cancer and
Their Families 24 (also available in Spanish: Control del dolor:
Guía para las personas con cáncer y sus familias)
Get Relief from Cancer Pain
Thinking About Complementary and Alternative Medicine: A Guide for People with Cancer 12
"Biological Therapies for Cancer:
Questions and Answers 25" (also available in Spanish: "Terapias
biológicas: el uso del sistema inmune para tratar el cáncer 26")
"How To Find a Doctor or Treatment
Facility If You Have Cancer 27" (also available in Spanish: "Cómo
encontrar a un doctor o un establecimiento de tratamiento si usted tiene
cáncer 28")
"National Organizations That Offer
Services to People With Cancer and Their Families 14" (also
available in Spanish: "Organizaciones nacionales que brindan servicios a las
personas con cáncer y a sus familias 29")
Publications About Living With Cancer
Advanced Cancer: Living Each Day 30
Facing Forward Series: Life After
Cancer Treatment 13 (also available in Spanish:
Siga adelante: la
vida después del tratamiento del cáncer 31)
Facing Forward Series: Ways You Can Make a
Difference in Cancer 32
Taking Time: Support for People with Cancer and
the People Who Care About Them 33
When Cancer Recurs: Meeting the Challenge 34
Publications About Clinical Trials
Taking Part in Cancer Treatment Research Studies 15
Taking Part in
Clinical Trials: Cancer Prevention Studies: What Participants Need To Know 35
(also available in Spanish: La participación en los estudios clínicos: estudios
para la prevención del cáncer)
|
