Considerations for Antiviral Drug Stockpiling by Employers in Preparation for an Influenza Pandemic
Topics on this Page
Summary Optimal planning and preparation for an influenza pandemic requires coordinated efforts by every part of society including individuals and families, communities, employers in public and private sectors, and all levels of government. Federal, State, and local governments will implement strategies to protect the public in an influenza pandemic. Employers also will play a key role in protecting employees' health and safety, thereby limiting pandemic impacts on health, the economy, and society. As part of their comprehensive pandemic planning, some employers (from public and private sectors) have asked for guidance about whether they should stockpile or otherwise arrange for influenza antiviral drugs to be available for their employees during a pandemic. Private stockpiles, in coordination with public health stockpiles, would extend protection more broadly than could be achieved through the public sector alone and improve the ability to achieve the national pandemic response goals of mitigating disease, suffering, and death, and minimizing impacts on the economy and functioning of society.
The Federal Government strongly encourages all public and private sector employers, regardless of size, to plan for a pandemic, to protect the health of employees and assure continuity of operations. Influenza antiviral drugs (antivirals) are one of several approaches to protecting people during a pandemic and can serve as an important part of a layered approach to pandemic mitigation. In some cases, employees whose jobs would normally involve very high or high exposure risk to known/suspected pandemic patients may reduce or eliminate exposure through engineering, administrative and work practice strategies. Nonpharmaceutical measures and personal protective equipment should also be used as a critical component of an employer's plan to protect employees during a pandemic. Employers that provide frontline healthcare and emergency services should plan to protect their employees who will be exposed to ill persons during a pandemic. This guidance recommends providing antiviral prophylaxis to these very high exposure risk and high exposure risk employees for the duration of community pandemic outbreaks to prevent illness. Businesses that provide goods or services essential to community health, safety, or well-being have an obligation to plan and prepare for continued operations in the event of a pandemic. As a part of comprehensive pandemic planning, these critical infrastructure employers should strongly consider providing antiviral prophylaxis for the small number of employees who are critical to essential operations. In addition, other employers may consider antiviral prophylaxis for workers in order to maintain business continuity.
If an employer is considering stockpiling antiviral drugs, it should do so with a clear understanding of the legal, regulatory, ethical, logistical, and economic issues that will be encountered in ordering, storing, securing and dispensing prescription medications. Employers should work with their company or contracted occupational health providers/services to plan for stockpiling antivirals. This guidance does not establish the requirement or expectation that all employers stockpile antiviral drugs; rather, it defines a prudent strategy for employer antiviral drug stockpiling and use that can contribute to a more effective pandemic response. Any employer that chooses to stockpile antivirals should do so as part of comprehensive pandemic preparedness and response activities in coordination with State and local pandemic preparedness plans and in conjunction with other measures to protect workers and maintain continuity of operations.
Antiviral drug stockpiles have been established at the Federal level and many States have also established stockpiles. Current recommendations focus on using up to 6 million courses of the Federally stockpiled antiviral drugs as part of a comprehensive public health response to contain the initial pandemic outbreak, wherever in the world it occurs, to reduce transmission when cases first appear in the United States, and to use the majority of stockpiled antiviral drugs to treat persons who have pandemic illness and may benefit from therapy.
Newly developed Federal guidance recommends expanding antiviral drug use to include prophylaxis (i.e., antiviral use to prevent infection in persons either before or after they are exposed to pandemic influenza) in healthcare and emergency services occupations, for people whose immunity is compromised by an underlying medical condition or treatment, and for people living in group settings (e.g., nursing homes) if an outbreak of pandemic disease occurs at the facility. The Federal guidance on antiviral use also suggests a potential benefit of prophylaxis for workers who are critical to providing essential community services but leaves decisions on how to identify approaches to purchase and stockpile antiviral drugs to support its implementation to employers. Household contacts of ill persons also may benefit from prophylaxis. However, further work is needed to assess the feasibility of stockpiling and providing antivirals for household contacts and to identify approaches to purchase and stockpiling the antiviral drugs to support its implementation. Despite expanding recommendations for antiviral drug use, there are no current plans for a commensurate expansion of public sector stockpiles and employers will have to take the lead role for protection of their workforce if these recommendations are to be implemented.
Employers may choose to purchase antiviral drugs for stockpiling for several reasons: (1) to provide prophylaxis for front-line healthcare and emergency services workers (fire, law enforcement, and emergency medical services [EMS]) whose occupations put them at very high or high risk of exposure and infection; (2) to provide prophylaxis for workers who are critical to essential operations in critical infrastructure businesses to sustain provision of essential community services; (3) to assure early treatment to employees who become ill; (4) to maintain business continuity; and (5) to protect overseas employees and operations where U.S. government pandemic response activities will not reach. In addition to defining an employer's antiviral drug strategy and which workers may be targeted, employers may also consider protecting workers who must travel during the pandemic and non-employees such as contractors or volunteers. Decisions on stockpiling should be made in the context of pandemic planning and preparedness, broadly, in which a range of protective measures are used to minimize employee infections during a pandemic, particularly for those employees at high risk for exposure to or severe diseases from complications of pandemic influenza. Nonpharmaceutical interventions such as isolation of ill persons, quarantine of household members, and social distancing will be the first line of defense for employers during a pandemic. Antiviral drugs are only one tool that should be counted on to help mitigate a pandemic influenza, as their ultimate effectiveness in treating pandemic illnesses cannot be predicted in advance. In addition, it is important that employers be aware of the potential impacts and potential side effects of antiviral medications, the legal requirements and strategies for stockpiling and dispensing, ethical considerations in providing antiviral medications to some portion or all of the workforce, as well as the current public sector stockpile strategies.
top of page
Purpose
The purpose of this guidance is to provide information to employers (both public and private sector) so that informed planning and implementation decisions on antiviral drug stockpiling for pandemic influenza can be made and, if drugs are stockpiled, to assure that they are maintained and used optimally. This guidance does not establish the requirement or expectation that all employers stockpile antiviral drugs. The Federal Government encourages employers to consider stockpiling antivirals for use during an influenza pandemic if stockpile plans are consistent with their overall pandemic preparedness plan and they have carefully considered the legal, ethical, regulatory, logistical, and economic implications of stockpiling antiviral medications. Employers are encouraged to coordinate their plans for antiviral stockpiling with State and local public health agencies to improve community-level response during a pandemic. It is recognized that antiviral stockpiling may not be a suitable strategy for many employers; nonpharmaceutical strategies, effectively planned and implemented can provide substantial protection for employees during a pandemic.
This guidance should be considered - interim- and should be reassessed as new scientific and technological advances are made, and at the time of the pandemic when the characteristics of the pandemic virus and patterns of an emerging pandemic are known.
top of page
Background
An influenza pandemic is a global disease outbreak of a new influenza virus for which people have little or no immunity. The disease spreads easily from person-to-person, causes serious illness, and can spread around the world and sweep across the country in a short time. When the next influenza pandemic will occur or how severe it will be are impossible to predict. Health professionals are concerned that the continued spread of a highly pathogenic avian influenza A (H5N1) virus across eastern Asia and other regions represents a significant pandemic threat. Since 2003, a growing number of human influenza A H5N1 cases have been reported in Asia, Europe, and Africa. More than 60 percent of the people infected with this avian virus have died. Although it is unknown whether this virus will evolve into one that causes a pandemic, scientists believe that future pandemics inevitably will occur, and wherever and whenever a pandemic starts, everyone around the world will be at risk.
