|
|||
|
|
Fatality Assessment and Control Evaluation (FACE) Program |
|
Hispanic Youth Dies in Densifier at a Plastics Recycling Plant - Tennessee |
| ||||||||||||||
SummaryOn March 9, 2005, a fourteen-year-old male Hispanic laborer (the victim) died from injuries sustained after coming in contact with the blade inside a Densifier. A Densifier is a machine used to shred and grind plastic bags into a recyclable product. During the night shift, while the seven other crew members, all Hispanic, were out of the immediate vicinity of the Densifier, the victim entered the machine. When the coworkers returned to the area, they were unable to locate the victim on the plant floor. A coworker looked into the machine and saw the victim inside. He called 911 and then called the plant manager at his home. Emergency Medical Service (EMS) personnel responded to the scene within 7 minutes. When the plant manager arrived, he turned off and locked out the external power source to the Densifier. EMS personnel, who entered the machine through a side access hatch by removing the fixed bolts, removed the remains of the victim. A coroner in attendance pronounced the victim dead at the scene.
NIOSH investigators concluded that, to help prevent similar occurrences, employers should:
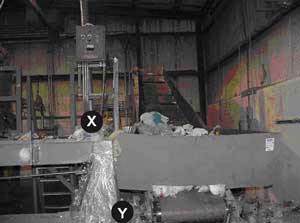
IntroductionOn March 9, 2005, a fourteen-year-old male Hispanic laborer (the victim) died from injuries sustained after coming in contact with the blade inside a Densifier (Photo 1). On March 16, 2005, the U.S. Department of Labor, Wage and Hour Division, notified the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR) of the incident. On March 23-24, 2005, a DSR Safety and Occupational Health investigative team met with a compliance officer and an Assistant Director of the U.S. Department of Labor, Wage and Hour Division, Southeast Region; and with a compliance officer of the Tennessee Department of Labor and Workforce Development (TDLWD), Division of Occupational Safety and Health. Findings from the compliance officers’ investigations were reviewed, along with the police report of the incident and the assistant coroner’s report. On March 23, 2005, the DSR team made a site visit to the plant and discussed the incident with the plant manager and the employer’s workers’ compensation specialist. None of the coworkers who were working during the incident were available for interview. The DSR team was allowed to view the incident scene at a distance, but was not permitted to take measurements or photograph the area. Photographs and measurements taken by TDLWD were used in this report.
The employer began operations at the plastics recycling plant on December 2, 2003. The company employed 31 people at the time of the incident. Twenty-nine were Hispanic and spoke primarily Spanish. Two employees, the plant manager and the mechanic, spoke only English. No one working at the plant at the time of the investigation was bilingual. According to the plant manager, the company had employed an office worker who was bilingual, but she left the company two weeks before the incident. According to the TDLWD compliance officer, the company’s general safety program was deficient in several areas. There was no permit-required confined space safety program, and the hazardous energy program (lockout/tagout) in place at the time of the incident was not machine specific for this facility. The bilingual office worker had conducted the company safety training. This training involved translating the safety pamphlets on general lockout/tagout procedures, work place safety, and forklift operations. The instructor had reportedly not received any formal training in these areas herself. There was no documentation of training. The victim, who was hired five days prior to the incident, received no training. He presented a social security card and an alien registration card attesting that he was 19 years old. Following the incident it was discovered, through the police investigation of the incident, that the victim’s reported social security card number corresponded to the number from an individual who died in 1987, and the victim’s alien registration card was attributed to an individual from Honduras. The victim’s correct age was 14. This was confirmed by his birth certificate obtained after his death from a family member. This was the employer’s first workplace fatality. Back to TopInvestigationThe incident took place at a plastics recycling plant that produced 50 million pounds of high density polyethylene annually. The main process at the plant consisted of converting discarded plastic bags into plastic pellets, which were then sold to various industries. The conversion occurred when the plastic bags were introduced into the Densifier via a conveyor belt powered by a 1 horsepower motor. The conveyor belt was approximately 24 inches wide with an angled metal guard on either side to prevent the plastic bags from falling off the belt. When the plastic bags reached the end of the conveyor belt, they fell through the top opening of the Densifier. The combination of the sheering action of the blade and the heat produced from the motion converted the plastic bags into pellets that were discharged through a side chute. The pellets were moved through pneumatic conveyors to a collection point where they were bagged and stored on pallets.
