Fatality Assessment and Control Evaluation (FACE) Program |
|
A Gas Well Drilling Floorhand Died When He Was Struck by a Hoisted Wellhead Equipment Stack |
| |||||||||||||||||||||||||
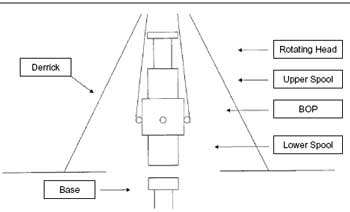
SummaryA 56-year-old gas well drilling floorhand died on May 30, 2005 from chest trauma he received after being struck by a hoisted wellhead stack that overturned. The stack was composed of a lower spool, blowout preventer (BOP), upper spool, and a rotary head. The crew was attempting to replace the lower spool at the time of incident. As the victim and a coworker attempted to pry the lower spool loose, the 18,000-pound, top-heavy equipment overturned, pinning the victim to the ground and striking the coworker. Other crew members immediately freed the victim and called for emergency response. Emergency medical services (EMS) arrived at the scene and transported the victim to the nearest hospital. He was then transported by helicopter to another hospital where he was pronounced dead in the emergency room. Oklahoma Fatality Assessment and Control Evaluation (OKFACE) investigators concluded that to help prevent similar occurrences, employers should:
IntroductionA gas well drilling floorhand died on May 30, 2005 from chest trauma received when he was struck by a hoisted wellhead equipment stack that overturned. OKFACE investigators were notified of the incident and an interview with a company official was conducted on July 7, 2005. OKFACE investigators reviewed the death certificate and reports from the Medical Examiner and the Occupational Safety and Health Administration (OSHA). Employer:The victim was employed by an oil and gas drilling company. The company drilled well sites for oil and gas exploration companies on a contract basis. The company had been in business for five years and employed 85 full-time workers at the time of incident. The company had a written safety and health program, including written task specific and machine specific instructions for all tasks. The company had an active labor/management safety committee and a management safety and health committee. Written contracts existed between the company and subcontractors that established safety responsibilities. Victim:The 56-year-old male victim had been working for the oil and gas drilling company for six months. The victim was performing his usual work tasks in his usual work area at the time of the incident. He had 25 years of experience in oil and gas drilling operations. Training:Site crews conducted weekly safety meetings at all well sites and the company safety officer conducted a safety meeting with all employees every two weeks. Company employees conducted task-specific, machine-specific, and general safety training. Tool pushers (drilling machine operators) and forklift operators were required to complete operator certification training. In addition to hands-on training, equipment manuals, videos, and formal classroom settings were used to train machine operators. Certified machine operators’ proficiency and effects of training were measured through testing and demonstration. All training and safety meetings were documented and kept on file with the company. Incident Scene:The incident occurred on a gas drill site where the company had been operating for 21 days (Figure 1). The incident took place on the ground under the drill floor at a wellhead (Figure 2 and Table 1). The ground in the area was level, but muddy, and oily. Weather: On the day of the incident, the weather conditions were warm and sunny.
Back to TopInvestigationThe incident involved a wellhead located below the drill floor. The wellhead equipment stack weighed approximately 18,000 pounds and was composed of four stacked components including a lower spool, BOP, upper spool, and rotating head (Figure 3). Under normal operations, wellhead components may be replaced or serviced several times throughout a drilling operation. The wellhead was being removed to replace the lower spool to accommodate a change from 7-inch to 4-inch pipe during the drilling operation. The drilling company had nine employees working at the site at the time of the incident, including a tool pusher designated as the supervisor and two drilling crews of four men each.
Employees were wearing hard hats at the time of incident. One of the crews was nearing the end its shift and the second was preparing to start. In addition, a representative (#1) was present from the company holding the property under an oil and gas lease and another representative (#2) from a third company was onsite to deliver the lower spool replacement. Written standard operating procedures and witness statements from employees indicated that the normal procedure for wellhead removal was to disassemble the wellhead starting from the top and remove each component individually, rather than lift the assembled wellhead as one piece. Disassembly of the wellhead usually took two hours. On the day of the incident, the tool pusher was supervising operations, but left the immediate area to get a drink of water and relinquished control of the wellhead removal to representative #2 who was acting as a third party on site. Representative #2 directed the crew to lift the fully assembled wellhead stack as a single unit to save the time and work of disassembling. Representative #2 directed employees to use a two-chain sling attached to two of the four lifting shackles located on the BOP (Figure 4). According to the BOP manufacturer, all four lifting shackles should be used during lifting operations and were designed only to lift the BOP, not other ancillary equipment. The stack was top-heavy during the lifting operation because the lifting sling was attached to the BOP near the bottom of the wellhead assembly.
Witness statements indicated that the wellhead stack had been lifted several times, but the crew had difficulty loosening the lower spool from the BOP. During attempts to remove the lower spool, the lifted wellhead had tipped over without striking anyone. Representative #2 then directed that the twochain sling be rotated 90 degrees to attach to the other two lifting shackles of the BOP than the ones previously used. The points of attachment to the lifting shackles were changed to get more clearance between the wellhead and the bottom of the overhead drill floor. The stack was lifted again while the victim and a coworker used a hammer and crowbar to remove the lower spool. As the lower spool came off the bottom of the BOP, the wellhead tipped over toward the victim and coworker, striking the coworker and pinning the victim to the ground. Coworkers immediately freed the victim and called for emergency response. EMS arrived at the scene within 10 minutes and transported the victim to the nearest hospital. He was transported by helicopter to another hospital where he was pronounced dead a few hours later in the emergency room. The coworker was not hospitalized and suffered primarily bruises, contusions, and abrasions. Cause of DeathThe Medical Examiner’s report listed the cause of death as blunt trauma of the chest. Back to TopRecommendations/DiscussionRecommendation # 1: Employers should ensure that employees do not position themselves under suspended loads.Discussion: The OSHA standards for materials handling and storage that address the use of lifting slings indicate that all employees should be kept clear of loads about to be lifted and of suspended loads. The areas below and adjacent to suspended loads should be controlled access zones. Employees should not occupy controlled access zones while a load is suspended. Employees should use tag lines or other means of remote control to steady and control elevated loads while allowing employees to maintain adequate clearance. Safe working load limits of tag lines should be considered when selecting tag line materials.
| ||||||||||||||||||||||||||