Fatality Assessment and Control Evaluation (FACE) Program |
|
A Lumberyard Forklift Operator Died after Being Crushed Between Two Railcar Couplings. |
| |||||||||||
SummaryOn September 24, 2004, a 31-year-old forklift operator for a lumber company died when he was crushed between the couplings of two railcars. The victim was working with two other employees to position and “couple,” or connect, the railcars for loading and shipping. One worker was operating a forklift, which was being used to push one loaded railcar toward a second, stationary, empty car, while the victim and the third worker acted as spotters. After noticing that the couplers (devices to connect the railcars) were not aligned properly and would not connect, the decedent pulled himself up the ladder on the moving car and attempted to kick the coupler into position. The two railcars hit, causing the victim to fall between them. He was subsequently crushed when the second railcar hit the railcar stop and recoiled back toward him. The second spotter immediately called for assistance by radio and emergency medical services (EMS) transported the victim to a local hospital where he was pronounced dead on arrival. Oklahoma Fatality Assessment and Control Evaluation (OKFACE) investigators concluded that to help prevent similar occurrences, employers should:
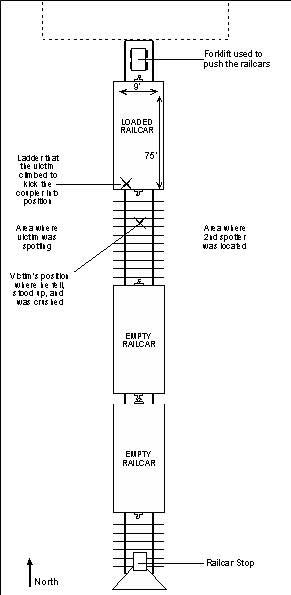
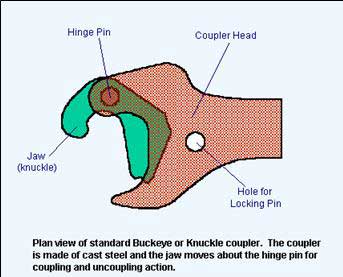
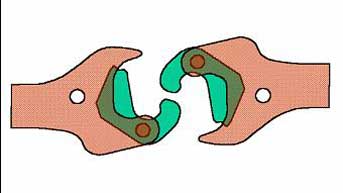
IntroductionOn September 24, 2004, a 31-year-old forklift operator for a lumber company was crushed by the couplings of two railroad cars, while he and two other employees were attempting to position the cars in the shipping area. OKFACE investigators were notified of the incident and an interview with company officials was conducted on December 1, 2004. OKFACE investigators reviewed the death certificate and reports from the Medical Examiner, investigating law enforcement officer, and the Occupational Safety and Health Administration (OSHA). Employer:The victim was employed in the shipping area of a lumber company, which had been in business for over nine years and employed approximately 116 full-time employees. The company had a comprehensive written safety and health program, which included a labor/management safety committee. The company had task-specific, written standard operating procedures in place, as well as machine-specific procedures for all equipment. The company had two job classifications within the shipping area, shipping forklift operator and shipping car loader. They shipped an average of 20-25 railcars of lumber each month. Victim:The 31-year-old male victim had been in the lumber business for 3½ years and had over 1½ years of experience in his particular occupation. He was employed as a shipping forklift operator and had duties that included loading trucks and railroad cars with lumber. Training:Weekly safety meetings were conducted for all employees with a monthly team safety meeting included. The company conducted all training through the use of classroom, video, and on-the-job techniques. Machine operators were required to be certified, licensed, and tested for proficiency. New employees were provided with an orientation that included 4½ hours of safety instruction and additional on-the-job training. The victim did receive on-the-job training, but there was no record of what was specifically covered and the employees who instructed him were no longer with the company. The victim also had been involved with a behavior-based safety program where he had received 4-5 weeks of training on hazard recognition and performed monthly observations. Many job hazard analyses had been done on the company’s work practices, but there was not one for moving railcars. The company kept documentation of all training, safety meetings, and required certifications on file. Incident Scene:The incident occurred on a dead end rail spur, which had a covered, open-sided loading shed and an outside railcar stop. Empty railcars were delivered to the plant by the railroad, and the lumber employees loaded and moved the cars around on the spur line as needed. Railcars were loaded in the shed area and then pushed outside by a forklift, where up to four cars would be connected. On the day of the incident, two empty railcars sat outside on the spur line, while a loaded car was being pushed out of the shed. The incident occurred near the end of the first