About This Booklet
What Is Leukemia?
Types of Leukemia
Risk Factors
Symptoms
Diagnosis
Treatment
Second Opinion
Supportive Care
Nutrition and Physical Activity
Follow-up Care
Sources of Support
Taking Part in Cancer Research
National Cancer Institute Information Resources
National Cancer Institute Publications
About This Booklet
This National Cancer Institute (NCI) booklet (NIH Publication No. 08-3775) is
about leukemia,* cancer that starts in the tissue that
forms blood. Each year in the United States, more than
40,800 adults and 3,500 children learn they have this
disease.
Learning about medical care for leukemia can help
you take an active part in making choices about your
care. This booklet tells about:
- Diagnosis
- Treatment options
- Supportive care you may need before, during, or
after treatment
- Tests the doctor may give you during follow-up
visits
- Taking part in research studies
This booklet has lists of questions that you may
want to ask your doctor. Many people find it helpful to
take a list of questions to a doctor visit. To help
remember what your doctor says, you can take notes or
ask whether you may use a tape recorder. You may also
want to have a family member or friend go with you
when you talk with the doctor - to take notes, ask
questions, or just to listen.
For the latest information about leukemia, please
visit our Web site at http://www.cancer.gov/cancertopics/types/leukemia. We have materials
on adult and childhood leukemia. Or, contact our
Cancer Information Service. We can answer your
questions about cancer. We can also send you NCI
booklets and fact sheets. Call 1-800-4-CANCER
(1-800-422-6237) or instant message us through the
LiveHelp 1 service at http://www.cancer.gov/help.
*Words in italics are in the Dictionary 2. The Dictionary
explains these terms. It also shows how to pronounce them.
What Is Leukemia?
Leukemia is cancer that starts in the tissue that
forms blood. To understand cancer, it helps to know
how normal blood cells form.
Most blood cells develop from cells in the bone marrow called stem cells. Bone marrow is the soft
material in the center of most bones.
Stem cells mature into different kinds of blood cells.
Each kind has a special job:
White blood cells, red blood cells, and platelets are
made from stem cells as the body needs them. When
cells grow old or get damaged, they die, and new cells
take their place.
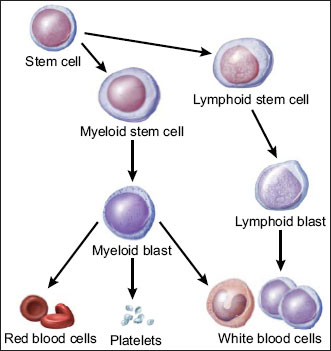
The picture below shows how stem cells can mature
into different types of white blood cells. First, a stem
cell matures into either a myeloid stem cell or a
lymphoid stem cell:
- A myeloid stem cell matures into a myeloid blast.
The blast can form a red blood cell, platelets, or one
of several types of white blood cells.
- A lymphoid stem cell matures into a lymphoid blast.
The blast can form one of several types of white
blood cells, such as B cells or T cells.
The white blood cells that form from myeloid blasts
are different from the white blood cells that form from
lymphoid blasts.
|
| Picture of blood cells maturing from stem cells. |
Most blood cells mature in the bone marrow and
then move into the blood vessels. Blood flowing
through the blood vessels and heart is called the
peripheral blood.
In a person with leukemia, the bone marrow makes
abnormal white blood cells. The abnormal cells are
leukemia cells.
Unlike normal blood cells, leukemia cells don't die
when they should. They may crowd out normal white
blood cells, red blood cells, and platelets. This makes it
hard for normal blood cells to do their work.
Types of Leukemia
The types of leukemia can be grouped based on how
quickly the disease develops and gets worse. Leukemia
is either chronic (which usually gets worse slowly) or
acute (which usually gets worse quickly):
- Chronic leukemia: Early in the disease, the
leukemia cells can still do some of the work of
normal white blood cells. People may not have any
symptoms at first. Doctors often find chronic
leukemia during a routine checkup - before there are
any symptoms.
Slowly, chronic leukemia gets worse. As the number
of leukemia cells in the blood increases, people get
symptoms, such as swollen lymph nodes or
infections. When symptoms do appear, they are
usually mild at first and get worse gradually.
- Acute leukemia: The leukemia cells can't do any of
the work of normal white blood cells. The number
of leukemia cells increases rapidly. Acute leukemia
usually worsens quickly.