The goals of the Federal Government's response to pandemic influenza1 are to:
(1) Stop, slow, or otherwise limit the spread of a pandemic to the United States;
(2) Limit the domestic spread of a pandemic, and mitigate disease, suffering, and death and
(3) Sustain infrastructure and mitigate impact to the economy and the functioning of society.
Protecting human health is of primary importance and will enable the achievement of preserving societal function as well as mitigating the social and economic consequences of a severe pandemic.
Federal, State, and local governments have primary responsibility for the public health response during a pandemic. There are multiple strategies for combating pandemic influenza, including: 1) providing vaccination, (2) isolating ill persons and recommending quarantine of well household members and other persons who may have been exposed to the virus but not yet have symptoms, (3) closing child care facilities, dismissing of students from schools, and keeping children and teenagers from re-congregating in the community, (4) decreasing the frequency and duration of close contact among people (social distancing), (5) using antiviral medications to treat or prevent illness, and (6) improving hand and respiratory hygiene and using personal protective equipment (PPE) such as facemasks (e.g., surgical masks) or respirators (e.g., N95 filtering facepieces) to reduce the chance of becoming infected if close contact with an infected person occurs (infection control). While a vaccine against the pandemic virus strain will provide the most durable protection against pandemic illness, it is unlikely that such a vaccine or only limited quantities of stockpiled pre-pandemic vaccine, may be available when the first U.S. pandemic wave begins. Once the pandemic strain emerges and is identified, based on current technologies, it will take at least 20 weeks before the first doses of a pandemic vaccine are available. After vaccine production begins, vaccine will become available incrementally depending on production capacity. Work is ongoing to shorten the time needed for pandemic vaccine development, expand production capacity, develop and expand stockpiles of pre-pandemic vaccines (vaccines made from currently circulating influenza viruses that may pose a pandemic threat and that may provide partial protection against a pandemic strain), and improve the number of doses and effectiveness of vaccines through the use of adjuvants - “ substances that increase the immune response to vaccination.
By contrast, antiviral drugs can be stockpiled in advance and therefore be available when a pandemic begins. Current strategies for use of antiviral drugs from Federal and State stockpiles include containing or suppressing an initial pandemic outbreak wherever it occurs in the world and when cases are first introduced into the United States, and treatment of persons with pandemic illness. With recent increases in antiviral drug production capacity, expanded antiviral drug use strategies are being recommended. Newly developed Federal guidance5, developed with input from multiple Federal agencies and from State, local and tribal public health agencies, includes recommendations for prophylaxis for the duration of a community outbreak for front-line healthcare workers and emergency service providers (e.g., Emergency Medical Services personnel, fire fighters, and law enforcement personnel); and recommendations for post-exposure prophylaxis (PEP) for less frequently exposed healthcare and emergency response workers, severely immunocompromised persons who may not be protected by vaccination, and persons living in group settings such as nursing homes or prisons in the context of an outbreak at the facility. Although PEP among household contacts of persons with pandemic illness may provide individual and community benefits in disease prevention, implementation issues have not been resolved.
While there is no national recommendation for prophylaxis of critical infrastructure workers outside of the healthcare and emergency services sectors, employers in businesses that support essential community services should plan and prepare for an influenza pandemic so that critical services are maintained. Antiviral prophylaxis provided to a small number of these employees (who are critical to essential operations) for the duration of a community pandemic outbreak may serve as an important strategy to ensure critical services are not disrupted by worker illness and absenteeism. The Federal Government is "leading by example" in this regard; each Agency is assessing the amount of antivirals needed for employees who provide healthcare or emergency care services and the small number of other employees who perform critical functions and efforts to stockpile antivirals for these workers are underway.
Four antiviral drugs (amantadine, rimantadine, zanamivir, and oseltamivir) are approved by the FDA for treatment and/or prevention of influenza. Two agents, oseltamivir (Tamiflu ®) and zanamivir (Relenza ®), are currently being purchased for the Centers for Disease Control and Prevention's (CDC- ™s) Strategic National Stockpile (SNS) for use during a pandemic. (See Appendix 1 for more information on these medications) These drugs have also been made available for State purchases for State-level stockpiles. Amantadine and rimantadine are not recommended for use against currently circulating influenza A viruses or influenza A (H5N1) viruses because many such strains are resistant to these drugs. Moreover, drug resistance to these agents develops rapidly when they are used for treatment. By contrast, drug resistance to oseltamivir and zanamivir has been uncommon among circulating human and avian influenza viruses to date.
Oseltamivir and zanamivir have been shown to reduce the duration of symptoms in patients with seasonal influenza illness by 1 to 1 ½ days when begun within the first 48 hours of illness. When treatment is begun earlier, benefits are likely to be greater; a Canadian study reported that the duration of seasonal influenza was about 3 - 4 days shorter when patients presented for treatment within 12 hours of illness onset. In addition, a pooled analysis of clinical trials reported that treatment decreased respiratory complications of pneumonia and bronchitis and decreased rates of hospitalization for persons ill with seasonal influenza when taken within 48 hours of the onset of the illness. Thus, implementation planning for antiviral treatment in a pandemic should stress early care seeking and initiation of therapy. One study also suggests that treatment of persons with seasonal influenza infection at hospital admission may reduce the risk of death from influenza or its complications.
There is no experience using oseltamivir or zanamivir during a pandemic because no pandemic has occurred since these drugs have become available. Laboratory studies of influenza A H5N1 virus strains show sensitivity to oseltamivir and zanamivir. Studies of oseltamivir in animals suggest that it has activity against the avian H5N1 virus. People infected with influenza A H5N1 viruses who are treated with oseltamivir early in the course of their illness have been less likely to die compared with those who did not receive treatment., Recent guidance issued by the World Health Organization recommends the use of oseltamivir as the primary treatment of choice for the current situation with sporadic influenza A (H5N1) virus human infection. Antiviral medications given as prophylaxis shortly after exposure to a family member with seasonal influenza have been shown to reduce the risk of illness by 70 to 90 percent., By preventing infection in close contacts of persons with pandemic illness, prophylaxis also may limit ongoing transmission within communities, reducing overall pandemic impacts. Results from mathematical models of pandemic spread suggest that antiviral post-exposure prophylaxis in households could reduce the spread of pandemic infection in households and communities, thus reducing the total number of people who suffer pandemic illness and its consequences.,, Implementation of a post-exposure prophylaxis strategy requires sufficient antiviral drug supply and effective methods to deliver the medication shortly after exposure occurs (i.e., within 48 hours). Current antiviral drugs in the SNS and State stockpiles purchased off of Federal subsidized contracts are not sufficient to allow for household prophylaxis. Current Federal and State stockpiles have been reserved primarily for the treatment of ill patients.
