Fatality Assessment and Control Evaluation (FACE) Program |
|
Forklift Driver Pinned Under an Overturned Forklift Dies |
|
||||||||||||||
SummaryOn February 17, 2006, a 46-year-old Hispanic male utility man was killed when he backed an 8,670-pound, propane-powered Toyota Model 426FGCU25 forklift over the edge of a loading dock, which then overturned and landed on him. The dock plate had two standard guardrails on either side with a chain across the dock opening. There were no witnesses to the events prior to the incident or to the incident itself. The decedent was discovered when another employee traveling through the area noticed the forklift’s lights shining on the wall and the truck’s forks up and against the wall in the truck well. This employee summoned others to the area when he discovered the decedent pinned face down between the concrete floor and the overhead guard. Several employees manually lifted the forklift enough to move the decedent from under it. It is assumed that the forklift was traveling in reverse, because neither the forks nor the mast appeared bent, as would have been the case if he had been traveling forward and drove off of the dock edge. It is unknown if he jumped or was thrown from the operator's seat. 911 was called and paramedics pronounced him dead at the scene.
Recommendations:
IntroductionOn February 17, 2006, a 46-year-old Hispanic male utility man was killed when he was pinned under an overturned forklift. On February 17, 2006, MIFACE investigators were informed by the Michigan Occupational Safety and Health Administration (MIOSHA) personnel who had received a report on their 24-hour-a-day hotline, that a work-related fatal injury had occurred and the decedent had died on that day. On February 21, 2006, MIFACE interviewed the firm's Human Resource Manager, Assistant Plant Manager and several of the decedent's coworkers, including union officials. During the course of writing this report, the police report, medical examiner's report, and MIOSHA file and citations were reviewed. The decedent's employer granted MIFACE permission to view the incident site and take incident site pictures and pictures of the damaged forklift, which had been placed in storage. Figures 1, 4, 6, and 7 are courtesy of the MIOSHA compliance officer and have been modified to remove identifiers. Figures 2, 3, and 5 were taken at the time of the MIFACE site visit. The decedent's employer conducted heat treat operations, and manufactured and processed ball bearings for the automotive industry. The firm also assembled small parts. The firm employed approximately 250 people, had a three-shift operation, and had a unionized workforce. Twelve individuals had the same job classification as the decedent, utility man. The decedent was one of approximately 60 people who worked third shift. On the night of the incident, there were two shift foremen and three to four utility persons, in addition to the other third shift workers. The decedent was a temporary employee who was employed full-time as an hourly employee. He had been a utility man for the past five months. A utility person was assigned specified job assignments, such as cleaning bathrooms, emptying dumpsters, etc. The utility person would also have special assignments as determined by the shift foreman. The decedent's job tasks included driving a forklift, but driving a forklift was not his primary responsibility. He had previous experience at another firm operating a forklift. He wore glasses. The decedent's work shift began at 11:00 p.m. and ended at 7:00 a.m. He had worked first shift for the previous five months. He had ended working first shift on a Friday afternoon, and begun working third shift two days later on a Sunday evening. The incident occurred on the fourth day of his third shift work. Fellow employees interviewed stated that the decedent liked working third shift. The firm had a written health and safety program, including a joint health and safety committee. Up until approximately one and one-half weeks prior to the incident, the occupational health nurse had primary responsibility for the safety program. The nurse maintained training databases, arranged for training videos and facilitated the safety committee. The safety committee met monthly, and the results were shared with upper management. The safety committee supplied upper management with a checklist to "buddy up" with a knowledgeable person to assess health and safety items in a department. Accidents, injuries, and near misses were to be reported to senior management so proactive efforts to prevent a future injury/loss incident could be implemented. The firm’s health and safety policy required safety glasses with eye shields and hearing protection in certain designated areas. Employee health and safety training was conducted on each work shift by the occupational health nurse and the union. Forklift training was conducted for all forklift operators. The decedent had successfully completed both the written and practical tests and was in possession of a valid operator permit. English was the primary language of the decedent. At the conclusion of the MIOSHA investigation, the firm was issued an Other-than-Serious citation: MIOSHA General Industry Safety Standard - Powered Industrial Trucks, Part 21.
The MIOSHA General Industry compliance officer made two safety recommendations to the company:
Back to TopInvestigationThe forklift involved in the incident was a propane-powered Toyota Model 426FGCU25 weighing 8,670 pounds. The forklift's rear tires were smooth and the front tires had treads. The forklift had an overhead guard and was equipped with a functional seat belt system (Figure 2, circle). The deceased operated the forklift in all areas of the plant and was familiar with the plant's layout. The forklift controls were not clearly labeled. The assistant plant manager stated that the firm's forklift training included a requirement that seatbelts must be worn when operating a forklift equipped with a seatbelt. Daily forklift safety checks were performed and verbal information passed on for the equipment concerning inspection and maintenance. No documentation was maintained for daily operator checks. Employees stated that forklift maintenance was timely; when a machine was taken out of service, a rental machine was acquired.
