
Investigation: # 01MI038
Maintenance Worker Struck in Head by Exploding Pressurized Tank
SUMMARY
|
RECOMMENDATIONS
INTRODUCTION
On June 21, 2001, a 39-year old male died when a storage tank holding a mixture of waste oil and water ruptured. The individual was draining the storage tank using pressurized air from a compressed airline. While under pressure, the tank ruptured and some part of the tank struck him in the head as it lifted off its base. On June 21, 2001, MIFACE investigators were informed by the Michigan Occupational Safety and Health Act (MIOSHA) 24-hour fatality report system that a work-related fatal injury had occurred that day. The notification stated that a tank had exploded killing one worker. Initial reports of the incident indicated it had been caused by a gas leak. Neighboring businesses were evacuated. The company Safety and Health Director was interviewed at the plant by the MIFACE researcher on August 22, 2001. The site of the fatality was not seen, nor was the storage tank. It has been placed in a locked area. Pictures of the site and the tank were viewed. The medical examiner’s report, the police report, statements of witnesses at the plant, and a copy of the citation issued to the employer were obtained during the course of the investigation.
The event resulted in MIOSHA issuing one serious citation under the General Duty Clause for failing to establish, train on and enforce use of a procedure to empty waste oil containers which would prohibit application of air pressure to a container not designed or rated as a pressure vessel.
INVESTIGATION
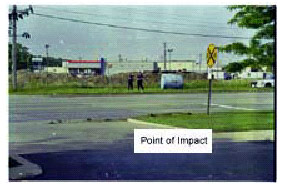 |
Shortly after the noise occurred, personnel from the city police department, fire department, fire/rescue squad, and the state Fire Marshall arrived at the plant believing there had been an explosion caused by a gas leak. Neighboring businesses were evacuated. The noise was actually a result of the storage tank under pressure erupting from its base. The tank was projected approximately 500 feet through the air over the plant fence and over a bank parking lot into the road by the force of the compressed air with which it was being filled. The base of the tank slid across the plant property. The plant fence stopped the base’s movement.
The worker who had been injecting the compressed air into the tank was killed. His head was struck by some part of the tank as it ruptured at its base. The coroner’s report indicates the cause of death was cranial cerebral injuries. Brain death occurred on impact. The 40-year old victim had worked for the company for 16 years. He had worked at this plant for two years and had been doing this job since he arrived there. His job classification was building maintenance. He was working ten-hour days plus overtime when the incident occurred.
The plastic injection molding company supplies trim parts to the auto industry. The company has been in business for 27 years. It has owned this plant for 14 years. The company has 31 plants in the U.S. with a workforce of approximately 9,500. Twenty of its plants are in Michigan. Worldwide the company employs 17,000.
Approximately 200 employees were on site on the day the fatality occurred. The plant was evacuated when the noise occurred, because of the belief that it was caused by a gas explosion.
On the day of the incident, the victim was vacuuming liquid from shallow trenches below injection molding machines into a 500-gallon liquid storage tank, so that pipes in the trenches needing replacement could be accessed. This was a common practice. The waste liquid consisted basically of water with a small amount of tramp oil. The waste liquid storage tank was filled to approximately three-quarters full. The tank was transported by a lift truck to an underground waste liquid holding tank located just outside the south side of plant building. The waste liquid was to have been gravity-drained into the underground holding tank.
A quarter-inch ball valve was located on top of the tank for venting. Just below this vent on the side of the tank was a two-inch diameter pipe where the sump pump drain line was attached. This upper two-inch fitting used during filling had various piping adapters and reducing fittings with a quick disconnect. Another valve assembly with a two-inch ball valve attachment was located on the bottom of the tank directly below the upper attachment. The operator would connect a 1½ inch diameter 8-foot rubber hose to the lower attachment to drain the tank. Between the upper and lower fittings was a one-half inch diameter plastic tube used as a sight glass to determine the height of the waste liquid in the tank.