shift, at approximately 5:00 p.m. The victim and his two coworkers were the only employees in the immediate area. Weather:The weather conditions were dry and clear with a moderate temperature. The walking and working surfaces of the loading area, rail spur area, and yard were dry. Back to TopInvestigationOn the day of the incident, a three-person crew in the lumber shipping area was working to position railcars to fulfill an order that had been received that afternoon. Railcars were not loaded in a particular order, but there were designated railcars for designated loads of lumber. There were four railcars on the spur line; one was north of the loading shed and was not a factor in the incident (Figure 1). Two empty cars were sitting outside on the spur line, south of the loading shed and just north of the railcar stop. The fourth railcar, which was 9-feet wide, 75-feet long, and loaded with 177,600 pounds of lumber, was being pushed south out of the loading shed. The southernmost railcar needed to be loaded, so the plan was to connect the loaded railcar to the two empty ones and pull all three back north into the loading area. The incident occurred during the process of connecting the three railcars. One employee was driving the forklift that was pushing the loaded railcar. The company used their heavy, rubber-tired forklifts, which operated on concrete and traveled no faster than five miles per hour, for pushing and pulling railcars. The other two employees were acting as spotters, immediately adjacent to the coupling devices on the railcars; the decedent was on the west side of the rail spur and the other worker was on the east side. Aside from hand signals and shouting, the spotters had no other means of communicating with the forklift operator. As the forklift operator moved the railcar at approximately two to three miles per hour and it approached the nearest stationary railcar, the decedent noticed that the coupling devices (Figures 2 and 3) were not aligned properly and would not connect. He proceeded to run up to the moving loaded railcar and climb the ladder on the end (out of the forklift operator’s line of sight). He stood off to the side on the ladder and began trying to realign the coupler by kicking it with his foot. Meanwhile, the other spotter was yelling at the victim to get out of there. Before the decedent could get out of the way, the railcars collided and bounced apart. The couplings were still misaligned, so the railcars did not connect. The impact of the hit caused the decedent to fall off the ladder and onto the ground between the couplings. The force caused the empty railcars to collide with the rail stop and recoil back toward the victim, who was now standing between the couplings. The recoiling empty car slammed back into the loaded car, crushing the decedent in between the two couplings.
The second spotter yelled for the forklift operator to pull the railcar back north and also radioed to the main office for help. Upon separating the railcars, the decedent fell diagonally across the east side of the tracks and was treated there by first responders. Company management called 911, responded to the scene within two minutes, and initiated first aid. Emergency medical services arrived on scene approximately 15 minutes later and transported the victim to the nearest hospital where he was pronounced dead on arrival. Cause of DeathThe Medical Examiner’s report listed the cause of death as blunt trauma of the chest and abdomen. Back to TopRecommendations/DiscussionRecommendation # 1: Employers should ensure that employees do not enter the space between railcars that are being moved, including during procedures of coupling and uncoupling.Discussion: The area between moving railcars should be considered hazardous and should not be entered. The Federal Railroad Administration recommends a minimum distance of 50 feet between railcars for safe entry by workers. Employers should continually educate their employees who work around railcars on how to move and maneuver around them. Employees should be instructed and monitored on not using outdated practices that are shown to be dangerous, such as kicking couplers. In situations where couplings are observed to be misaligned, workers should stop the operation, separate the railcars by at least 50 feet, and ensure that the railcars are completely stopped before entering the area and realigning the couplings.
| ||||||||||||