|
 |

|
Print  Download Reader
Download Reader 
|
|
|
Print Download Reader
Testimony
June 23, 2005
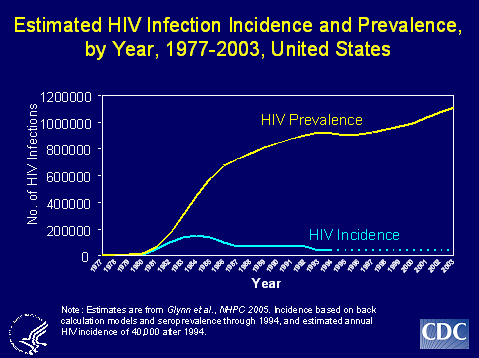
Introduction We are now in the third decade of the HIV/AIDS epidemic. To date, HIV has claimed the lives of more than 22 million people worldwide. In the United States, more than 500,000 people have died of AIDS. The number of new HIV infections annually has declined from more than 150,000 in the late 1980s to an estimated 40,000 a year today. What is more difficult to measure, however, are the countless Americans who have been spared from infection through prevention efforts implemented nationwide. While cases of disease can be counted, it is impossible to count what didn�t happen, namely, cases averted. In addition to the dramatic declines in the occurrence of new cases since the beginning of the epidemic, the HIV/AIDS epidemic has changed in other important ways. Initially, it primarily affected whites, but today the majority of those affected are people of color. Racial and ethnic minorities are disproportionately at risk for and affected by the HIV/AIDS epidemic. The epidemic also continues to have a great impact on men who have sex with men (MSM). Dramatic decreases in mother to child HIV transmission (perinatal transmission) are one of the great success stories of HIV prevention. Since 2000, CDC estimates that 280-370 HIV-infected infants are born in the United States each year -- a substantial reduction from the 1,000 to 2,000 perinatal HIV cases estimated to have occurred each year in this country in the early 1990s. These declines are due to multiple interventions, such as routine voluntary HIV testing of pregnant women, including the use of rapid HIV tests at delivery for women of unknown HIV status, and the use of antiretroviral therapy by HIV-infected women during pregnancy and infants after birth. We remain concerned about perinatal HIV transmission and reducing perinatal transmission is one of our key prevention goals. We continue to work to further decrease perinatal transmission by promoting active case management for high risk women, routine opt-out testing, and the use of rapid tests at labor and delivery for mothers whose status is unknown. We also have seen declines in the number of HIV and AIDS cases attributed to injection drug use. For example, the number of AIDS cases attributed to injection drug use has declined by about 15 percent from 1999 to 2003.
HIV/AIDS Trends Of great concern to us is that approximately 25 percent of those infected with HIV do not know they are infected. We believe that infections transmitted from this group account for more than half of new HIV infections each year, underscoring the rationale for our substantially increased efforts to reach at-risk communities with HIV testing services. Knowledge of one�s HIV infection can help prevent the spread of HIV to others. When people know their status they are more likely to protect their partners from infection.
Trends in Estimated HIV Diagnoses Looking at trends by risk, the annual diagnoses among MSM increased 11% during this four-year period, with the largest increase occurring between 2001 and 2002. MSM continue to constitute a substantial proportion of HIV cases�44% of cases in the period from 2000 to 2003. The increase in HIV diagnoses among MSM may be linked to a rise in use of crystal methamphetamine (crystal meth) among MSM. Crystal meth, a powerful, illicit drug that can reduce inhibitions, has been associated with high-risk behaviors and sexually transmitted diseases in multiple studies. The annual number of diagnoses associated with high-risk heterosexual contact remained roughly stable during 2000-2003; new diagnoses associated with injection drug use declined slightly. In 2003, the highest rate of HIV diagnosis was among African American males (103.4 per 100,000 population), with a rate almost seven times that of white males (15.2) and nearly three times the rate among Hispanic males (40.4) The rate of HIV diagnosis among African American females in 2003 (53 cases per 100,000 population) was more than 18 times higher than among white females (2.9) and almost five times higher than among Hispanic females (10.9). Among American Indians/Alaska Natives, the rate of HIV diagnosis among males (15.6) was slightly higher than the rate among white males; the rate among females (6.4) was twice the rate of white females. But studies show that cultural, socioeconomic, and health-related factors, in addition to barriers to risk reduction, may drive the HIV epidemic in communities of color.
