Fatality Assessment and Control Evaluation (FACE) Program |
|
A Carpenter Died after Falling 20 Feet From a Roof. |
|
|||||||||||
SummaryA 40-year-old Hispanic carpenter working for a general contracting company fell from a roof on January 20, 2006. The victim was part of a three-person crew that was installing plywood roof decking to a structural steel frame. The victim and his two coworkers were not using fall protection while working at an elevation of approximately 20 feet. One worker cut sheets of plywood on an adjacent flat structure, while the victim and the other coworker attached the decking to an arched roof using screw guns. The fall was not witnessed because the victim’s coworkers were involved in their own tasks and the job superintendent was inside the structure. Coworkers noticed the fall and immediately called 911. Emergency medical service (EMS) arrived in less than 15 minutes and transported the victim to a local hospital where he was pronounced dead approximately one hour after the incident occurred. Oklahoma Fatality Assessment and Control Evaluation (OKFACE) investigators concluded
IntroductionOn January 20, 2006, a 40-year-old Hispanic carpenter died after falling 20 feet from a roof that was under construction. OKFACE investigators were notified of the incident and an interview with company officials was conducted on February 10, 2006. OKFACE investigators reviewed the death certificate and reports from news agencies, the Medical Examiner, and the Occupational Safety and Health Administration (OSHA). Employer: The victim was employed by a construction general contractor. The company had been in business for 100 years and employed 25 full-time workers. There were no written task-specific safe work procedures or machine-specific safe operating instructions. The company did not have a safety and health committee. A company vice president acted as the safety director. The company had a written safety and health program available only in English. The written safety and health program did contain a policy on safely working from elevations. The employer’s safety handbook addressed floor openings and open sides, personal protective equipment, and safety responsibilities of workers, job foremen, and project superintendents. The safety handbook stated “The employee is responsible for wearing appropriate personal protective equipment in operations where there is exposure to hazardous conditions, or where need is indicated to reduce hazards.” Job foremen and project superintendents were in leadership roles on jobsites and, according to the employer’s handbook, were responsible for making sure personal protective equipment was available and used. The safety handbook required workers to use and maintain all safety devices provided. It also specified that lifelines, safety belts, and lanyards be used only for employee safeguarding. The employer had signed and dated records on file to verify that fall protection hazards were addressed during onsite safety meetings. Victim: The 40-year-old Hispanic male victim had worked for the company for two years at the time of the incident. The victim had been living in the United States for 20 years and worked as a carpenter during that time. His primary language was Spanish; he could read and speak both English and Spanish well. The victim’s direct supervisor spoke only English. English was also the primary language of the victim’s immediate coworkers. Training: The safety director or a job superintendent provided weekly toolbox safety meetings to employees in English; Spanish translations were not provided. The company provided task-specific training for all tasks performed. The job superintendent at the time of the incident and at least one other job superintendent had attended an OSHA 10-hour training course and were aware of the requirements for fall protection for employees constructing a leading edge more than six feet above the ground or a lower level. The employer did cover the topic of fall hazards during documented safety meetings. Incident Scene: The incident occurred at a commercial construction site. The company had been working at the site for five months; five general contractor employees and 20 subcontractor employees were working at the time of the incident. Weather: On the day of the incident, the weather conditions were dry, but cool and windy.
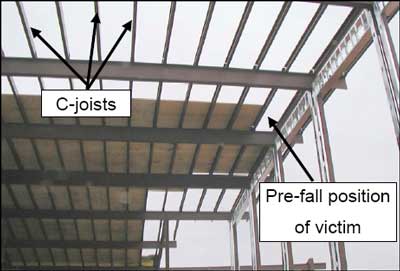
Back to TopInvestigationWhen the crew arrived at 7:00 a.m., the job superintendent instructed them to use an aerial lift to access the roof at approximately 7:45 a.m. and install plywood decking on the framed roof. Installing roof decking was considered a common and routine activity for these workers. Installing roof decking is referred to as leading edge work in which the edge of a floor, roof, or deck changes as additional materials are installed. The crew was working on top of a structural steel frame that formed a broad arch shaped roof over a concrete slab. The east and west corners of the steel frame were 17 feet, 8 inches tall and arched to 21 feet, 9 inches in the center. The north roof edge, from which the victim fell, was approximately 20 feet tall. The front edge of the roof was located to the north and the roof extended southward until stopping at a concrete wall (Figure 1). A rough-terrain forklift had been used to lift 5/8-inch thick, 4-foot by 8-foot sheets of plywood to a flat metal roof located just to the west of the work area. The work area was in view of the job superintendent’s office that was located 100-150 feet north of the structure. Safety harnesses were located in the office, but no anchors were available. The crew was instructed to install roof decking from the southwest corner of the roof, completing each south to north row as they worked towards the east roof edge. One of the three crew members cut plywood sheets from the adjacent flat roof and distributed them to the victim and another crew member, who used screw guns to secure them to the C-joists that ran west to east (Figure 2). The crew was performing work according to the supervisor’s instructions. Witness statements indicated that crews had used fall protection devices in the past on previous job sites, but they were not in use at the time of the incident. The superintendent was aware that fall protection was not being used. Physical evidence collected during the investigation indicated that the victim’s weight was over the piece of plywood during the incident when the plywood and the victim fell. Two screws had already been placed into the plywood before the fall occurred. One screw was completely drilled into the plywood and C-joist and the second screw was partially in when it broke. When the plywood was found, a very small section of the board with the completely drilled screw was separated from the rest and still attached to the C-joist. The employer did not have data regarding the load bearing capacity of the plywood or the decking screw’s resistance to sheering forces. During this decking operation, two pieces of plywood met on top of the 2 ½-inch wide C-joist, leaving 1 ¼-inch of plywood-joist overlap when perfectly cut. As the workers installed the plywood decking, there was a period of time when there were no or few screws engaged between the plywood and joists. During these times, shifting the plywood could cause it to fall off of narrow joists and result in the worker falling, particularly if the worker’s weight was over the plywood. The victim was last seen on the roof by the other carpenter who was installing the decking. The victim and his coworker had a conversation while the victim was sitting and holding a 4- foot by 29 ½-inch piece of plywood on his lap. The victim’s coworker returned to his duties after the conversation and the fall was not witnessed. The incident occurred at 10:48 a.m. The plywood and victim were found approximately 20 feet below his work area on the concrete slab. The victim had fallen in the 21 ½-inch space between two C-joists located on the north side of the roof. Coworkers immediately called 911 and EMS arrived less than fifteen minutes after the call was placed. The victim was transported by EMS to a local hospital where he was pronounced dead approximately one hour after the incident occurred.
Cause of DeathThe Medical Examiner’s report listed the cause of death as multiple blunt force trauma. Back to TopRecommendations/DiscussionRecommendation # 1: Employers should ensure that employees working from surfaces elevated more than six feet above a lower surface or the ground are provided with and use fall restraints, such as a fall arrest system, guardrail, or safety net.Discussion: OSHA regulations require employees constructing a leading edge six feet or
more above a lower level to be protected from falling by guardrail systems, safety net
systems, or a personal fall arrest system. A personal fall arrest system includes a full-body
harness, lanyard, connectors, and appropriate anchorage points. Harnesses, as part of a
personal fall protection system, were available the day the incident occurred, but were not
used. The General Duty Clause of the Occupational Safety and Health Act of 1970 requires
employers to furnish a place of employment that is free from recognized hazards and
requires employers and employees alike to comply with occupational safety and health
standards. During this incident, the use of a safety net or personal fall arrest system may
|
||||||||||||