Investigation: # 03MI029
Co-Owner of Metal Forge Shop Dies When an Ejected Piece of Steel Used as a Stop Block in a Full Revolution Press Strikes Him in the Chest
|
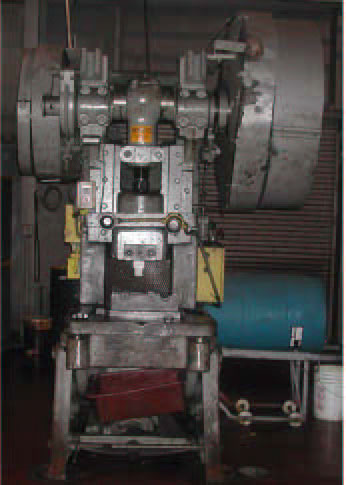
| Figure 1. “Bender” press |
RECOMMENDATIONS
INTRODUCTION
On April 3, 2003, a 62-year-old forging company co-owner died when a piece of steel struck him in the chest when a full revolution press cycled. On Friday, April 4, 2003, MIFACE investigators were notified of the fatality by a newspaper article. Later that day, MIFACE was informed by the Michigan Occupational Safety and Health Act (MIOSHA) personnel, who had received a report on their 24 hour-a-day hotline, that a work-related fatal injury had occurred on April 3, 2003. On June 5, 2003, the MIFACE researcher interviewed the co-owner who was also working in the shop at the time of the incident. At the time of the interview, the co-owner escorted the MIFACE researcher into the shop where she was able to observe and take pictures of the steel that struck the victim, the die and press involved in the incident. The company permitted a follow-up visit by the MIFACE researcher to photograph the safety block and press guard. During the course of writing the report, the autopsy results, death certificate, police report, and the MIOSHA citations were obtained.
The company was issued 4 alleged serious citations. Three citations were for violations of Part 24, Mechanical power Presses. Part 24, Rule 2463 requires the distance between each two-hand trip and point of operation be greater than the distance determined by the formula prescribed in Rule 2463(8)(c) on full revolution clutch presses; the distance between the trips and the press did not meet the minimum safety distance. Part 24, rule 2476 requires that dies be fastened securely; the upper dies of the press were inadequately secured. The third citation involving Part 24 was a violation of rule 2477(4) that required means to prevent cycling of the press during die repair with safety blocks in place; the firm was not enforcing lockout when the victim was making repairs to dies in the press and using a die block (4” long, 1 7/8” diameter cylindrical steel referred to in Summary) that was not interlocked. The fourth citation concerned the Control of Hazardous Energy Sources, Part 85, Rule 1910.147(c)(4)(i) adopted by Rule 8502 required the development, documentation and utilization of procedures for the control of potentially hazardous energy when employees are engaged in service or maintenance of machines or equipment where unexpected energization, start-up or release of stored energy could occur. There were no machine-specific procedures established for the press that the victim was working on.
The company has been in business for 15 years, specializing in steering linkage for heavy equipment. The company had 3 employees, one office worker and the co-owners who both worked in the shop to form the product line. The victim worked full time, approximately 8-hour days. He had at least 44 years of experience operating a press. The victim had worked 7 years at this site. The company had a written health and safety program, including lockout/tagout. The victim had worked at various companies during his work history and had a great deal of experience in setting up dies and operating many different types of presses, including full revolution presses. At a previous place of employment, he had received over 2000 hours of press operation time and had been classified as a full revolution press operator. Press inspections had been performed and documented.
INVESTIGATION
The rubber boot cutting operation was a new operation for the company; the company had previously outsourced this task to an out-of-state firm. Approximately nine months prior to the incident, the out-of-state firm was no longer able to perform the work. The company owners bought back the dies from the out-of-state company and determined that they would perform the rubber boot trim operation instead of identifying another company to outsource the task. The company did not purchase the press in which that the dies were originally installed.