Whether or not employers make antivirals part of their pandemic preparedness strategy, early use of nonpharmaceutical measures should be employed to protect employees during a pandemic6. Approaches include changing workplace practices to decrease the frequency and duration of close contact (within 6 feet) among workers (e.g., holding conference calls instead of in-person meetings, and promoting tele-working and flexible scheduling); encouraging employees not to report to work if ill with influenza-like symptoms and allowing leave when a worker or household member is sick; and providing education and materials to promote hand and respiratory hygiene and supporting the use of facemasks or N-95 respirators and other personal protective equipment, where appropriate under OSHA guidance or other recommendations., Guidance on comprehensive pandemic planning for businesses and employers has been provided by the Federal Government. 2,
top of page
Process of Developing this Document
The U.S. Department of Health and Human Services (HHS) convened a Federal agency working group to examine possible recommendations for employer stockpiling that included representatives from Federal agencies and obtained input from State and local public health experts as well as representatives from public health organizations, boards of pharmacy groups, employers and business organizations. The recommendations were vetted through Federal agencies and were posted for public comment in the Federal Register. All working group members were free from conflicts of interest with antiviral drug manufacturers and manufacturers did not present to the working group or influence its deliberations. The working group used the same pandemic planning assumptions in the development of this document as was used in the development of the overall antiviral use strategy guidance. 5
top of page
Stakeholder Engagement
Consistent with ethical principles of transparency and inclusiveness and recognizing the value of public input in developing policy, representatives from the working group met with stakeholders in State and local government, public health, healthcare and emergency services, businesses, organized labor, and the public. Objectives of these meetings were to obtain input on the proposed recommendations; identify potential barriers to implementation; and define interventions that would facilitate implementation. Overall, 13 meetings were held with representatives from about 400 organizations who participated either in-person or by telephone. From this process, comments consistently indicated that employers needed guidance to adequately plan and prepare for antiviral stockpiling and agreement with expanding the antiviral drug guidance to include prophylactic uses, including support for a recommendation of outbreak prophylaxis for healthcare and emergency services personnel who have frequent exposure to persons with pandemic influenza infection. During these meetings, several barriers were identified to employer stockpiling. These included cost of the medication as well as issues related to storing and dispensing, the shelf-life of the drugs, legal issues and potential liability concerns for employers, logistical issues, and the potential for local or State government seizure of stockpiled drugs.
top of page
Roles and Responsibilities
The National Strategy for Pandemic Influenza published in November, 20051, recognized that effectively preparing for and responding to a pandemic requires coordinated action at all levels of government and in the private sector. The National Strategy is guided by the following principles:
- The Federal Government will use all instruments of national power to address the pandemic threat.
- States and communities should have credible pandemic preparedness plans to respond to an outbreak within their jurisdictions.
- The private sector should play an integral role in preparedness before a pandemic begins, and should be part of the national response.
- Individual citizens should be prepared for an influenza pandemic, and be educated about individual responsibility to limit the spread of infection if they or their family members become ill.
- Global partnerships will be leveraged to address the pandemic threat.
The States and Federal Government have established a target to stockpile 81 million courses of antiviral medications as part of public health preparedness for a pandemic. The Federal Government through CDC's Strategic National Stockpile (SNS) has purchased 50 million courses of antiviral drugs. An additional 31 million courses are targeted for purchase by the States under a Federal contract that subsidizes 25 percent of the cost of the antiviral drugs. Together, Federal and State antiviral stockpiles (if all States buy their full allocation) are predicted to be sufficient for treatment of those who are ill with pandemic disease and who may benefit from therapy based on assessment of medical need.
Whereas Federal guidance expands antiviral drug use recommendations to include prophylaxis for healthcare and emergency services personnel and, consistent with this document, suggests that employers more broadly consider antiviral prophylaxis as part of comprehensive pandemic planning, there has been no decision to expand public sector antiviral stockpiling to support these additional uses. Within the context of pandemic planning and preparedness being a shared responsibility of the government and the private sector, employers should not anticipate that antiviral drugs stockpiled by the Federal Government will be available for prophylaxis of their essential workforce. Employers considering antiviral prophylaxis, especially in healthcare and emergency services, are encouraged to talk with their State health department to understand whether support may be available.
Until recently, due to limited global production capacity and scarce supply of antiviral drugs, the Federal Government recommended against private sector stockpiling because it could delay the ability to meet national goals and divert supply needed to treat persons with seasonal influenza illness. Substantially increased global antiviral drug production capacity now makes stockpiling by employers feasible.
top of page
Issues for Planning for an Antiviral Stockpile
Public sector strategies for antiviral medications
Evolving Federal strategies for antiviral drug stockpiling and use are described above. Currently, States are developing plans for allocating, distributing, and dispensing antiviral medications during a pandemic. Distribution of antivirals from Federal and State stockpiles will be primarily the responsibility of State and local authorities. Potential venues for dispensing antiviral medications from these stockpiles during a pandemic include pharmacies, or specified points of dispensing (PODs) which may include public health sites, community health centers, outpatient offices and clinics, emergency departments, hospitals, occupational clinics, workplaces, pre-hospital emergency medical services, and other locations.
Plans and strategies will be periodically reviewed and will be re-assessed at the time of a pandemic when characteristics of the pandemic are known, including its severity, the characteristics of the disease and the groups at highest risk of influenza complications and death. Recommendations may also be updated as more is learned about the effectiveness of antiviral use strategies and when an effective influenza vaccine becomes available during a pandemic.
top of page
Relationship between public sector and employer antiviral stockpiles
Employers are encouraged to communicate and coordinate their comprehensive pandemic preparedness plans (including strategies for stockpiling antivirals) with relevant local and State public health officials. Collaborative planning and response efforts between the public sector and employers will afford communities the best chance to protect lives and preserve the functioning of the community during the time of a public health crisis like a severe influenza pandemic. Sharing information on antiviral drug plans can lead to coordinated use to best meet common public and private sector pandemic response goals. Employers also are encouraged to ask health providers and healthcare facilities that are dispensing antivirals on the employer's behalf to report cases of pandemic illness to State and local health agencies. At the time of a pandemic, CDC and State and local health officials will provide specific guidance to healthcare providers for reporting of cases of pandemic influenza and timing and appropriate use of antiviral medications based on the emergent pandemic virus strain and epidemiologic characteristics of the pandemic.
