Fatality Assessment and Control Evaluation (FACE) Program |
|
City Equipment Operator Killed when Run Over by a Rotary Riding Mower |
| |||||||||||
SummaryOn August 20, 2003, a 54-year-old public sector equipment operator (the victim) was fatally injured when he was run over by a sit-down rough rotary mower. The victim, who was mowing a section of a city park, stopped the mower on an edge of a hill and turned off the engine. After exiting the mower, he noticed that it had started to roll down the hill. The victim attempted to stop the rolling mower by stepping in front of it, but became trapped underneath the mower and was dragged approximately 75 feet. The victim was ejected from underneath the mower and the mower continued to roll another 25 feet. Two co-workers who were working nearby witnessed the incident and went to assist the victim. A call was placed for Emergency Medical Services (EMS). EMS responded to the incident site within minutes and transported the victim to a local hospital where he was pronounced dead. The Massachusetts FACE Program concluded that to prevent similar occurrences in the future, employers should:
In addition, employers of state and municipal workers should:
IntroductionOn August 26, 2003, the Massachusetts FACE Program was notified by the city clerk's office through the 24-hour Occupational Fatality Hotline, that on August 20, 2003, a 54-year-old male was fatally injured when he was run over by a lawn mower. An investigation was initiated. On October 2, 2003, the Massachusetts FACE Program Director traveled to the city parks department office and the incident location where the department’s deputy commissioner was interviewed. The death certificate, mower information, and police incident report were reviewed. Photographs of the machine involved in the incident and the incident location were taken during the course of the site visit. The employer, a city parks department, employed approximately 60 people. The incident location was a 480 acre city-owned park that had been in existence for more than 100 years. At the time of the incident, the victim and 16 other employees held the job title of laborer/motor equipment operator. The victim had worked for the city parks department for approximately eight years. The employer did not have a designated person in charge of safety and health and did not have a written safety and health program. Training provided by the city on the mower involved in the incident was on-the-job. The dealership from which the city purchased the mower had provided limited training to employees on the mower upon delivery. The victim did have a current Massachusetts Commercial Drivers' License (CDL) and a Hoisting Machinery Operator License, issued through the Massachusetts Department of Public Safety, although these licenses are not required to operate the equipment involved in the incident. The victim was a member of a public sector union. Back to TopInvestigationThe vehicle involved in the incident was a rough rotary mower that was approximately three years old (Figure 1). It was a sit down style mower with a four cylinder 87 horsepower diesel engine. The mower was equipped with four-wheel drive and 29 inch diameter front tires and 24 inch diameter rear tires. The maximum forward mowing speed was 8.5 miles per hour and the maximum forward transport speed was 20 miles per hour. The mower’s braking system consisted of drum brakes and a hand lever parking brake. The mower contained three cutting decks: a 92 inch front deck with five 21 inch blades and two 59 inch wing (side) decks each with three 21-inch blades. Each cutting deck could be placed in a folded up position so the mower would be able to fit into smaller spaces. The over all cutting width of the mower was 192 inches (16 feet). The mower weighed 6,350 pounds and was 16 ½ feet wide and 14 ½ feet long. The victim's normal working hours were 7:00 a.m. - 3:30 p.m. On the day of the incident, the victim's task was to mow grass inside the city owned park. The deputy commissioner had reported that the ground conditions were wet/damp on this day. Mowing the grass at the park was an ongoing task, because once the entire park had been mowed, the sections that had been mowed first would have to be mowed again. The victim was specifically assigned to the mower involved in the incident and had been using the mower for the past few years. Two other employees had been working with the victim prior to the incident. One was using a different style mower and the other was weed trimming locations where the mowers could not fit. At approximately 1:30 p.m. on the day the incident occurred, the victim had stopped the mower on the top edge of a hill (Figure 2) with the cutting decks in the folded up positions. The victim stopped the mower, turned off the engine and exited the operator's area. Within a few seconds of the victim exiting the operator's area, the mower started to roll in a forward direction down the hill. The victim noticed the unattended mower rolling down the hill and attempted to stop it by stepping in front of the mower and pushing against it in the direction opposite in which it was rolling. The mower rolled on top of the victim and he then became trapped underneath it. The mower continued to roll down the hill for approximately 75 feet with the victim trapped underneath it. The victim was then ejected from underneath the mower and the mower continued rolling down the hill for approximately another 25 feet and stopped on level ground. Co-workers who witnessed the incident went to assist the victim and notified Emergency Medical Services (EMS). EMS responded to the incident site within minutes and started to administer first aid. The victim was then transported a local hospital where he was pronounced dead. Back to TopCause of DeathThe medical examiner listed the cause of death as multiple traumatic injuries. Recommendations/DiscussionRecommendation #1: Employers should develop, implement, and enforce standard operating procedures (SOPs) for operating and shutting down mowers, including requirements to park mowers on level ground with the cutting decks lowered to the ground.Discussion: The safest location to stop and park a mower is on level ground. In this case, the victim stopped the mower at the edge of a hill, turned the mower to the off position and exited the mower with the cutting decks in the up position. While unattended, the mower started to roll in the forward direction down the hill. Following SOPs when shutting down mowers will ensure that mowers are stable and will help prevent mowers from moving unexpectedly. When developing standard operating procedures (SOPs) for mowers, employers should refer to the manufacturer’s user/operator manual for mower specific operating features. Some general procedures for parking and shutting down mowers include, but are not limited to:
Once the SOPs have been developed, the employer should provide employees with training on the SOPs and adequate supervision, including unscheduled routine inspections of employee work practices. Although the safest location to stop and park a mower is on level ground, in situations where mowers must be stopped on a slope, the mower should be position sideways across the slope. Then the operator should follow the above procedures with one additional requirement: blocking the mower's wheels.
| ||||||||||||
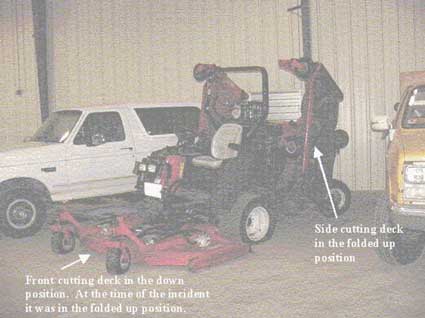 |
| Figure 1 –
Mower involved in the incident |
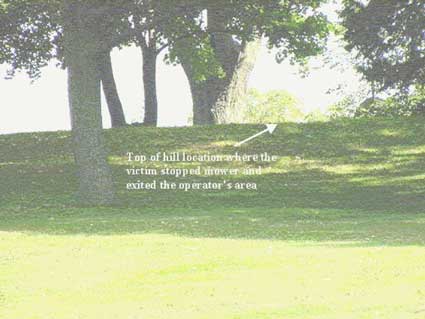 |
Figure
2 – Incident site |
Core elements
Basic obligations
Employee participation
Identify and assess hazards to which employees are exposed
Investigate safety and health events in the workplace
Safety and health program record keeping
Hazard prevention and control
Information and training
Program evaluation and maintenance
Multi-employer workplaces
To contact Massachusetts State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.