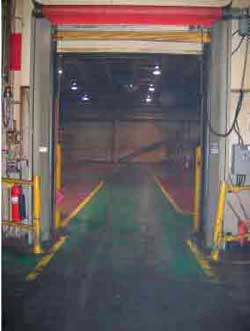
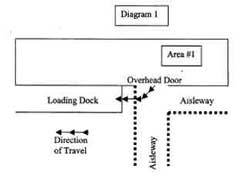
The incident occurred at a loading dock. Standard guardrails were installed six inches away from the edges of the 6-foot wide loading dock plate. The loading dock floor was approximately four feet below the plant floor. Adjacent to the loading dock was an 8-foot-wide overhead door leading to Area #1. On either side of the overhead door were guardrails protecting the entrance to the door (Figures 3 and 4 and Diagram 1). At the time of the incident, the loading dock entrance had a chain across the opening.
On the day before the incident, Area #1 had a roof leak and water was entering the plant area via the leak. To catch the dripping water, the decedent was directed to take a palletized empty 27-inch wide x 17-inch tall x 28-inch long heavy cardboard box, line it with a plastic bag, and take it to Area #1, mop up the leak, and place the box under the leak. Area #1 also stored other empty similarly sized palletized cardboard boxes. The next evening, the decedent told the supervisor that he had found two additional areas with roof leaks and would place a box with liner in those areas as he had done the night before. The decedent had taken an authorized work break - several employees had seen him and talked with him in the break room and he appeared alert at that time. After the break, he climbed into the forklift and drove away. Shortly thereafter, a coworker needed an empty cardboard box for parts. He climbed aboard a forklift and drove to Area #1 to retrieve a box/pallet. He passed by the loading dock but did not see the decedent. Upon returning to his workstation, he noticed the forklift's lights shining on the wall and the truck's forks up and against the wall in the truck well. He stopped and went to the edge of the loading dock and after seeing the decedent's leg, he ran for help. The forklift was still running when he found the decedent. The decedent was found laying face down on the cement floor with the left rear support of the overhead guard lying across his back. A number of employees returned and one of these coworkers turned the forklift engine off. The coworkers were able to momentarily manually lift the forklift so that someone could pull the decedent from underneath the overhead guard. Preliminary first aid was started and continued until emergency response personnel arrived. Emergency response arrived and declared the decedent deceased at the scene.
Investigation of the incident scene noted that there were no skid or brake marks on the plant floor. The decedent was not carrying a load at the time of the incident. It appears that the forklift was driven off the dock while traveling in reverse based upon the position of the truck. Neither the forks nor the mast appeared bent, as would have been the case if he had been traveling forward and drove off of the dock edge. The counterweight attachment bolt sheared, and the counterweight had detached from the machine and was lying to the side. A fresh impact point was noted in the cement of the truck well approximately three and one-half feet from the top of the loading dock. The left rear tire was approximately five and one-half feet from the edge of the loading dock platform. This distance suggests that the forklift was traveling at a fairly fast rate. The barrier chain across the dock opening was sheared off. The dock boarding plate had a significant bend on the edge and the chain's fastening loop was sticking straight out (Figures 5 and 6). The forks were facing upward and were leaning against the truck well wall. The forklift fork gouged the wall at a height of approximately 103 inches. A scrape on the wall began approximately 8 feet above the loading dock floor and ended at approximately 44 inches above the floor. It is thought that the scrape was made when trying to lift the forklift from the decedent's back. The event was unwitnessed. It is unknown what caused the decedent to back off the end of the loading dock, but a likely scenario is that he was driving in reverse at a significant rate of speed. The damaged/bent dock plate and the location of the machine, several feet from the loading dock edge, after falling to the dock floor supports this hypothesis. A less likely hypothesis is that the decedent was moving slowly, and as the forklift's rear wheels came off of the dock edge, he panicked. Forgetting to place the gearshift in forward, he applied the gas in an attempt to move the machine forward. As the forklift was still in reverse, the machine would have traveled off of the loading dock plate. This scenario is less likely because it is unlikely that the forklift would have traveled so far from the edge under this scenario.
It is unknown whether the decedent attempted to jump from the operator's seat as the forklift proceeded over the dock plate to the truck well floor or whether he was thrown from the forklift as it fell. An employee who worked with the decedent stated that the decedent had difficulty with his peripheral vision as he had to turn his head to align with the center of travel when he drove the forklift. He also stated that he had seen the decedent hit a wall with a hopper while moving it, but there had been no damage or injuries and he did not report the incident to management. At the conclusion of the MIOSHA investigation, the company reviewed the powered industrial truck permits of all employees who operated a forklift and surveyed the operators to determine if operator restrictions needed to be noted on the permit. The firm has issued new powered industrial truck operator permits to employees who wear corrective lenses with the permit indicating that glasses must be worn during truck operation. Back to TopCause of DeathThe cause of death as listed on the death certificate was multiple injuries. Toxicology was negative for alcohol and other screened drugs. Recommendations/DiscussionEmployers should install drop-off protection capable of withstanding forklift impact on a loading dock entrance when the dock entrance is near a normal path of travel for a forklift or pedestrian.A barrier chain was the only device used to protect the loading dock platform. Loading docks that are vacant can create a hazardous situation for dock personnel, material handlers and pedestrians in the area. Providing drop-off protection at the platform by installing a safety barrier that can be manually positioned and removed by a single forklift operator can be a solution for this problem. When the drop-off protection is in position, it can also provide a constant visual safety reminder of the dock area. There are several manufacturers that provide easy-to-use and relatively inexpensive drop-off protection devices to eliminate this hazard and prevent an injury.
| |||||||||||||||