Trends in AIDS Diagnoses and Deaths African Americans continue to be most severely affected by AIDS. In 2003, rates of AIDS cases were 58.2 per 100,000 among African Americans, 20.0 among Hispanics, 8.1 among American Indian/Alaska Natives, 6.1 among whites, and 4.0 among Asian/Pacific Islanders.
Trends in Persons Living with AIDS
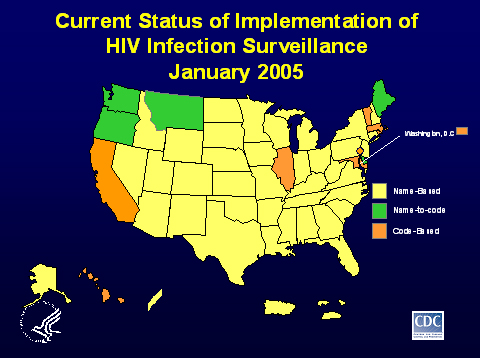
State HIV surveillance systems CDC is responsible for ensuring the integrity of the national HIV/AIDS surveillance system to accurately monitor the epidemic in the United States. CDC also provides funding, technical assistance, and coordinates activities with states to aggregate data that comprises the national system. As with other diseases, individual state governments have authority for statutory and regulatory issues for HIV/AIDS reporting and data protection, including the decision as to what type of system will be used for disease reporting, such as name-based or code-based. Except for HIV, all other reported infectious diseases, including AIDS, are routinely reported to states using name-based reporting systems. States remove names before submitting the data to CDC. Since the beginning of the epidemic, AIDS surveillance has been a cornerstone of national, state, and local efforts to monitor the scope and impact of the HIV epidemic. AIDS surveillance data, however, no longer accurately describe the full extent of the epidemic, as effective therapies slow the progression of HIV disease. Since 1999, CDC has advised states to conduct HIV reporting using the same name-based approach currently used for AIDS surveillance nationwide. Currently, 38 states and 5 territories have adopted name-based HIV reporting. Seven states, the city of Philadelphia, and the District of Columbia, have code-based reporting, and 5 states have name-to-code reporting. (See Figure 2, Current Status of Implementation of HIV Infection Surveillance, January 2005.) In the 14 areas using codes, 13 different codes are used. Except for HIV, all other reported infectious diseases are routinely reported to the states using name-based reporting systems. It is important to note, for confidentiality purposes, that the CDC does not receive the names of individuals. This information resides at the state level. Because all states do not use a uniform, name-based approach to HIV reporting, there are some limitations of the current, national HIV reporting data. These limitations include:
In 1999, CDC published a set of performance standards for HIV reporting systems. CDC reports HIV infection data only from areas conducting confidential name-based reporting because this reporting has been shown to routinely achieve high levels of accuracy and reliability. Confidential name-based surveillance systems have been shown to best meet the necessary performance standards. Studies have also shown that implementing code-based and name-to-code systems are more expensive to implement than confidential, name-based systems. And currently, only confidential name-based HIV reporting, integrated with AIDS surveillance data, can be used by states to identify and remove cases that are counted in more than one state (a process called de-duplication) before they are reported to CDC�s national surveillance database. The last Ryan White CARE Act reauthorization called for an Institute of Medicine study of states� HIV surveillance systems and their adequacy and reliability for the purpose of using such data as the basis for CARE Act formula grant allocation. The reauthorization also called for the Secretary to make a determination regarding the use of HIV data for CARE Act formulas. The Institute of Medicine issued a report, Measuring What Matters, on allocation, planning and quality assessment for the Ryan White CARE Act. Based on the report findings, in June 2004, the Secretary of HHS determined that �HIV data not be used for purposes of making formula grants under Titles I and II of the Ryan White CARE Act, and that estimated living AIDS cases continue to be utilized until such time as high quality HIV data are available nationwide.� To reach the goal of nationwide, high-quality HIV data, CDC is moving from �advising� to �recommending� jurisdictions use name-based HIV reporting. We continue to work closely with the states to help them adopt and implement high quality HIV surveillance systems. Having all states collect HIV information in the same manner will ensure that the nation has reliable and valid data to monitor the scope of the epidemic; plan for and evaluate prevention, care, and treatment programs; and focus those programs on persons most at risk. Thank you again for this opportunity. I will be pleased to answer any questions.
Figure 1
Figure 2 Last Revised: June 23, 2005 |