The Densifier was reportedly manufactured 30 years ago. The employer did not have an operator’s manual for the machine. It consisted of a large steel drum with an 18 by 26 inch opening in the top of the Densifier. The Densifier body was approximately 5 feet in height and approximately 3.5 feet in diameter. The distance from the top of the Densifier opening to the plant floor was approximately 8.5 feet. A 3 foot diameter direct drive rotor blade which traveled at 1750 rotations per minute revolved at the base inside the Densifier and was powered by a 250 horsepower motor. There was a hinged hood over the top opening that could be retracted to gain access to the interior of the Densifier from above. The hood was not used as a guarding method for the opening. It was used to keep the plastic bags from being thrown upward during plastic bag shredding operations. According to the TDLWD compliance officer, the conveyor belt was wide enough for a single worker to walk on to reach the top of the Densifier. The controls for the conveyor belt and Densifier’s spinning internal rotor blade were located to the side of the machine and were accessed by an operator who stood on an elevated platform. The platform was approximately 56 inches wide at the front of the platform and 4.5 feet above the plant floor. There were no standard guardrails at the front of the platform (Photo 2). The control panel for the Densifier consisted of push start/stop buttons and an emergency shutoff button for the blade. There was an on/off switch mounted on a pole near the operator station which controlled power to the conveyor belt. A sign was observed on the Densifier’s control panel that read in English, “Only Authorized Personnel Can Operate this Machine.” There was no Spanish translation provided. Power to the Densifier ran through a fuse box mounted on the wall adjacent to the machine (Photo 3). The machine was designed to be operated by two people. One worker (the loader) stood at the base of the conveyor belt and threw the plastic bags over a guard onto the conveyor belt. The role of the second person (the operator) was to turn the conveyor belt on and off, to push the start and stop buttons that control movement of the blade, and to ensure smooth flow of raw materials into the Densifier. The victim was employed as a loader.
There was a side access hatch leading to the interior of the Densifier that was covered and secured with bolts (Photo 4). There were no signs or placards observed on the Densifier warning that it was a permit-required confined space and that special operating procedures were required for authorized entrance. According to the company’s mechanic, this side opening was designed as a sole entrance into the Densifier for its maintenance, but it was frequently entered from the top when the rotor blade jammed. According to the TDLWD compliance officer, there was a 4 riser stairway at the rear of the Densifier leading to this hatch. Standard railings were not installed on the stairway.
The incident was unwitnessed. It occurred at approximately 4:45 a.m. on March 9, 2005, when the plant was being operated by a workforce of eight Hispanic workers. The Spanish speaking police officer who investigated the scene on the morning of the incident was reportedly told by the Hispanic coworkers that they had not seen or heard anything. One coworker said he saw the victim’s body at the bottom of the Densifier and called 911. No one remembered turning the controls for the Densifier and the conveyor belt off, but they were off when EMS personnel arrived. All of these coworkers failed to report to work after the incident and were not available for interview by DSR investigators. Interviews with other plant workers familiar with the procedures and operation of the machine in question, as well as the physical parameters of the incident site, prompted investigators to postulate that the victim, for unknown reasons, was operating the machine alone, loading plastic bags onto the belt with both the conveyor belt and the Densifier running. At some point, it is presumed that the rotor blade inside the Densifier jammed. Several workers familiar with the process reported that this occurred frequently when the rotor blade became dull and no longer cut the plastic bags efficiently. The plastic bags would melt and congeal around the rotor blade. When there was a sufficient amount of plastic accumulated around the blade, it would jam. The victim presumably went to the controls and shut off the conveyor belt and the Densifier rotor blade from the operator’s platform, but he failed to shut down and lockout the power to the machine at its source (Photo 3). From the location of the operator’s platform, which was located about four feet from the top opening to the Densifier, it was unlikely that the victim could have stepped over to the Densifier’s top opening. He presumably walked up the conveyor belt and entered the Densifier from above, most likely with the intent to unjam the blade at its base. It is also possible that the victim fell into the Densifier, but given that there was a history of routine entry into the machine from the top to clear jams, this was determined by investigators to be less likely. While inside the Densifier and bent over, the victim would not have been visible to anyone in the plant. It is presumed that a second worker, unaware of the victim being inside the Densifier and noticing that the machine was not running, went to the controls and started the Densifier. The victim may have made a sound prompting a coworker to stop the machine or coworkers may have noted that the victim was not at his post and began looking for him. A coworker looked in the Densifier and saw the victim’s body. He called 911 and then called the plant manager at his home. Emergency Medical Service (EMS) personnel responded to the scene within 7 minutes. When the plant manager arrived, he turned off and locked out the external power source to the Densifier. EMS personnel entered the Densifier through the side access hatch after removing the fixed bolts which secured the hatch. They recovered the remains of the victim. A coroner in attendance