The company did not have any manuals for the “bender” press. The “bender” did not have a serial number or other identifying information. The company co-owner estimated that the press was manufactured sometime between 1940 and 1950, and was an approximately 8-ton press. The “bender” was normally used to bend metal, specifically press drag links. The “bender” was a full revolution press. It consisted of a moving slide (ram) guided in a definite path by the press frame and a stationary bed. The lower die was attached to the press’s base plate, the plate attached to the top of the stationary bed having drilled holes to T-slots; the upper die attached to the ram. The “bender” did not have an interlocked press barrier guard attached to the press frame or bolster. There was a metal mesh guard at the rear of the press. (See Figure 1) The press did have a barrier guard when used as a “bender”; the barrier guard was impractical for the boot cutting operation and was not installed on the press for this job.
The rubber boot, which protects the steering bearings from dirt and other contaminants, was loaded manually by hand into the press. To activate the clutch, two palm buttons must be depressed simultaneously. When the clutch is tripped and the flywheel engaged it cannot be disengaged until the crankshaft completes its full revolution. An emergency stop button cannot stop the downward and upward strokes of the ram once the crankshaft is engaged; the ram will complete the entire revolution and return to the start (up) position.
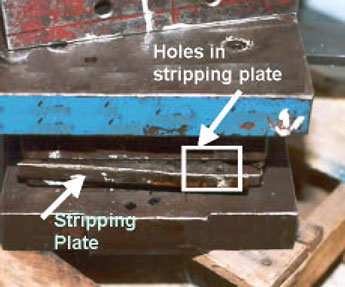
The victim installed the upper and lower dies on the “bender” press to trim the rubber boot. Figure 2 shows the die set used in the rubber boot trim operation. Attached to the bottom die was the stripping plate. The stripping plate was attached by four springs to the bottom die. When the press is activated and the upper ram moves downward and comes into contact with the stripping plate, the stripping plate goes down with the ram, but doesn’t touch the bottom die. In this way, excess boot material can be stripped without damaging the product and
Figure 2. Die set for rubber boot
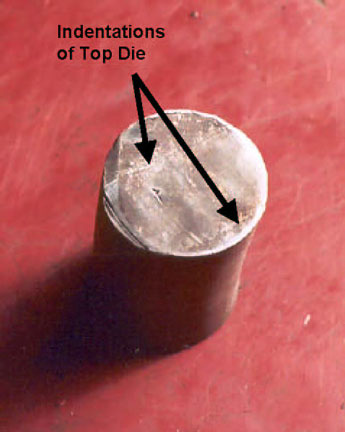
The first run produced defective parts; the rubber was not completely trimmed from the boot and needed further hand trimming. To correct this problem, the victim had taken the dies out of the press and sharpened them. The fatal incident occurred when he restarted the press after he installed the sharpened dies. It appears the victim had placed a cylindrical piece of solid steel 17/8” in diameter and 4” long on the top edge of the stripping plate, nearest to him (See Figure 3). He was using the steel as both a measurement tool for the die and as a stop block to ensure that the top ram would not go down too far (bottom out) on the lower die pins.
A stool was located in front of the press. The victim activated the press with the piece of steel on the stripping plate. It is unknown if the victim was seated on a stool in front of the press when the incident occurred; if seated on the stool facing the press, he had a good view of the ram movement. He may have noticed the steel on the stripping plate and tried to remove it (there were cuts on his right hand). Under normal operation, when the ram comes down, the stripping plate will depress evenly. At the time of the incident, when the ram came down and contacted the piece of steel on the front side of the stripping plate causing the stripping plate to depress unevenly - the front side was lower than the back side of the stripping plate. Figure 3 and Figure 4 show the force of the dies on the stop block. Figure 3 shows the mark on the chunk of steel where it was contacted by the upper die. Figure 4 shows the pinch mark where the steel was placed on the edge of the stripping plate and indentations on the steel that matched the holes on the stripping plate.
