No one knows exactly what starts the AD process or why some of the normal changes associated with aging become so much more extreme and destructive in people with the disease. We know a lot, however, about what happens in the brain once AD takes hold and about the physical and mental changes that occur over time. The time from diagnosis to death varies—as little as 3 or 4 years if the person is older than 80 when diagnosed to as long as 10 or more years if the person is younger. Several other factors besides age also affect how long a person will live with AD. These factors include the person’s sex, the presence of other health problems, and the severity of cognitive problems at diagnosis. Although the course of the disease is not the same in every person with AD, symptoms seem to develop over the same general stages.
 Preclinical AD |
PRECLINICAL AD
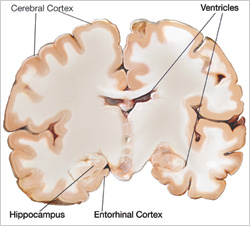
AD begins deep in the brain, in the entorhinal cortex, a brain region that is near the hippocampus and has direct connections to it. Healthy neurons in this region begin to work less efficiently, lose their ability to communicate, and ultimately die. This process gradually spreads to the hippocampus, the brain region that plays a major role in learning and is involved in converting short-term memories to long-term memories. Affected regions begin to atrophy. Ventricles, the fluid-filled spaces inside the brain, begin to enlarge as the process continues.
Scientists believe that these brain changes begin 10 to 20 years before any clinically detectable signs or symptoms of forgetfulness appear. That’s why they are increasingly interested in the very early stages of the disease process. They hope to learn more about what happens in the brain that sets a person on the path to developing AD. By knowing more about the early stages, they also hope to be able to develop drugs or other treatments that will slow or stop the disease process before significant impairment occurs (see "The Search for New Treatments" for more information).
| |
|
PiB and PET |
|
Imagine being able to see deep inside the brain tissue of a living person. If you could do that, you could find out whether the AD process was happening many years before symptoms were evident. This knowledge could have a profound impact on improving early diagnosis, monitoring disease progression, and tracking response to treatment.
Scientists have stepped closer to this possibility with the development of a radiolabeled compound called Pittsburgh Compound B (PiB). PiB binds to beta-amyloid plaques in the brain and it can be imaged using PET scans. Initial studies showed that people with AD take up more PiB in their brains than do cognitively healthy older people. Since then, scientists have found high levels of PiB in some cognitively healthy people, suggesting that the damage from beta-amyloid may already be underway. The next step will be to follow these cognitively healthy people who have high PiB levels to see whether they do, in fact, develop AD over time.
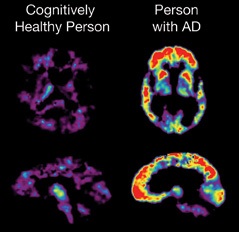
In this PET scan, the red and yellow colors indicate that PiB uptake is higher in the brain of the person with AD than in the cognitively healthy person. | |
VERY EARLY SIGNS AND SYMPTOMS
At some point, the damage occurring in the brain begins to show itself in very early clinical signs and symptoms. Much research is being done to identify these early changes, which may be useful in predicting dementia or AD. An important part of this research effort is the development of increasingly sophisticated neuroimaging techniques (see "Exciting New Developments in AD Diagnosis" for more on neuroimaging) and the use of biomarkers. Biomarkers are indicators, such as changes in sensory abilities, or substances that appear in body fluids, such as blood, cerebrospinal fluid, or urine. Biomarkers can indicate exposure to a substance, the presence of a disease, or the progression over time of a disease. For example, high blood cholesterol is a biomarker for risk of heart disease. Such tools are critical to helping scientists detect and understand the very early signs and symptoms of AD.
Mild Cognitive Impairment
As some people grow older, they develop memory problems greater than those expected for their age. But they do not experience the personality changes or other problems that are characteristic of AD. These people may have a condition called mild cognitive impairment (MCI). MCI has several subtypes. The type most associated with memory loss is called amnestic MCI. People with MCI are a critically important group for research because a much higher percentage of them go on to develop AD than do people without these memory problems. About 8 of every 10 people who fit the definition of amnestic MCI go on to develop AD within 7 years. In contrast, 1 to 3 percent of people older than 65 who have normal cognition will develop AD in any one year.
However, researchers are not yet able to say definitively why some people with amnestic MCI do not progress to AD, nor can they say who will or will not go on to develop AD. This raises pressing questions, such as: In cases when MCI progresses to AD, what was happening in the brain that made that transition possible? Can MCI be prevented or its progress to AD delayed?