The types of leukemia also can be grouped based on
the type of white blood cell that is affected. Leukemia
can start in lymphoid cells or myeloid cells. See the
picture of these cells 3. Leukemia that affects
lymphoid cells is called lymphoid, lymphocytic, or
lymphoblastic leukemia. Leukemia that affects myeloid
cells is called myeloid, myelogenous, or myeloblastic
leukemia.
There are four common types of leukemia:
- Chronic lymphocytic leukemia (CLL): CLL affects
lymphoid cells and usually grows slowly. It accounts
for more than 15,000 new cases of leukemia each
year. Most often, people diagnosed with the disease
are over age 55. It almost never affects children.
- Chronic myeloid leukemia (CML): CML affects
myeloid cells and usually grows slowly at first. It
accounts for nearly 5,000 new cases of leukemia
each year. It mainly affects adults.
- Acute lymphocytic (lymphoblastic) leukemia
(ALL): ALL affects lymphoid cells and grows
quickly. It accounts for more than 5,000 new cases
of leukemia each year. ALL is the most common
type of leukemia in young children. It also affects
adults.
- Acute myeloid leukemia (AML): AML affects
myeloid cells and grows quickly. It accounts for
more than 13,000 new cases of leukemia each year.
It occurs in both adults and children.
Hairy cell leukemia is a rare type of chronic
leukemia. This booklet is not about hairy cell leukemia
or other rare types of leukemia. Together, these rare
leukemias account for fewer than 6,000 new cases of
leukemia each year. The Cancer Information Service
(1-800-4-CANCER) can provide information about
rare types of leukemia.
Risk Factors
When you're told that you have cancer, it's natural
to wonder what may have caused the disease. No one
knows the exact causes of leukemia. Doctors seldom
know why one person gets leukemia and another
doesn't. However, research shows that certain risk factors increase the chance that a person will get this
disease.
The risk factors may be different for the different
types of leukemia:
- Radiation: People exposed to very high levels of
radiation are much more likely than others to get
acute myeloid leukemia, chronic myeloid leukemia,
or acute lymphocytic leukemia.
- Atomic bomb explosions: Very high levels of
radiation have been caused by atomic bomb
explosions (such as those in Japan during World
War II). People, especially children, who survive
atomic bomb explosions are at increased risk of
leukemia.
- Radiation therapy: Another source of exposure to
high levels of radiation is medical treatment for
cancer and other conditions. Radiation therapy
can increase the risk of leukemia.
- Diagnostic x-rays: Dental x-rays and other
diagnostic x-rays (such as CT scans) expose
people to much lower levels of radiation. It's not
known yet whether this low level of radiation to
children or adults is linked to leukemia.
Researchers are studying whether having many
x-rays may increase the risk of leukemia. They
are also studying whether CT scans during
childhood are linked with increased risk of
developing leukemia.
- Smoking: Smoking cigarettes increases the risk of
acute myeloid leukemia.
- Benzene: Exposure to benzene in the workplace can
cause acute myeloid leukemia. It may also cause
chronic myeloid leukemia or acute lymphocytic
leukemia. Benzene is used widely in the chemical
industry. It's also found in cigarette smoke and
gasoline.
- Chemotherapy: Cancer patients treated with certain
types of cancer-fighting drugs sometimes later get
acute myeloid leukemia or acute lymphocytic
leukemia. For example, being treated with drugs
known as alkylating agents or
topoisomerase inhibitors is linked with a small chance of later
developing acute leukemia.
- Down syndrome and certain other inherited
diseases: Down syndrome and certain other
inherited diseases increase the risk of developing
acute leukemia.
- Myelodysplastic syndrome and certain other blood
disorders: People with certain blood disorders are at
increased risk of acute myeloid leukemia.
- Human T-cell leukemia virus type I (HTLV-I):
People with HTLV-I infection are at increased risk
of a rare type of leukemia known as adult T-cell
leukemia. Although the HTLV-I virus may cause
this rare disease, adult T-cell leukemia and other
types of leukemia are not contagious.
- Family history of leukemia: It's rare for more than
one person in a family to have leukemia. When it
does happen, it's most likely to involve chronic
lymphocytic leukemia. However, only a few people
with chronic lymphocytic leukemia have a father,
mother, brother, sister, or child who also has the
disease.
Having one or more risk factors does not mean that
a person will get leukemia. Most people who have risk
factors never develop the disease.
Symptoms
Like all blood cells, leukemia cells travel through
the body. The symptoms of leukemia depend on the
number of leukemia cells and where these cells collect
in the body.