The Federal Government recognizes that one perceived barrier to coordinated planning and to employer antiviral stockpiling is the question of whether a State or local government agency might seize an employer's supply during a pandemic. Because of the magnitude of the threat that a severe pandemic poses to public health and society, Federal doctrine posits that an optimal response will require the effective and coordinated action by all levels of government, the private sector, communities, and individuals and families. In this context, actions that might inhibit planning and preparedness are counterproductive. Collaboration between State and local public health agencies and employers is important for an effective and seamless pandemic response. Given the substantial level of shared responsibility proposed for antiviral stockpiling and implementation, coordination is particularly important. On October 10, 2008, the Secretary issued a declaration under the Public Readiness and Emergency Preparedness (PREP) Act covering oseltamivir and zanamivir. Under the PREP Act, the Secretary may specify that liability immunity is afforded to the extent countermeasures such as influenza antivirals are obtained through a particular means of distribution. In the influenza antivirals (oseltamivir and zanamivir) declaration, the Secretary specified that liability immunity is provided to governmental program planners, e.g. State and local governments, including tribes, to the extent they obtain antivirals through voluntary means of distribution. The Secretary made this specification based upon his finding that the possibility of governmental program planners obtaining antivirals other than through voluntary means would - œundermine national preparedness efforts and should be discouraged.- Concern about potential seizure of stockpiled drugs is being addressed by a working group of public health and business representatives, convened by the Association of State and Territorial Health Officials (ASTHO). This group is developing strategies and model agreements to enhance coordination and reduce risks to organizations that stockpile antiviral drugs. Employers engaged in stockpiling activities are strongly encouraged to work with State and local health agencies to coordinate activities and investigate opportunities to establish agreements on this issue.
top of page
Legal and liability issues
Employer purchasing and stockpiling of antiviral drugs must comply with applicable Federal and State laws and regulations. These laws and regulations provide important public health protections by, among other things, establishing standards for the storage, handling, distribution, securing and dispensing of drugs; providing appropriate regulatory oversight to ensure that standards are met; and ensuring that licensed health professionals are involved in determining and prescribing specific drugs that are medically appropriate for the needs of specific patients. Employers that are considering stockpiling antiviral drugs or are arranging for others to provide or store drugs for the use of their employees should consider consulting with knowledgeable professionals to determine whether they should include antivirals in the company's pandemic planning strategy, whether to stockpile, and how to ensure compliance with all applicable legal requirements. Compliance with these storage and stockpiling requirements helps ensure that these drugs retain their safety and effectiveness for use in the event of an influenza pandemic.
The legal requirements that apply to employers interested in stockpiling and dispensing antivirals as part of preparing for an influenza pandemic will vary, depending on what approach to these activities is pursued. Given that storage and dispensing prescription medications are significantly regulated by States (practices of medicine and pharmacy, wholesale distribution of drugs, and dispensing of drugs), it is recommended that employers review State laws and consult with their State Boards of Pharmacy, or as appropriate, other State health offices, to determine what laws and regulations would be implicated by various approaches under consideration. Federal laws may also be implicated. Employers also may want to consult with their occupational health providers (if applicable), legal counsel, health insurance, and other insurance carriers as they consider planning for stockpiling antivirals. As an overall matter, employers should be guided in their relationship with their employees not only by Federal, State, or local employment laws, but by their own employee handbooks, manuals, and contracts (including bargaining agreements). In addition, employers should address any applicable privacy and discrimination issues that may arise in deciding who will receive antivirals or in dispensing the drugs.
An additional consideration for employers is potential liability associated with implementing an antiviral drug program for employees. The aforementioned PREP Act declaration provides immunity from tort liability (except for willful misconduct) to entities and individuals involved in the development, manufacture, testing, distribution, administration, and use of oseltamivir and zanamivir in accordance with the terms of the Secretary's declaration. The immunity covers claims of loss caused, arising out of, relating to, or resulting from administration or use of oseltamivir and zanamivir. The declaration defined "administration of [oseltamivir and zanamivir]" to include "public and private delivery, distribution, and dispensing activities relating to physical administration of the countermeasures to recipients, management and operation of delivery systems, and management and operation of distribution and dispensing locations."
top of page
Ethical concerns
If an employer is considering purchasing and stockpiling antiviral medications for use during a pandemic, there are several key ethical issues that must be included in the planning process. Decisions regarding which employees receive medications and under what circumstances may raise concerns about equity. Ethical principles that can guide planning for antiviral stockpiling should include:
- Decision-making processes must be informed by science, be transparent, and be inclusive of a range of community values.
- Employers should carefully consider criteria by which employee sub-populations, contractors, or groups would be provided antiviral medications and the objective business reasons for selecting some groups versus others. Targeting resources, such as antivirals, to specific groups may help reduce the overall impact of a pandemic and help preserve the health, safety, and essential functioning of the community. If certain workers are needed to perform essential functions for which their risk of illness is increased, protection by the use of antivirals and other means may be warranted.
- If antivirals are provided only to workers who have occupational exposure or who perform critical job functions (or based on other criteria), but not other workers, the employer should be explicit to all employees regarding the exposure criteria and other objective reasons for this strategy.
- A principle of fairness requires that all persons in a similar situation have similar access to the medication. Providing antivirals should not be based on gender, race or ethnicity and all persons within a defined target group should have similar access.
- Other issues regarding equity may arise as employers develop their plans for antiviral stockpiling in settings located overseas; these ethical and equity considerations must be incorporated into an overall plan that is consistent with anti-discrimination policies, the laws and culture of the overseas location, standard business practices, and corporate culture.
top of page
Determining antiviral drug use strategies and the amount of antivirals to stockpile
Decisions on the strategy for using antiviral drugs and the amount to purchase for a stockpile should be made in the context of overall pandemic planning by the organization and be consistent with Federal guidance for use. Employers should recognize that various nonpharmaceutical and infection control measures are available to protect workers and maintain essential business functions, thus reducing the need for antiviral prophylaxis. In some cases, employees whose jobs would normally involve very high or high exposure risk to pandemic influenza may reduce or eliminate exposure to known/suspected pandemic patients through engineering, administrative and work practice measures. Workplace exposures can be reduced by changing practices to decrease close contact between workers and the public and among workers by creating greater physical distances between people in the workplace, having conference calls instead of meetings, and promoting teleworking and flexible scheduling, among other strategies. Educating workers not to report to work if ill with influenza-like symptoms and allowing leave when a household member is sick also will reduce workplace exposures. Providing education and materials to promote hygiene and the use of facemasks and other personal protective equipment, where appropriate under OSHA recommendations, may reduce the risk exposure to influenza if workplace contacts would occur.
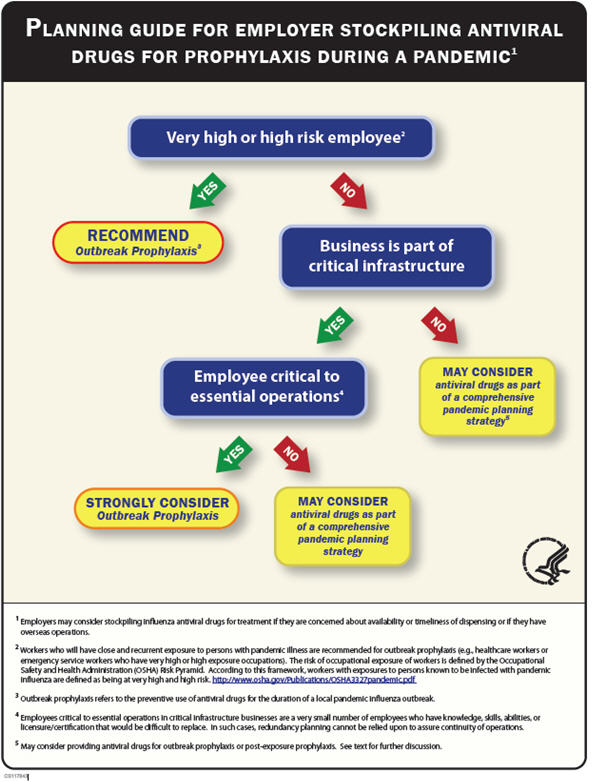
- Outbreak prophylaxis - Outbreak prophylaxis refers to the preventive use of antiviral drugs for the duration of a local pandemic influenza outbreak, potentially up to 12 weeks. A key consideration is the risk of occupational exposure of workers as defined by the Occupational Safety and Health Administration (OSHA) risk pyramid. According to this framework, workers with high potential for exposure to known or suspected sources of pandemic influenza virus are defined as being at very high and high risk; those who have unavoidable and frequent close contact with persons not known to be infected are defined as being at medium risk; and those without frequent close contacts are defined as being at lower risk. Persons who will have close and recurrent exposure to persons with pandemic illness (e.g., healthcare workers or emergency responders who have very high or high exposure occupations) are recommended for outbreak prophylaxis. Outbreak prophylaxis (in combination with other protective measures) may be particularly useful for increasing worker confidence and may discourage unnecessary absenteeism due to fear of becoming ill. In healthcare and emergency service sectors, workers who provide direct patient care and have high-risk exposure must be identified, and plans must be made for dispensing antivirals to support outbreak prophylaxis when local circulation of the pandemic virus is first identified.