pronounced the victim dead at the scene. Back to TopCause of DeathThe assistant coroner’s report listed the cause of death as partial decapitation of the head with multiple open/crushing injuries. Recommendations/DiscussionRecommendation #1: Employers should establish a lockout/tagout program that, at a minimum, meets requirements established by the Occupational Safety and Health Administration (OSHA).Discussion: All sources of hazardous energy should be locked out before any repairs, blade replacement, or procedures to remove jams are begun. Regulations regarding the control of hazardous energy (lockout/tagout) must be followed and are covered under OSHA standards. OSHA standards for General Industry have specific requirements for lockout/tagout procedures for control of hazardous energy located in subpart J.1 29 CFR 1910.147(a)(1)(i) states that “This standard covers the servicing and maintenance of machines and equipment in which the unexpected energization or start up of the machine or equipment, or release of stored energy could cause injury to employees.” 29 CFR 1910.147(a)(2)(ii) states that “Normal production operations are not covered by this standard. Servicing and/or maintenance which takes place during normal production operations is covered by this standard only if [A] An employee is required to remove or bypass a guard or other safety device; or [B] An employee is required to place any part of his or her body into an area on a machine or piece of equipment where work is actually performed upon the material being processed (point of operation) or where an associated danger zone exists during a machine operating cycle.” Specific recommendations are outlined in the NIOSH Alert titled Preventing Worker Deaths from Uncontrolled Release of Electrical, Mechanical, and other types of Hazardous Energy. Salient points that need to be covered should be machine specific and include the following:
Only trained and qualified personnel should perform repair work or work that entails removing jams from machinery. The company should identify personnel who are qualified and trained to conduct this work and document their hazardous energy related training.
| |||||||||||||||
 |
Discussion: Engineering controls are the cornerstone of any safety program. These controls include construction of physical barriers to isolate a hazard, installation of guardrails to mitigate against a fall hazard, and construction of access routes free of obstructions and hazards for safe operation in and around the plant while providing safe accessibility to the work area. This is in keeping with OSHA’s General Duty Clause which requires employers to furnish a place of employment which is free of recognized hazards that are causing or likely to cause death or serious physical harm to employees.14 Areas to consider retrofitting include placing a guard over the opening at the top of the Densifier to prohibit an employee from entering the Densifier from above. Also, consideration should be given to installing guardrails for fall protection around the operator platform and installing standard railings along the stairway leading to the Densifier’s side access hatch.
Discussion: Given the victim’s authentic-appearing social security and alien residence cards, both of which were forged, it may have been very difficult for the employer to ascertain the victim’s correct age. However, employers should make every effort to ensure they are aware of a worker’s true age and that 14-and 15-year old workers are not assigned to perform prohibited work. Employers who have a multi-lingual/multi-cultural work force should use interpreters when necessary to inform all employees about age-appropriate work assignments. If employers do not fully understand the types of work prohibited for young workers, they should contact the U.S. Department of Labor (DOL), Employment Standards Administration (ESA), Wage and Hour Division. This Division enforces child labor laws under the Fair Labor Standards Act (FLSA).
Under FLSA standards for 14-and 15-year-olds in nonagricultural employment, employment of 14-and 15-year-olds is limited to certain occupations and under certain conditions that do not interfere with their schooling, health or well-being. For example, employment in any manufacturing occupation [such as the manufacture of plastic pellets in this incident] and operating or tending of any hoisting apparatus or any power-driven machinery [such as the Densifer tended by the victim in this incident] is prohibited. Under FLSA Hours standards, 14-and 15-year-olds are prohibited from working before 7 a.m. or after 7 p.m. This incident occurred at 4:45 a.m., during a time expressly prohibited for employment of 14-and 15-year-olds. Information regarding FLSA can be obtained by visiting the DOL ESA web site at http://www.dol.gov/esa/. FLSA employment standards for nonagricultural occupations are listed and explained in Child Labor Bulletin 10115 and summarized in DOL Fact Sheet No. 43.16 Child labor information can also be obtained by calling or visiting offices of Federal and State child labor departments, located by using the telephone directory government pages.
Employers should meet with their workforce to communicate the company’s policies regarding appropriate work assignments for young workers. They should explain that young workers are at an increased risk for injury at work and reinforce the importance of assigning youths to appropriate work tasks. They should provide all staff with a description of youth work assignments, identify the person(s) responsible for supervision of young workers, inform all staff about assigned supervisors, and direct staff to notify supervisors immediately if they see young workers performing hazardous work or working outside their assigned tasks.
This investigation was conducted by Joseph F. Chesky MD, MPH, Occupational
Medicine Resident at West Virginia University School of Medicine assigned
to NIOSH, Division of Safety Research, Special Studies Team and Doloris
N. Higgins, Safety and Occupational Health Specialist, Fatality Investigation
Team, Surveillance and Field Investigations Branch, Division of Safety
Research.