|
|
|
| Environmental Medicine | CSEM | GREM | Continuing Education | Patient Education | PEHT | Community | |
Agency for Toxic Substances and Disease Registry
|
Learning Objectives |
Upon completion of this section, you should be able to
|
Introduction |
The two most important tests in diagnosing asbestos-associated disease are
Other tests and procedures that are sometimes used to diagnose asbestos-associated diseases by specialists in cases that require further work-up are
|
Screening Pulmonary Function Tests |
Screening pulmonary function tests are useful for finding restrictive deficits associated with parenchymal asbestosis (see table). Findings may include a reduction in forced vital capacity (FVC) with a normal Forced Expiratory Volume (FEV1)/FVC ratio. Some sources report abnormal pulmonary function tests in 50% to 60% of patients with asbestosis (Ross 2003). In some cases, combined patterns of restrictive and obstructive disease may be seen. For further assessment of whether a patient has a restrictive abnormality and asbestosis, additional, more specialized tests may be required
Consider consulting a pulmonologist if the diagnosis is unclear, if there is a rapid decline in pulmonary function, or if there is a need for a tissue biopsy or BAL, such as in cases where lung cancer, mesothelioma, or an infection is suspected. The pulmonologist may recommend more extensive pulmonary function tests. |
| Asbestos-Associated Disease | Pulmonary Function Test Findings |
|---|---|
Parenchymal asbestosis |
|
Asbestos-related pleural abnormalities |
|
Chest Radiograph |
The chest radiograph is used primarily to
Diagnosis of asbestosis should mostly but not totally be based on radiographic findings, per the diagnostic criterion of the American Thoracic Society. In 10% to 15% of cases, an asbestos-associated pulmonary function abnormality can occur without definite radiologic change (Ross 2003). The association of pleural thickening and calcification with interstitial changes enhances diagnostic accuracy of asbestosis. The American Thoracic Society includes radiographic findings as one of their criterion for making a diagnosis of asbestosis. In 1980, the International Labour Organization (ILO) developed a system for radiographic classification of the pneumoconiosis. Persons certified to use this rating system are called “B readers.” A current list of B readers can be found at http://www.cdc.gov/niosh/topics/chestradiography/breader-list.html. Detection of parenchymal asbestosis by chest radiography should be guided by the ILO system or other standard reading methods. A list of typical chest radiograph findings for each of the asbestos-associated diseases is in the table below. |
 |
 |
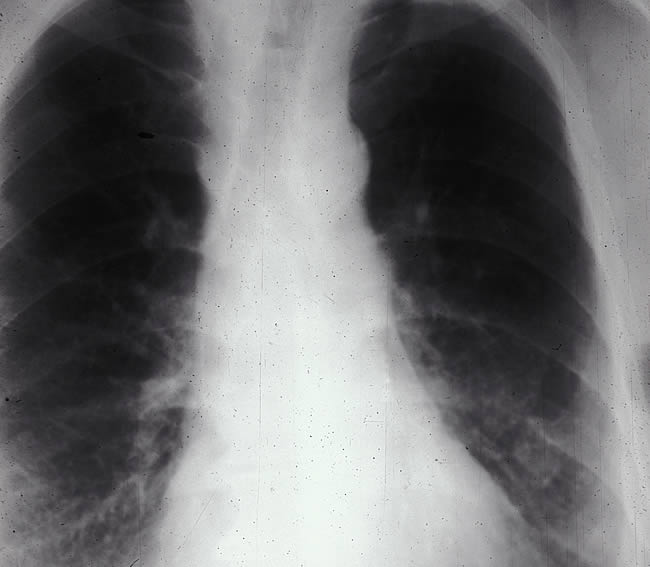 |
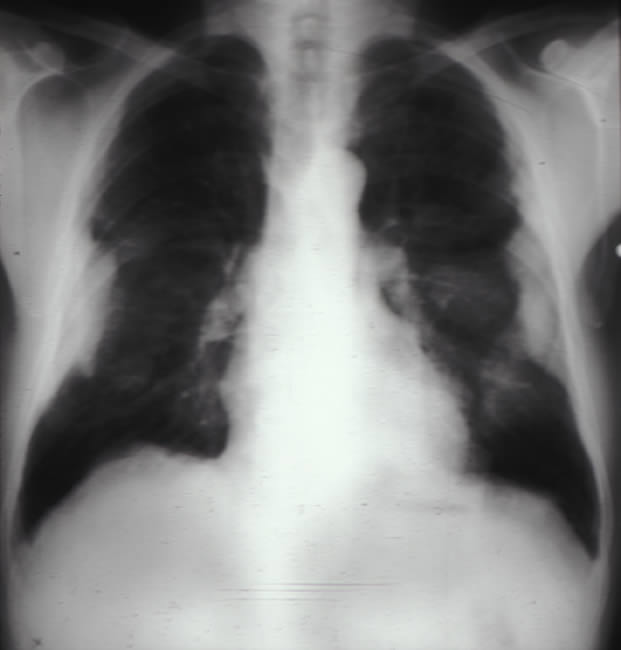
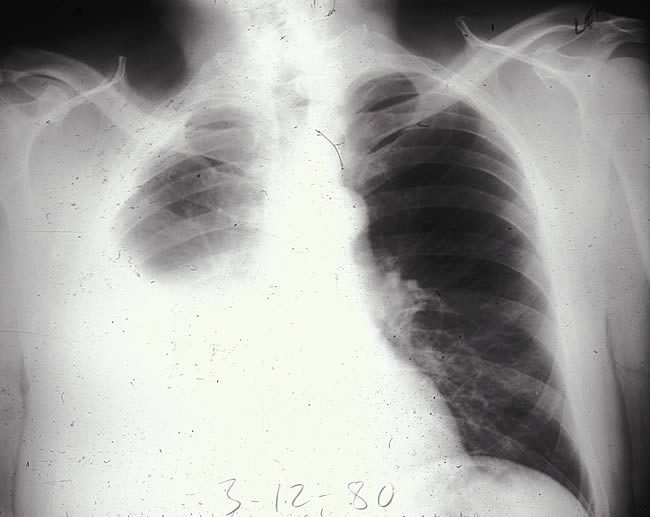
| Pleural Plaques | Pleural Mesothelioma | Parenchymal asbestosis |
| Asbestos-Associated Disease | Typical Chest Radiograph Findings |
|---|---|
|
Parenchymal asbestosis |
|
Asbestos-related pleural abnormalities |
Pleural Plaques
Benign Pleural Effusions
Diffuse Pleural Thickening
Rounded Atelectasis
|
|
Lung cancer |
Radiological appearance same as that of lung cancers with other causes, (i.e., solitary pulmonary mass with or without mediastinal lyphadenopathy). |
|
Mesothelioma |
May present as a
|
CT and HRCT |
In some cases, CT and HRCT scans can facilitate diagnosis of asbestos-associated diseases. Because they are associated with higher doses of radiation than conventional chest X-rays and their cost-effectiveness and efficiency as screening tools have not been established, CT scans should not be used for routine screening. They can be useful in further investigating abnormalities found on chest X-rays and in detecting abnormalities not seen on chest films of patients with dyspnea or pulmonary function abnormalities. CT and HRCT scans are more sensitive than chest radiographs. When B readers are not able to agree on the presence of asbestos-associated disease per the chest radiograph, CT and HRCT scans can be used (American Thoracic Society 2004). They are especially useful in detecting