- Outbreak prophylaxis also should be strongly considered for workers who are individually critical to provision of essential services in critical infrastructure businesses. By contrast with healthcare and emergency services, these critical workers, in general, will not have high-risk occupational exposure to pandemic infection, as defined by the Occupational Safety and Health Administration's risk pyramid. Employees critical to essential operations in critical infrastructure businesses, are a very small number of employees who have knowledge, skills, abilities, or licensure/certification that would be difficult to replace, for example, persons who keep the electric power grid operating, those who assure liquidity of the money supply, Air Traffic Controllers, and nuclear power plant engineers. In such cases, redundancy planning cannot be relied upon to assure continuity of operations.
- Employers may consider including antivirals for outbreak prophylaxis for other employees as well, although post-exposure prophylaxis may provide adequate and more appropriate protection (see below). A Planning Guide that provides an algorithm to help an employer make decisions about which employees may benefit from outbreak prophylaxis is provided in Appendix 2. Further information about antiviral use may be found here: http://pandemicflu.gov/vaccine/antiviral_use.pdf. Outbreak prophylaxis may protect a recipient for as long as the drug is being taken. If antiviral prophylaxis is used for the duration of a community pandemic wave (estimated to last up to 12 weeks), each person on outbreak prophylaxis would require up to 8 antiviral drug regimens.
- Post-exposure prophylaxis - Post-exposure prophylaxis (PEP) refers to the preventive use of antiviral drugs within 48 hours of close contact with someone who has pandemic illness. Based on experience with seasonal influenza, when used appropriately, antiviral drugs can be very effective in preventing infection in the exposed person. Challenges for an employer in implementing PEP include identifying when a risky exposure has occurred, who has been exposed, and how to provide the antiviral drug within 48 hours of exposure. During a pandemic, consultation with public health officials to help in making these decisions likely will not be available. Therefore, employers should create a plan to determine how exposures will be identified and how those employees will receive PEP. In addition, employers would need to decide whether to provide PEP only following workplace exposures or for exposures which may include those in the home or community and how that would be determined. PEP requires a single regimen of antiviral drugs (a regimen is defined as 10 drug doses). Planning the amount of drug to stockpile requires defining the number of workers who would be eligible for PEP and the proportion who may be exposed. In addition, because PEP only would afford some protection for the time the drug is being taken, workers may require more than one course of PEP during a 12-week pandemic outbreak. No national guidance is available regarding the number of regimens to stockpile per worker because exposures likely will differ in different community and workplace settings. Moreover, the use of other pandemic response measures (including engineering, administrative and work practice measures) may decrease the number of exposures that may lead to initiation of PEP. Stockpiling one to two antiviral regimens per targeted worker may be a reasonable estimate
- Treatment - Although public sector stockpiles are targeted for treatment of those who have pandemic illness and may benefit from therapy, employers may consider stockpiling antiviral drugs for treatment if concerned about the availability or timeliness of treatment using this supply. This may particularly be a concern for employers with overseas operations. Treatment requires a single antiviral drug regimen and thus, the amount stockpiled would be based on the number of employees targeted for treatment and their risk of becoming infected. National stockpiling targets have been established to be adequate to treat 25 percent of the population.
In addition to defining an employer's antiviral drug strategy and which workers may be targeted by each approach, employers may consider protecting workers who must travel during the pandemic and non-employees such as contractors or volunteers. Knowledge of and coordination with State plans and the capabilities of an employer to implement an effective antiviral drug program also are key considerations.
top of page
Antiviral prescribing, storage, and dispensing from an employer stockpile
Antiviral drugs are prescription drug products and should be prescribed to employees consistent with applicable State prescribing laws after medical screening for contraindications. Planning also must include appropriate receipt and storage of the antiviral stockpile and appropriate dispensing in accordance with applicable law. Prescription drugs such as antivirals held by employers must be legally dispensed according to State and Federal law. Under State law and the Federal Food, Drug, and Cosmetic Act (FDCA), prescription drugs may be dispensed only to individuals upon a written prescription or an oral prescription promptly reduced to writing that complies with State law, or by refilling such a prescription. Thus, under applicable law, an employer could not directly distribute a prescription drug to its employees without a prescription or outside the lawful dispensing process established under State law. A healthcare provider may prescribe a drug to his or her individual patient for use as directed by the healthcare provider (potentially including for use at a later time, if consistent with State law). Additionally, prescription drugs must be dispensed with labeling that complies with State and Federal law.
top of page
Stockpiling and dispensing models for consideration
There are several models that may be used by employers for stockpiling and dispensing antivirals during a pandemic. Selection of the best model for an employer to use should be made in coordination with healthcare providers who will be prescribing the antiviral medications. These models include:
A. Triggered- dispensing of antivirals at the time the pandemic occurs
Several methods can be considered for stockpiling antiviral drugs for dispensing at the time a pandemic is announced. Employers need to include plans for rapidly dispensing antivirals to employees when the pandemic emerges (either overseas or in the U.S.) Storing and dispensing antiviral drugs from an on-site or off-site State-licensed pharmacy is a method that will assure that drugs are stored in an appropriately maintained, secure environment and dispensed according to State law. Other facilities from which drugs may be legally dispensed include occupational healthcare facilities, healthcare practices/physician's offices, or clinics. Requirements for the storage and dispensing of drugs from these sites vary from State to State. Employers interested in this approach should review with their existing pharmacies, occupational health providers or other healthcare providers, or healthcare facilities, all proposed stockpiling plans to determine whether existing law allows them to store and dispense drugs, under what conditions such storage and dispensing is allowed and whether additional licenses or standards must be obtained or met. This option, using a company or contracted pharmacy or occupational medical service for stockpiling, might afford an employer is one practical approach to stockpiling antivirals.