In order to hasten the evacuation of the tank, a compressed air hose from just inside the plant with a quick disconnect was attached to the tank at the upper pipe assembly. Compressed air at 120 psi was released into the tank. A coworker indicated that the air pressure had recently been increased from 100 psi to 120 psi, and that the victim may have been unaware of the increase.
 |
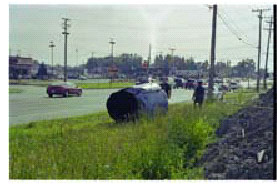
| Tank base against plant fence |
The liquid storage tank was not approved for use as a pressurized container. It had originally been used for oil storage, but developed a leak and was painted with "DO NOT USE". The base of the tank had been welded onto a metal device that allowed it to be transported by the forks of the lift truck. These welds did not separate. The top of the tank tore away from its base leaving the base welded to the transport device. Evidence of rust was visible around the base of the tank. The rust apparently weakened the steel enough for the pressure to cause the rupture at the bottom of the tank above the base.
 |
The company had a written health and safety program although there were no written procedures for this job. The company received assistance with health and safety issues from its worker’s compensation carrier and its insurance carrier. The employees received training from the Health and Safety Director. The Director acquired his health and safety knowledge through seminars and OSHA training courses. There is no health and safety committee at the company. Employees received up to 40 hours of training annually on a quarterly and as-needed basis by classroom lecture and videos. Testing and demonstration measured the effects of training. Training records were kept.
CAUSE OF DEATH
The medical examiner recorded the cause of death as cranial cerebral injuries sustained in an explosion. No alcohol or drugs of abuse were detected in the victim’s blood and urine. Carbon monoxide was less than 5% of total hemoglobin.
RECOMMENDATIONS
• Conduct job safety analyses and establish standard operating procedures for routine maintenance tasks and train the maintenance personnel in these procedures.
A job hazard analysis is a procedure used to review each job, identify potential hazards, and design actions and procedures to eliminate or control the hazards. Input from workers who usually perform the tasks is important. Of primary importance is the recognition that hazards exist. Even though maintenance work is complex and constantly changing, there are routine tasks. The transferring of waste oil and water was a routine task. A job hazard analysis may have identified the potential for employee injury pressurizing a tank that was not approved as a pressurized vessel. The OSHA Job Hazard Analysis publication may be found and downloaded from the OSHA website: http://www.osha.gov/Publications/osha3071.pdf.
• Do not pressurize a container not approved as a pressure vessel.
This fatality involved the improper use of equipment. The task was commonly conducted, yet no one associated with the practice was aware of the consequences of pressurizing a vessel not approved for use under pressure. MIOSHA has regulations regarding the use and inspection of pressure vessels. ASME, the Compressed Gas Association, and the American Petroleum Institute among others have standards and guidelines governing the use of pressure vessels. The Reference Section lists some of these applicable regulations, standards and guidelines.
• Train maintenance personnel to anticipate conditions that could jeopardize their safety or the safety of others.
A Maintenance Supervisor indicated he did not know pressurizing the tank was a dangerous practice or that anything could go wrong. Working with pressurized equipment requires a level of care and engineering knowledge which was not available in the Maintenance Department. Maintenance workers need safety training beyond that of other plant personnel, because they are continually presented with a complex and constantly changing set of activities. Maintenance workers travel throughout the entire plant in the course of their work. Properly trained, they can provide information that is beneficial to the other plant activities while conducting their work.
• Inform employees that no equipment is to be altered or retrofitted. Establish a procedure for a qualified person(s) to review proposed equipment changes. Conduct periodic plant audits specifically for non-standard use of equipment.
When equipment is retrofitted, altered or used in a way for which it was not designed or for a purpose other than originally intended, unintentional consequences may result. A procedure for a qualified person(s) to review equipment change, modification or use should be developed and implemented. Since there is always pressure to “make do” with what is at hand or adapt what is available, periodic plant audits to detect unapproved equipment change or modification should be conducted.
REFERENCES
MIFACE (Michigan Fatality and Control Evaluation), Michigan State University (MSU) Occupational & Environmental Medicine, 117 West Fee Hall, East Lansing, Michigan 48824-1315. This information is for educational purposes only. This MIFACE report becomes public property upon publication and may be printed verbatim with credit to MSU. The author of this report is working under contract to MSU and is affiliated with Wayne State University. Reprinting cannot be used to endorse or advertise a commercial product or company. All rights reserved. MSU is an affirmative-action, equal opportunity employer.
To contact Michigan State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.

![]()