Learning More About Mild Cognitive Impairment
The best-known consequence of AD is memory loss, but this is not the only feature. A person with AD has other problems as well, including difficulties in processing and organizing information; problems with judgments and making decisions; personality changes; hallucinations, delusions, and other psychiatric problems; depression; loss of impulse control; perceptual-motor problems (for example, having trouble getting out of a chair); and physical problems that become pronounced as the disease nears its end.
As some people grow older, they develop memory problems greater than those expected for their age. But they do not experience the personality changes or have the cognitive or other problems that are characteristic of AD. Their condition, then, may not meet all the medically-defined criteria for AD. These people have a condition called mild cognitive impairment (MCI).
People with MCI are a critically important group for research into the causes of AD because a higher percentage of them go on to develop AD compared to older people without these memory problems. It is not known whether all people with MCI
will advance to AD. This puzzle has raised a number of questions for scientists. Is MCI an early stage of AD, or are they entirely separate conditions? Why and when does MCI sometimes, but not always, develop into AD? Do people with MCI who don’t go on to develop AD have some special protective characteristics? Can MCI be prevented or its progress delayed or interrupted?
These questions have created some obvious research objectives:
- Define MCI and the relationship between MCI and AD
- Learn about the underlying causes and courses of MCI
- Understand the pathology of MCI
- Explore strategies that could prevent or delay MCI and AD
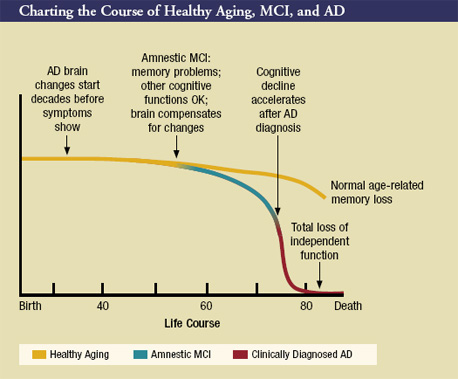
In recent years, investigators have made major progress in achieving these objectives. For example, scientists have developed a framework for understanding the causes and courses of MCI by defining subtypes of the condition based on cause (for example, degenerative, vascular, psychiatric, and medical), and on which aspects of cognition are predominantly affected. The subtype that features memory impairment most prominently is called MCI with memory loss, or "amnestic MCI." This definition of MCI already has been widely used by research teams working on AD treatment strategies in clinical trials. Scientists working in ADCs have reported that about eight in 10 people who meet criteria for amnestic MCI progress to AD within 6 years of diagnosis. The chart on the next page illustrates current thinking about the transition from healthy cognitive aging to amnestic MCI to AD.
Individuals with other MCI subtypes may have prominent deficits in other cognitive functions, such as language skills or visuospatial ability (the ability to recognize objects and determine where they are in relation to each other, and to mentally rearrange them). Other degenerative diseases, such as frontotemporal dementia, dementia with Lewy bodies, and vascular dementia also can cause these symptoms (Petersen, 2005). The development of a clear description of these conditions and the elements and extent of cognitive function affected by amnestic MCI has been a major contribution to AD research, particularly to the conduct of clinical trials.
Investigators pursuing many avenues of research have provided valuable additions to our storehouse of knowledge. Here are a few things we’ve recently learned about MCI:
- Genetic risk factors appear to play a role in MCI as they do in AD:
- Investigators at a number of research laboratories have found that people with MCI who also have the APOE-e4 allele progress to AD more rapidly than those without APOE-e4 (Fleisher et al., 2005; Petersen et al., 1995; Tschanz et al., 2006).
- In the recently completed 3-year Memory Impairment Study, one of NIA’s Alzheimer’s Disease Cooperative Study (ADCS) clinical trials (see "A Closer Look at Two Aspects of AD Clinical Trials" for more on the ADCS), investigators compared the effectiveness of vitamin E, donepezil, and a placebo in delaying the onset of a diagnosis of AD in 769 people with amnestic MCI (Petersen et al., 2005). In the subset of study participants who carried the APOE-e4 allele, donepezil appeared to decrease the risk of progression to a diagnosis of AD for the full 36 months of the study. For other participants, donepezil reduced risk of progressing to AD during the first 12 months of the study, but this benefit disappeared by 18 months. Vitamin E did not appear to slow the progression to AD.
- Different brain regions appear to be activated in cognitively healthy people and those with MCI during certain types of cognitive activities. Using brain imaging techniques, University of Pittsburgh investigators participating in the Ginkgo Evaluation of Memory (GEM) trial were able to detect differences in an aspect of cognitive function called attentional control (Rosano et al., 2005). These changes are likely to be related to early cognitive impairment. (see "A Closer Look at Two Aspects of AD Clinical Trials" for more about the GEM trial).
- The rate of brain atrophy can predict cognitive impairment and dementia. Investigators compared magnetic resonance imaging (MRI) scans over time in the same individuals with either normal cognition or MCI (Jack et al., 2005). They found that higher brain atrophy rates predicted increased impairment and dementia.
- Treatment with raloxifene (Evista), a selective estrogen receptor modulator used to treat osteoporosis, may reduce the risk of developing cognitive impairment and AD. The Multiple Outcomes of Raloxifene Evaluation (MORE) study was a prevention clinical trial conducted with nearly 5,400 postmenopausal women with osteoporosis (Yaffe et al., 2005). The women were divided into three groups: one group received a placebo, one group received 60 mg/day of the drug, and the third group received 120 mg/day. After 3 years of treatment, there was no difference between the 60 mg/day group and the placebo group. However, women who took 120 mg/day had a statistically significantly lower risk of developing amnestic MCI and a somewhat lower risk of developing AD and any cognitive impairment than did the women who took the placebo. (See "Putting Treatment Hypotheses to the Test in Clinical Trials" for a description of a treatment clinical trial in which investigators are examining raloxifene’s effect in women who already have AD.)
In addition to conducting studies like these, investigators are using a variety of sophisticated tools to push the boundaries of knowledge about the very early stages of the AD process. Several of these tools are described in greater detail in "Sophisticated Tools Help Investigators Learn More About Changes in the Brain".
 |