Alternately an employer may choose to contract with a pharmaceutical manufacturer or wholesale distributor to hold a predetermined quantity of antiviral drugs and then transfer these drugs to an appropriate entity (such as a pharmacy, healthcare clinic or physician's office) for dispensing to employees by prescription during a pandemic. New programs have been developed by antiviral drug manufacturers to assist employers in storing and dispensing these drugs at the onset of a pandemic. Issues of cost and shelf-life may be mitigated through these new programs where organizations pay a small annual fee per regimen for the manufacturer to hold a contracted quantity of antiviral drug and assure current dating; at the time of a pandemic, this drug would be delivered within 48 hours of request with payment of the retail drug cost. Another option is to contract with a wholesale distributor of drugs for stockpiling and dispensing. These distributors are subject to Federal and State laws and regulations. State regulations for wholesale distributors must meet minimum Federal standards, although States may adopt regulations that are more stringent. Any employer contemplating utilizing this model should identify from the distributor or others the applicable State legal requirements, including identifying to whom a wholesale distributor may provide drugs.
Employers that do not have healthcare facilities or pharmacies on their premises and are considering stockpiling drugs on-site should be aware that storing antiviral drugs would subject them to State and Federal regulation. Depending on what activities the employer is engaged in, it could be subject to different regulatory oversight, including State pharmacy laws. These State and Federal requirements would, among other things, address the proper procurement, storage, handling, distribution, and dispensing of drugs. Employers need to consult with State Boards of Pharmacy or as appropriate, other State health offices for specific guidance on this approach.
B. Pre-pandemic dispensing
Some employers are considering acquiring, prescribing, and dispensing antiviral drugs to employees before a pandemic rather than maintaining them in a stockpile. Consideration of a pre-pandemic distribution model has arisen from uncertainties if there will be sufficient time after a pandemic has emerged for prescribing and dispensing because of the global dynamics of pandemic spread, and the potential for community disruption. One option to address this concern may be to complete pre-pandemic screening and keep a prescription on file for each employee before the pandemic starts to facilitate rapid dispensing at the time a pandemic occurs. Additionally, some employers are considering pre-pandemic dispensing because of concerns about possible public sector appropriation of employer stockpiles. (See previous section regarding this issue). Dispensing drugs during a pandemic outbreak for treatment or post-exposure prophylaxis may be challenging because of the burden that a pandemic will place on healthcare.
If physicians are prescribing antivirals using a pre-pandemic dispensing model, dispensing should be based on individual physician-patient consultations. Continuity of interaction between the patient and healthcare provider prescribing the antiviral in advance of a pandemic is recommended, to promote the appropriate use and storage of the drug and to provide a point of contact to monitor medication administration and potential adverse effects. Dispensing medications prior to an event without physician-patient consultation should not be part of the company's strategy. Dispensing should take place from a licensed pharmacy or licensed facility, such as an occupational healthcare facility, healthcare practice/physician's office, or clinic, depending on applicable State law.
Several potential disadvantages or risks are associated with a pre-pandemic dispensing approach. Because of employee turnover, persons included in the program may no longer be working for an employer when the pandemic occurs and those who have been recently employed may not be included. There also is a risk of inappropriate storage leading to reduced drug potency. Dispensed antiviral medications are subject to State pharmacy board regulations and generally, expiration dates are six to twelve months after dispensing. In addition, drugs stored at home may be used inappropriately before the pandemic or for a non-influenza illness during the pandemic that is mistakenly believed to be influenza. If antivirals are taken improperly or used before a pandemic (e.g. to treat an influenza-like illness), this may potentially contribute to the emergence of drug resistant viruses. Potential changes in an employee's health status from the time a prescription is dispensed to time of use and potential for secondary unauthorized distribution also should be considered.
An approach that reduces the potential problems of pre-pandemic dispensing while also avoiding the concern that disruption of healthcare services during a pandemic may compromise timely dispensing, would be to prescribe and distribute stockpiled antiviral drugs under the care of a healthcare provider (consistent with the above described models) when the pandemic is imminent - i.e., when an initial pandemic outbreak first occurs anywhere in the world.
top of page
Special considerations by employers with overseas operations
U.S. employers with overseas operations or locations may have special considerations when planning for a pandemic. Employers need to determine if in-country medical services and/or medications will be available for employees during a pandemic. Employers also need to understand local and national pandemic policies and plans and coordinate their plans with the host country and embassy. There is no current Federal plan for allocation of public sector stockpiles to private employers or employees located outside the United States, nor are such provisions anticipated. Employers should consider a wide range of issues when evaluating whether to include antiviral medications in a pandemic plan for overseas employees and particularly should include ethical and equity considerations in determining which employees will receive antiviral medications provided by the employer. In addition to importing, storing and dispensing medications consistent with local laws and regulations, employers should consider potential implications of antivirals being available for employees but unavailable to members of the local community. Additional considerations regarding enhanced security requirements and the possibility that antiviral supplies could be seized by either the host government or by other national entities at borders during transportation may be applicable depending on the location. The U.S. Department of State, Consular Affairs has issued the following statement that may help U.S. businesses with overseas operations understand the availability and limitations of US Government assistance abroad during the time of a pandemic:
- The Department of State lacks the legal authority to provide any type of medication, including Tamiflu®, to private American citizens.-
top of page
Additional issues
Possible antiviral resistance
The effectiveness of antivirals against a new pandemic influenza virus cannot be predicted. Influenza viruses may become resistant to antiviral drugs. Although influenza activity in the first part of the 2008 – 2009 season was low in the United States, preliminary data from a limited number of States indicated that the prevalence of influenza A (H1N1) virus strains resistant to the antiviral medication oseltamivir was high.[45] Other circulating seasonal influenza and H5N1 viruses remain susceptible to oseltamivir. No resistance to zanamivir has been detected. Antiviral resistance may limit or eliminate the effectiveness of treatment and prophylaxis for those infected with a resistant virus. Enhanced surveillance for influenza antiviral resistance among seasonal and novel influenza viruses such as H5N1 viruses is ongoing at CDC. Resistance among seasonal influenza strains does not predict resistance among pandemic influenza viruses. It is unknown whether resistance to zanamivir or oseltamivir may become a problem with widespread use of the drugs during a pandemic. Recognizing the uncertainties around potential antiviral resistance, HHS continues to recommend that employers consider antiviral stockpiling as part of a comprehensive pandemic response. Employers that are stockpiling antivirals to treat ill employees should arrange for healthcare providers to monitor those patients (and collect laboratory specimens) for signs of failed treatment (e.g. symptoms worsening during therapy) as those patients may be infected with viruses resistant to the antivirals and/or may have other complications needing different diagnostic and therapeutic interventions.
Appropriate environmental conditions for stockpiling
Storage and distribution of antiviral drugs by on-site or off-site State-licensed pharmacies will ensure that appropriate environmental conditions are maintained. For antiviral drugs stored in other licensed facilities, such drugs must be stored under appropriate conditions as stated in the FDA approved package insert. As with all medications, keep out of the reach of children.
Approved expiration dates for antiviral drugs
The current FDA-approved expiration date for oseltamivir (Tamiflu ®) and zanamivir (Relenza®) is 5 years from the date of manufacture, and can be found on the bulk product's immediate container label and/or outer package. However, State pharmacy dispensing laws often require assignment of a shorter expiration date (typically 6 months to 1 year from the date of dispensing) once a drug is dispensed to patients. New programs developed by antiviral drug manufacturers address issues related to shelf-life of these medications.41 Once expired, all products should be disposed of properly (please contact State pharmacy boards or appropriate State authority for regulatory requirements associated with disposal of expired pharmaceutical drugs).
