 |
Virtual Colonoscopy Identifies Large Polyps
|
|
Also in the Journals |
|
| A supplement on "Improving Delivery of Colorectal Cancer Screening in Primary Care Practice" was recently published by the journal Medical Care. The supplement consists of 22 papers from a program of research sponsored by NCI and the Agency for Healthcare Research and Quality (AHRQ) to improve the delivery, utilization, and outcomes of colorectal cancer screening in primary care practice. The supplement presents approaches to delivering colorectal cancer screening in primary care settings and evaluating screening outcomes. This initiative directly addresses efforts to improve colorectal cancer screening uptake in the United States, which remains low - at about 50 percent. |
|
Results from the American College of Radiology Imaging Network (ACRIN) National CT Colonography Trial, published in the September 18 New England Journal of Medicine, show that computed tomography (CT) colonography - also known as virtual colonoscopy - can detect 90 percent of adenomas (noncancerous tumors that can progress to cancer) or colorectal cancers measuring 1 centimeter or more in diameter.
These results compare favorably with standard optical colonoscopy, "which misses roughly 8 to 10 percent" of lesions of this size, says Dr. Carl Jaffe, chief of the NCI Cancer Imaging Program's Diagnostic Imaging Branch.
Both CT colonography and colonoscopy can be employed to screen for precancerous polyps, the removal of which helps prevent the development of colorectal cancer. While colonoscopy uses a thin, tube-like instrument to physically examine the inside of the colon and rectum, CT colonography takes 2- or 3-dimentional pictures of the colon and rectum using a high-powered x-ray machine linked to a computer. The computed tomography technology required for CT colonography is already found in almost all hospitals, explains Dr. Jaffe.
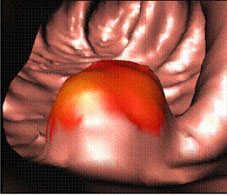
Virtual colonoscopy image of the inside of a colon. The red colored area indicates a polyp. Image courtesy of Dr. Ronald M. Summers, Diagnostic Radiology Department, Clinical Center, National Institutes of Health.
| |
|
"The less invasive nature of CT colonography and the low risk of procedure-related complications, as compared to colonoscopy, may be attractive to patients and may improve screening-adherence rates by addressing certain concerns of both patients and providers," state the authors.
Investigators at 15 hospitals participated in the ACRIN trial and enrolled more than 2,500 participants aged 50 or older who were scheduled for a screening colonoscopy. Participants first underwent CT colonography followed by standard colonoscopy, which was performed on the same day for 99 percent of participants.
The investigators compared results from the CT colonography exam to colonoscopy results for each patient, for the detection of lesions 5 millimeters or more in diameter, and calculated the false negative and false positive rates for CT colonography - the likelihood of missing a lesion (false negative) or falsely identifying a lesion that could not be found on follow-up colonoscopy (false positive).
While CT colonography could correctly identify 90 percent of people who had at least one polyp 10 millimeters in diameter or greater, the ability to correctly identify people who had smaller polyps was lower - down to 65 percent for polyps 5 millimeters in diameter.
|

A still frame of an NIH Clinical Center video, which shows a virtual colonoscopy of the rectosigmoid colon performed in a retrograde fashion. The entire video can be viewed at http://www.cc.nih.gov/drd/colonoscopy.html on the NIH Clinical Center's Web site.
|
|
The significance of these smaller lesions remains under debate. "Traditionally we've said that advanced adenomas are the ones with the most potential for developing into cancer," says Dr. Barry Kramer, associate director for disease prevention at the National Institutes of Health. The risk posed by smaller polyps "is the nub of a debate that's already started and will continue between radiologists and gastroenterologists," he explains.
Some additional questions about CT colonography remain to be answered, explains Dr. Robert Fletcher, professor emeritus from Harvard Medical School, in an accompanying editorial; in particular, whether CT colongraphy may miss some flat or depressed adenomas and what cumulative radiation dose may result from exposure to regular CT scans for screening.
The difficulty with flat and depressed adenomas, says Dr. Kramer, is that "we don't really yet know their natural history. We don't know how important it is to catch every last one," he explains. Both CT colonography and colonoscopy techniques need to be refined to better detect this type of adenoma.
Dr. Jaffe does not think that the radiation exposure, which is less than a standard CT scan, will be a large concern in this population. "For people over 50, the risk becomes diminutive, and if you use newer CT techniques, you can keep the exposure relatively low," he says.
For him, the most exciting thing about CT colonography is the ability to potentially reserve colonoscopy - which is more expensive and invasive, and currently requires specialists who are in short supply in the United States - for patients who have identified polyps, "so that [gastroenterologists] can concentrate on cases that merit polyp removal," he concludes.
—Sharon Reynolds
The current U.S. Preventive Services Task Force guidelines on colorectal cancer screening are available online at http://www.ahrq.gov/clinic/uspstf/uspscolo.htm.
|