Scientists also have found that genetic factors may play a role in MCI, as they do in AD (see "Genetic Factors at Work in AD" for more information). And, they have found that different brain regions appear to be activated during certain mental activities in cognitively healthy people and those with MCI. These changes appear to be related to the early stages of cognitive impairment.
| Charting the Course from Healthy Aging to AD |
|
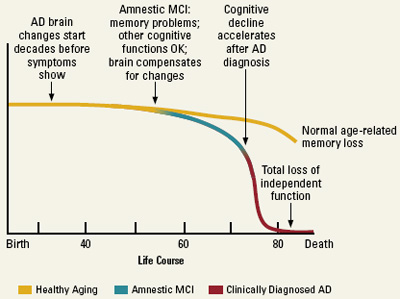
This chart shows current thinking about the evolution from healthy aging to AD. Researchers view it as a series of events that occur in the brain over many years. This gradual process, which results from the combination of biological, genetic, environmental, and lifestyle factors, eventually sets some people on a course to MCI and possibly AD. Other people, whose genetic makeup may be the same or different and who experience a different combination of factors over a lifetime, continue on a course of healthy cognitive aging.
|
Other Signs of Early AD Development
As scientists have sharpened their focus on the early stages of AD, they have begun to see hints of other changes that may signal a developing disease process. For example, in the Religious Orders Study, a large AD research effort that involves older nuns, priests, and religious brothers, investigators have explored whether changes in older adults’ ability to move about and use their bodies might be a sign of early AD. The researchers found that participants with MCI had more movement difficulties than the cognitively healthy participants but less than those with AD. Moreover, those with MCI who had lots of trouble moving their legs and feet were more than twice as likely to develop AD as those with good lower body function.
It is not yet clear why people with MCI might have these motor function problems, but the scientists who conducted the study speculate that they may be a sign that damage to blood vessels in the brain or damage from AD is accumulating in areas of the brain responsible for motor function. If further research shows that some people with MCI do have motor function problems in addition to memory problems, the degree of difficulty, especially with walking, may help identify those at risk of progressing to AD.
Other scientists have focused on changes in sensory abilities as possible indicators of early cognitive problems. For example, in one study they found associations between a decline in the ability to detect odors and cognitive problems or dementia.
These findings are tentative, but they are promising because they suggest that, some day, it may be possible to develop ways to improve early detection of MCI or AD. These tools also will help scientists answer questions about causes and very early development of AD, track changes in brain and cognitive function over time, and ultimately track a person’s response to treatment for AD.
 Mild to Moderate AD |
MILD AD
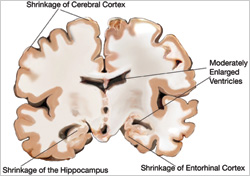
As AD spreads through the brain, the number of plaques and tangles grows, shrinkage progresses, and more and more of the cerebral cortex is affected. Memory loss continues and changes in other cognitive abilities begin to emerge. The clinical diagnosis of AD is usually made during this stage. Signs of mild AD can include:
- Memory loss
- Confusion about the location of familiar places (getting lost begins to occur)
- Taking longer than before to accomplish normal daily tasks
- Trouble handling money and paying bills
- Poor judgment leading to bad decisions
- Loss of spontaneity and sense of initiative
- Mood and personality changes, increased anxiety and/or aggression
In mild AD, a person may seem to be healthy but is actually having more and more trouble making sense of the world around him or her. The realization that something is wrong often comes gradually to the person and his or her family. Accepting these signs as something other than normal and deciding to go for diagnostic tests can be a big hurdle for people and families. Once this hurdle is overcome, many families are relieved to know what is causing the problems. They also can take comfort in the fact that despite a diagnosis of MCI or early AD, a person can still make meaningful contributions to his or her family and to society for a time.