 |
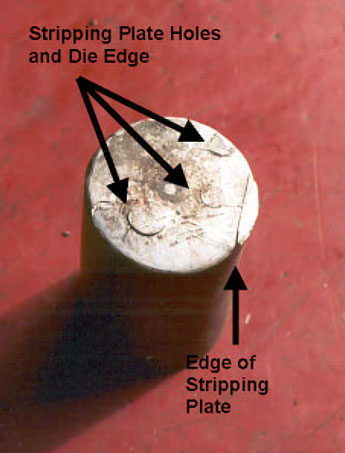 |
| Figure 3. Indentations from top die on steel used by victim | Figure 4. Indentations from stripping plate on steel used by victim |
Because of the location of the piece of steel on the stripping plate and the downward force of the ram, the chunk of steel was propelled from its position on the stripping plate at a high velocity away from the press, toward the victim. Figure 5 shows the deformation of the cylindrical piece of steel caused by the force of the press. The piece of steel struck him in the chest. The co-owner was working approximately 20 feet away. He heard two bangs; heard the victim yell and looked over to see the victim on the ground. The co-owner provided CPR while the office worker called 911. Emergency response arrived and transported the victim to the hospital, where he died of his injuries.
Figure 5. Side view of cylindrical steel piece used by victim as stop block |
CAUSE OF DEATH
The cause of death as stated on the death certificate was blunt force injuries of the chest. The results of all toxicological tests were negative.
RECOMMENDATIONS/DISCUSSION
 |
 |
| Figure 6. Company-designed safety block | Figure 7. Barrier Guard |
| Tm=1/2 | + | Number of engaging points per revolution |
x | time necessary to complete 1 revolution of the crankshaft (seconds) |
REFERENCES
MIOSHA Standards cited in this report can be directly accessed from the Consumer and Industry Services, MIOSHA website http://www.michigan.gov/dleg/0,1607,7-154-11407_15368---,00.html. (Link updated 12/11/2007)
The Standards can also be obtained for a fee by writing to the following address: Department of Consumer and Industry Services, MIOSHA Standards Division, P.O. Box 30643, Lansing, MI 48909-8143. MIOSHA phone number is (517) 322-1845.
MIFACE (Michigan Fatality and Control Evaluation), Michigan State University (MSU) Occupational & Environmental Medicine, 117 West Fee Hall, East Lansing, Michigan 48824-1315. This information is for educational purposes only. This MIFACE report becomes public property upon publication and may be printed verbatim with credit to MSU. Reprinting cannot be used to endorse or advertise a commercial product or company. All rights reserved. MSU is an affirmative-action, equal opportunity employer. 11/14/03
To contact Michigan State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.
| To improve the quality of the MIFACE program and our investigation reports, we would like to ask you a few questions regarding this report. | |||
| Please rate the following on a scale of: | |||
| Excellent | Good | Fair | Poor |
| 1 | 2 | 3 | 4 |
| What was your general impression of this MIFACE investigation report? | |||
| Excellent | Good | Fair | Poor |
| 1 | 2 | 3 | 4 |
| Was the report… | Excellent | Good | Fair | Poor |
| Objective? | 1 | 2 | 3 | 4 |
| Clearly written? | 1 | 2 | 3 | 4 |
| Useful? | 1 | 2 | 3 | 4 |
| Were the recommendations … | Excellent | Good | Fair | Poor |
| Clearly written? | 1 | 2 | 3 | 4 |
| Practical? | 1 | 2 | 3 | 4 |
| Useful? | 1 | 2 | 3 | 4 |
| How will you use this report? (Check all that apply) | |
| O | Distribute to employees |
| O | Post on bulletin board |
| O | Use in employee training |
| O | File for future reference |
| O | Will not use it |
| O | Other (specify) __________________________________________ |
Thank You!
Please Return To:
MIFACE
Michigan State University
117 West Fee Hall
East Lansing, MI 48824
FAX: 517-432-3606
Comments:
| If you would like to receive e-mail notifications of future MIFACE work-related fatality investigation report summaries, please complete the information below. | |
| Name: __________________________________________ | |
| e-mail address: ___________________________________ | |
| I would like to receive summaries for reports involving: | |
| ___ Construction | ___ Agriculture |
| ___ Manufacturing | ___ All |

![]()