Stockpile Security
A large-scale public health emergency such as a severe pandemic will likely produce widespread anxiety, fear, and possibly panic. By law, pharmacies are required to be constructed to prevent unauthorized access to drugs. For antiviral drugs stored in other on-site licensed facilities, the stockpiling plan should ensure adequate security to protect not only the drugs but also the people who oversee the medications, and the transportation system that delivers them (depending on the quantity stockpiled). An employer planning to stockpile antivirals in an on-site licensed pharmacy or other healthcare facility may want to conduct a security risk assessment of the areas occupied by and adjacent to the licensed pharmacy or other healthcare facility to determine additional security needs. Additional security may be needed to facilitate movement of drugs from one location to another and to protect personnel, if needed, when drugs are dispensed. Financial and personnel resources should be identified to reduce risks to stockpiled assets, personnel, and general operations.
Education and information for employees and families
Employers that choose to stockpile and distribute antiviral medications should work with healthcare providers and/or occupational health services to include an education component as an important part of their antiviral drug program. Providing education and information will assure that the medications are used appropriately and the use of the drugs will be safe as possible. Important components of an educational program for employees include information on the proper use of the medication, a description of who should not take the drugs (contraindications), proper storage of the drug, directions for when to start taking the drug, the importance of taking all of the prescribed doses, possible side effects, and advice to seek medical care for serious adverse effects (See Appendix 1 for package insert information). Persons who receive post-exposure prophylaxis should be given clear instructions as to when and where they should seek care for treatment of suspected pandemic influenza. In addition, persons should be given instructions that the medications should not be used for any other illness (e.g., for - self treatment ) or to treat family or friends. Because employer stockpiles will be calibrated to the estimated need, employees should be educated that if they take the medications before the onset of a pandemic, additional medication may not be available to them from the employer stockpile.
Use of antiviral medications in pregnant women and children
Limited information is available on the safety of antiviral drugs in women who are pregnant (FDA pregnancy Category C). At the time of a pandemic, prescribing antivirals to women who are pregnant should be based on the potential assessment of the benefit versus the risk. Oseltamivir is approved for use as treatment and prophylaxis in children >1 year of age. Zanamivir is approved for use as treatment in children aged >7 years and for prophylaxis in children aged >5 years. No influenza antiviral agents are currently approved for use in infants younger than 12 months of age. See Appendix 1 for package insert information about precautions and prescribing guidelines.
Monitoring antiviral drug use and serious adverse reactions
Tracking recipients of antiviral drugs through an employer's stockpile is important to monitor use and ensure coordination with public sector programs. If dispensing is done through a licensed pharmacy, appropriate records of dispensing and patient counseling will be maintained. For those employers that choose to stockpile and distribute antivirals using another licensed healthcare facility, policies, and procedures should be in place to ensure a method of tracking of who receives antivirals and assures that all recipients of antivirals from the employer's stockpile receive education about proper use and potential side effects associated with the medication.
As with all prescription medications, adverse reactions to antivirals may occur. For example, Relenza® is not recommended for persons with underlying airway disease (e.g., chronic obstructive pulmonary disease or asthma) because of the risk of bronchospasm. The package labeling of both Tamiflu® and Relenza® was recently updated to include a precaution based on post-marketing reports (mostly among pediatric patients and mostly from Japan) of self-injury and delirium with the use of these medications in patients with influenza, although the contribution of the drug to these events is not known. Patients experiencing serious adverse events that may be associated with the use of antiviral drugs for prophylaxis and treatment of influenza should seek medical attention and report the incident to FDA, through the MedWatch program. Responsibility for detecting, managing, and reporting serious adverse events should be shared by healthcare provider and public health professionals as well as patients.
top of page
Next Steps
It is essential that U.S. employers be engaged in preparedness and response activities for a pandemic reflecting a shared responsibility with all levels of government, communities, and individuals and families, to protect the health of the workforce and reduce adverse consequences of a pandemic. Successful planning and response require a comprehensive strategy including the application of multiple interventions initiated early and consistently for the duration of the pandemic. Federal Government and States are stockpiling antiviral drugs for use as part of the public health response to a pandemic. Employers should consider whether maintaining an antiviral stockpile or otherwise arranging for antiviral drugs to be available for their employees should be a component of their overall, comprehensive pandemic plan.
top of page
Conclusion
Antiviral strategies may be most useful for employers that have employees who will have frequent exposure to persons with pandemic illness, in critical infrastructure sectors, and those that have overseas locations and operations. Outbreak prophylaxis of front-line healthcare and emergency services workers (fire, law enforcement, and emergency medical services [EMS]) is recommended because of their important role in providing critical healthcare services, preserving health and safety in communities, the lack of surge capacity in these sectors and the importance of reducing absenteeism when demands for services are likely to be increased. Protecting healthcare workers also protects patients by reducing the risk that healthcare workers will transmit infection to those they care for. Employees who occupy business-critical roles for the provision of critical community services may also benefit from antiviral use, especially coupled with other protective interventions such as infection control, social distancing, and other interventions. Strategies ensuring workplace safety may increase worker confidence, protect health, and may discourage unnecessary absenteeism during a pandemic.
This document does not create a requirement; rather, it defines a prudent strategy for employer antiviral drug stockpiling and use that can contribute to a more effective pandemic response. Nonpharmaceutical approaches to protecting workers will have substantial benefit when effectively applied. The Federal Government encourages employers to consider stockpiling antivirals for use during an influenza pandemic as part of a comprehensive approach and if stockpile plans are consistent with their overall pandemic preparedness plan and they have carefully considered the legal, ethical, regulatory, logistical, and economic implications of stockpiling antiviral medications. Employers should coordinate the planning and use of antiviral stockpiles with public health agencies in their communities to assure optimum use that aligns with the public health strategy for that community.
It is recognized that antiviral drug stockpiling and planning effective use of those medications is a significant undertaking. Ongoing dialogue among employers, labor unions, public health agencies, government, and healthcare and occupational health providers is important to address outstanding issues and concerns and to develop templates for employer use for planning antiviral stockpiling. This guidance document was developed based on the best available information to date; it should be considered - interim- and will be revised, as needed, as new scientific and technological advances are made, as pandemic plans evolve, and as lessons are learned through tabletop and field exercises. Although the challenges of pandemic planning are formidable, our best chances of protecting health and maintaining community functioning during a pandemic rely on a coordinated response between public sector and private sector partners.
top of page
Appendix 1 Information about the use of antiviral drugs, approved indications, and potential impacts
Tamiflu ® (oseltamivir) and Relenza ® (zanamivir) will likely be the antiviral medications used if antiviral treatment of pandemic influenza is indicated.
Contact Information for State Departments of Public Health http://www.pandemicflu.gov/plan/states/statecontacts.html
Contact for State Boards of Pharmacy in the United States
http://www.nabp.net/index.html?target=/whoweare/boards3.asp&
For more information about planning for pandemic influenza, please see: www.pandemicflu.gov
Appendix 2
top of page
Additional References
Balicer RD, Huerta M, Davidovitch N, Grotto I. Cost-benefit of stockpiling drugs for influenza pandemic. Emerg Infect Dis. 2005 Aug;11(8):1280-2.