ATSDR recommends low-dose CT scans for screening certain former vermiculite miners or vermiculite mill workers and their household contacts whose chest radiographs are indeterminate (Muravov et al. 2005). The utility of other imaging techniques such as ultrasound, gallium scanning, magnetic imaging, ventilation-perfusion studies, and positron emission tomography has not been established. New digital imaging techniques (e.g., digital radiography) are under development as well. |
BAL and Lung Biopsy |
BAL (bronchoalveolar lavage) is sometimes used by specialists to identify other possible causes for lung pathology and it can be used to determine the level of exposure to asbestos by measuring the amount and type of asbestos bodies in the lung tissue and lavage fluid (Santorelli et al. 2001; American Thoracic Society 2004). Special laboratory facilities for quantitating asbestos fibers must be available. Lung biopsy is a definitive test used in the histopathical confirmation of asbestos-associated diseases. Lung biopsies are rarely used to diagnosis asbestosis or pleural plaques, because diagnosis of these conditions is usually based on findings from the medical evaluation and other tests. Appropriate referral to a specialist is indicated if lung cancer or mesothelioma is suspected, since a lung biopsy may be indicated under these conditions. |
Blood Studies |
Arterial blood gas (ABG) and pulse oximetry are sometimes used to detect decreases in oxygen in the blood associated with the respiratory changes associated with asbestos-related disease. Blood chemistry studies may occasionally be useful for ruling out other causes of restrictive lung disease (e.g., rheumatoid lung disease, uremia, increased sedimentation rate). |
Colon Cancer Screening |
Some studies show that asbestos exposure increases a patient’s risk for colon cancer. Therefore, colon cancer screening should be considered in accordance with the American Cancer Society’s screening guidelines for colon cancer for people over age 50 American Thoracic Society 2004). |
False Positives and False Negatives |
It is important to know what other conditions bear radiographic similarities to changes associated with asbestos-related disease (see table). |
| Asbestos-Associated Disease | Similar Radiographic Appearance |
|---|---|
|
Parenchymal asbestosis |
|
|
Asbestos-related pleural abnormalities |
General differential diagnoses
Pleural plaques may be confused with
Benign asbestos pleural effusions may be confused with
Diffuse pleural thickening may be confused with
Rounded atelectasis
|
|
Lung cancer |
Lung cancer not related to asbestos. |
|
Mesothelioma |
All other causes of unilateral pleural masses. |
Attribution of Asbestos-Related Cause |
To help attribute pulmonary fibrosis to asbestos exposure check for the diagnostic guidelines suggested by the American Thoracic Society
Other findings that aid in attributing a disease to asbestos exposure include
Bilateral calcified pleural plaques are usually attributed to asbestos exposure, but single-sided pleural plaques may not be and a search for other causes such as old tuberculosis, empyema, or hemithorax may be indicated. CT scanning can be used to make a definite diagnosis of rounded atelectasis, if there are any questions (Khan et al. 2004). As stated previously, sets of diagnostic criteria like the Helsinki criteria can help determine if a lung cancer has any causal relationship to asbestos exposure. Malignant mesotheliomas are, for all practical purposes, related to previous asbestos exposure. |
Key Points |
|
Progress Check |
|
| Agency for Toxic Substances and Disease Registry 4770 Buford Hwy NE, Atlanta, GA 30341-3717 Contact CDC: 800-232-4636 / TTY: 888-232-6348 cdcinfo@cdc.gov |