| |
|
AD Spreads Through the Brain |
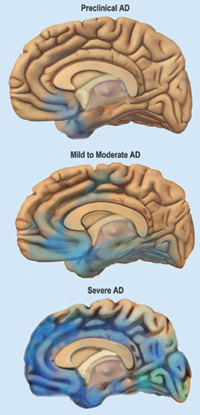 | |
MODERATE AD
By this stage, AD damage has spread to the areas of the cerebral cortex that control language, reasoning, sensory processing, and conscious thought. Affected regions continue to shrink, ventricles enlarge, and signs and symptoms of the disease become more pronounced and widespread. Behavioral problems, such as wandering and agitation, can occur. More intensive supervision and care become necessary, which can be difficult for many spouses and families. The symptoms of this stage can include:
- Increasing memory loss and confusion
- Shortened attention span
- Inappropriate outbursts of anger
- Problems recognizing friends and family members
- Difficulty with language and problems with reading, writing, and working with numbers
- Difficulty organizing thoughts and thinking logically
- Inability to learn new things or to cope with new or unexpected situations
- Restlessness, agitation, anxiety, tearfulness, wandering—especially in the late afternoon or at night
- Repetitive statements or movement, occasional muscle twitches
- Hallucinations, delusions, suspiciousness or paranoia, irritability
- Loss of impulse control (shown through undressing at inappropriate times or places or vulgar language)
- An inability to carry out activities that involve multiple steps in sequence, such as dressing, making a pot of coffee, or setting the table
Behavior is the result of complex brain processes, all of which take place in a fraction of a second in the healthy brain. In AD, many of those processes are disturbed, and these disrupted communications between neurons are the basis for many distressing or inappropriate behaviors. For example, a person may angrily refuse to take a bath or get dressed because he does not understand what his caregiver has asked him to do. If he does understand, he may not remember how to do it. The anger can be a mask for his confusion and anxiety. Or, a person with AD may constantly follow her husband or caregiver and fret when the person is out of sight. To a person who cannot remember the past or anticipate the future, the world can be strange and frightening. Sticking close to a trusted and familiar caregiver may be the only thing that makes sense and provides security.
 Severe AD |
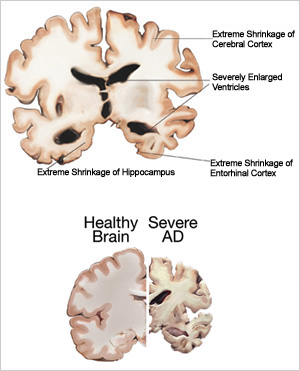
SEVERE AD
In the last stage of AD, plaques and tangles are widespread throughout the brain, most areas of the brain have shrunk further, and ventricles have enlarged even more. People with AD cannot recognize family and loved ones or communicate in any way. They are completely dependent on others for care. Other symptoms can include:
- Weight loss
- Seizures
- Skin infections
- Difficulty swallowing
- Groaning, moaning, or grunting
- Increased sleeping
- Lack of bladder and bowel control
Near the end, the person may be in bed much or all of the time. The most frequent cause of death for people with AD is aspiration pneumonia. This type of pneumonia develops when a person is not able to swallow properly and takes food or liquids into the lungs instead of air.
|
The Buddy Program at Northwestern University |
|
 The medical school curriculum demands that students spend enormous amounts of time in the classroom and clinic learning the information and skills necessary for a career in medicine. However, little or no time is set aside for students to be with patients outside the hospital or clinic setting. As a result, it is hard for medical students to get to know the human side of the diseases they are learning about. The medical school curriculum demands that students spend enormous amounts of time in the classroom and clinic learning the information and skills necessary for a career in medicine. However, little or no time is set aside for students to be with patients outside the hospital or clinic setting. As a result, it is hard for medical students to get to know the human side of the diseases they are learning about.
A program at Northwestern University’s Cognitive Neurology and Alzheimer’s Disease Center is adding just that element to its medical education. The Buddy Program, begun in 1998, matches first-year medical students with people diagnosed with AD or another form of dementia. About 10 to 15 medical students participate every year. They first take a 3-hour orientation course on AD, family issues, and communication skills. Then, for the next year, they spend at least 4 hours a month with a person with dementia in addition to monthly meetings with the program coordinators. Together with the person’s caregiver and the program’s professional staff, students and their “buddies” choose activities for their visits together. Activities can include shopping, visiting museums, exercising together, or even just sharing a coffee or a meal. The students also are able to observe their buddies’ clinical evaluations at the Center. Other medical schools have started similar programs.
The people with AD and their families are selected from Northwestern’s Alzheimer’s Disease Center and other related programs at the university. Families are contacted about participating, and the people with AD are selected based on their ability to understand the nature of the program and their willingness to spend time every month with the student buddy.
The program has clear benefits for both the medical student and the person with AD. For the medical student, it provides a hands-on way to learn about AD and related dementias, and it helps him or her understand the daily realities and issues involved in caring for and supporting people with AD and their families. It also introduces them to the career path of research and clinical practice in AD and related dementias. For the person with AD, participation in the program provides an opportunity for friendship and socializing and an outlet for sharing their experiences with a sympathetic listener.
For many of the students, the program is a transformative experience. They become very close to their buddies and family caregivers during their year together, and continue the friendship even after the year is over.
The Buddy Program pairs medical students with people with AD to spend time with—and learn from—each other. |
<< Back | Next >>