CDC. ACIP Provisional Recommendations for the Prevention and Control of Influenza. posted March 25, 2008. http://www.cdc.gov/vaccines/recs/provisional/downloads/flu-3-21-08-508.pdf
CDC. Recommendations for Using Antiviral Agents for Influenza for the 2007-08 Influenza Season. http://www.cdc.gov/flu/professionals/antivirals/agents.htm
Halloran ME, Hayden FG, Yang Y, Longini IM, Jr., Monto AS. Antiviral Effects on Influenza Viral Transmission and Pathogenicity: Observations from Household-based Trials. Am J Epidemiol. 2007 Jan 15;165(2):212-21.
Halloran ME, Ferguson NM, Eubank S, Longini IM Jr, Cummings DA, Lewis B, Xu S, Fraser C, Vullikanti A, Germann TC, Wagener D, Beckman R, Kadau K, Barrett C, Macken CA, Burke DS, Cooley P. Modeling targeted layered containment of an influenza pandemic in the United States. Proc Natl Acad Sci U S A. 2008 Mar 25;105(12):4639-44. Epub 2008 Mar 10.
Hayden FG, Gubareva LV, Monto AS, Klein TC, Elliot MJ, Hammond JM, et al. Inhaled zanamivir for the prevention of influenza in families. Zanamivir Family Study Group. N Engl J Med. 2000 Nov 2;343(18):1282-9.
Hayden FG, Belshe R, Villanueva C, Lanno R, Hughes C, Small I, et al. Management of influenza in households: a prospective, randomized comparison of oseltamivir treatment with or without postexposure prophylaxis. J Infect Dis. 2004 Feb 1;189(3):440-9.
Hayden FG, Pavia AT. Antiviral management of seasonal and pandemic influenza. J Infect Dis. 2006 Nov 1;194 Suppl 2:S119-26.
Lipsitch M, Cohen T, Murray M, et al. Antiviral resistance and the control of pandemic influenza. PLoS Medicine. 2007;4:e15.
Monto AS, Pichichero ME, Blanckenberg SJ, Ruuskanen O, Cooper C, Fleming DM, et al. Zanamivir prophylaxis: an effective strategy for the prevention of influenza types A and B within households. J Infect Dis. 2002 Dec 1;186(11):1582-8.
Monto, AS. Vaccines and antiviral drugs in pandemic preparedness. Emerg Infect Dis. 2006 Jan;12(1):55-60.
U.S. Homeland Security Council. National Strategy for Pandemic Influenza. 2005; Available from: www.whitehouse.gov/homeland/nspi.pdf
Aoki, Macleod, Paggiaro ,Carewicz et al. Early administration of oral oseltamivir increases the benefits of influenza treatment. Journal of Antimicrobial Chemotherapy 2003 51, 123-129
Kaiser L, Wat C, Mills T, Mahoney P, Ward P, Hayden F. Impact of oseltamivir treatment on influenza-related lower respiratory tract complications and hospitalizations. Arch Intern Med 2003 July 28;163(14): 1667- “1672.
Hurt AC,, Selleck P, Komadina N, et. al. Susceptibility of highly pathogenic A (H5N1) avian influenza viruses to the neuraminidase inhibitors and adamantanes. Antiviral Res. 2007 Mar;73(3):228-31. Epub 2006 Nov 10.
Govorkova, E , Ilyushina, NA, Boltz, DA, et. al Efficacy of Oseltamivir Therapy in Ferrets Inoculated with Different Clades of H5N1 Influenza Virus, Antimicrobial Agents and Chemotherapy (2007) 51:4, 1414-1424.
Hayden FG, Gubareva LV, Monto AS, Klein TC, Elliot MJ, Hammond JM, et al. Inhaled zanamivir for the prevention of influenza in families. Zanamivir Family Study Group. N Engl J Med. 2000 Nov 2;343(18):1282-9.
Welliver R, Monto AS, Carewicz O, Schatteman E, Hassman M, Hedrick J, et al. Effectiveness of oseltamivir in preventing influenza in household contacts: a randomized controlled trial. JAMA. 2001 Feb 14;285(6):748-54.
Longini IM, Jr., Halloran ME, Nizam A, Yang Y. Containing pandemic influenza with antiviral agents. Am J Epidemiol. 2004 Apr 1;159(7):623-33.
Institute of Medicine; Committee on Modeling Community Containment for Pandemic Influenza. Modeling Community Containment for Pandemic Influenza. A Letter Report. Washington D.C.: The National Academies Press; 2006. p.25.
If employers are choosing which employees may receive antivirals, they should do so pursuant to a company policy and this policy should be applied in a nondiscriminatory manner. Under federal law, employers must not discriminate on the basis of race, sex, age (40 years and over), color, religion, national origin, disability, or veteran status. Disability discrimination include making disability-related inquiries or requiring medical examinations under circumstances prohibited by the Americans with Disabilities Act (ADA), and also includes not holding medical information confidentially. The ADA, however, does permit disability-related inquiries or medical examinations in limited circumstances. First, after making a job offer, but before employment begins, an employer may ask all individuals whether they can take antivirals. Second, an employer may periodically survey all of its current employees to ask if they can safely take antivirals, as long as the employer makes it clear that self-identification is voluntary and explains the purpose for requesting the information. Finally, whether an employer periodically surveys all employees or not, it may ask certain employees with known disabilities that are linked with adverse reactions to antivirals, whether they can take a particular anti-viral. For an analogous discussion regarding emergency evacuations, see Fact Sheet on Obtaining and Using Employee Medical Information as Part of Emergency Evacuation Procedures, http://www.eeoc.gov/facts/evacuation.html. See generally: EEOC. Disability-related Inquiries and Medical Examinations of Employees under the Americans with Disabilities Act, http://www.eeoc.gov/policy/docs/guidance-inquiries.html.
The package insert for each antiviral drug should be consulted for the duration of prophylaxis for which efficacy and safety data are available. Any additional safety issues that might arise with increased duration of exposure cannot be predicted with confidence in the absence of longer-term data. If changes in drug regimens are considered that might warrant use of an Investigational New Drug application or an Emergency Use Authorization during an emergency declared by the Secretary justifying such use, FDA should be contacted as far in advance as possible to discuss regulatory needs and recommendations.
Federal law requires labels on dispensed prescription drugs to include the following minimum information for the drug to be exempt from numerous other labeling requirements: the name and address of the dispenser, the serial number of the medication, date of the prescription or of its filling, the name of the prescriber, the name of the patient (if stated in the prescription), the directions for use and cautionary statements, if any, contained in the prescription. See 21 U.S.C. § 353(b)(2) for more information http://www.fda.gov/opacom/laws/fdcact/fdcact5a.htm.
Committee on Infectious Diseases, American Academy of Pediatrics. Antiviral Therapy and Prophylaxis for Influenza in Children. Pediatrics 2007 April Vol.119(4), 852-860.