People with chronic leukemia may not have
symptoms. The doctor may find the disease during a
routine blood test.
People with acute leukemia usually go to their
doctor because they feel sick. If the brain is affected,
they may have headaches, vomiting, confusion, loss of
muscle control, or seizures. Leukemia also can affect
other parts of the body such as the digestive tract,
kidneys, lungs, heart, or testes.
Common symptoms of chronic or acute leukemia
may include:
- Swollen lymph nodes that usually don't hurt
(especially lymph nodes in the neck or armpit)
- Fevers or night sweats
- Frequent infections
- Feeling weak or tired
- Bleeding and bruising easily (bleeding gums,
purplish patches in the skin, or tiny red spots under
the skin)
- Swelling or discomfort in the abdomen (from a
swollen spleen or liver)
- Weight loss for no known reason
- Pain in the bones or joints
Most often, these symptoms are not due to cancer.
An infection or other health problems may also cause
these symptoms. Only a doctor can tell for sure.
Anyone with these symptoms should tell the doctor so
that problems can be diagnosed and treated as early as
possible.
Diagnosis
Doctors sometimes find leukemia after a routine
blood test. If you have symptoms that suggest
leukemia, your doctor will try to find out what's
causing the problems. Your doctor may ask about your
personal and family medical history.
You may have one or more of the following tests:
- Physical exam: Your doctor checks for swollen
lymph nodes, spleen, or liver.
- Blood tests: The lab does a complete blood count to
check the number of white blood cells, red blood
cells, and platelets. Leukemia causes a very high
level of white blood cells. It may also cause low
levels of platelets and hemoglobin, which is found
inside red blood cells.
- Biopsy: Your doctor removes tissue to look for
cancer cells. A biopsy is the only sure way to know
whether leukemia cells are in your bone marrow.
Before the sample is taken, local anesthesia is used
to numb the area. This helps reduce the pain. Your
doctor removes some bone marrow from your
hipbone or another large bone. A pathologist uses a
microscope to check the tissue for leukemia cells.
There are two ways your doctor can obtain bone
marrow. Some people will have both procedures
during the same visit:
- Bone marrow aspiration: The doctor uses a
thick, hollow needle to remove samples of bone
marrow.
- Bone marrow biopsy: The doctor uses a very
thick, hollow needle to remove a small piece of
bone and bone marrow.
The tests that your doctor orders for you depend on
your symptoms and type of leukemia. You may have
other tests:
- Cytogenetics: The lab looks at the chromosomes of
cells from samples of blood, bone marrow, or lymph
nodes. If abnormal chromosomes are found, the test
can show what type of leukemia you have. For
example, people with CML have an abnormal
chromosome called the Philadelphia chromosome.
- Spinal tap: Your doctor may remove some of the
cerebrospinal fluid (the fluid that fills the spaces in
and around the brain and spinal cord). The doctor
uses a long, thin needle to remove fluid from the
lower spine. The procedure takes about 30 minutes
and is performed with local anesthesia. You must lie
flat for several hours afterward to keep from getting
a headache. The lab checks the fluid for leukemia
cells or other signs of problems.
- Chest x-ray: An x-ray can show swollen lymph
nodes or other signs of disease in your chest.
You may want to ask your doctor these
questions before having a bone marrow aspiration
or biopsy:
- Will you remove the sample of bone marrow
from the hip or from another bone?
- Where will I go for this procedure?
- Will I have to do anything to prepare for it?
- How long will it take? Will I be awake?
- Will it hurt? What will you do to prevent or
control the pain?
- Are there any risks? What are the chances of
infection or bleeding after the procedure?
- How long will it take me to recover?
- How soon will I know the results? Who will
explain them to me?
- If I do have leukemia, who will talk to me
about next steps? When?
|
Treatment
People with leukemia have many treatment options.
The options are watchful waiting, chemotherapy,
targeted therapy, biological therapy, radiation therapy,
and stem cell transplant. If your spleen is enlarged,
your doctor may suggest surgery to remove it.
Sometimes a combination of these treatments is used.
The choice of treatment depends mainly on the
following:
- The type of leukemia (acute or chronic)
- Your age
- Whether leukemia cells were found in your
cerebrospinal fluid
It also may depend on certain features of the
leukemia cells. Your doctor also considers your
symptoms and general health.
People with acute leukemia need to be treated right
away. The goal of treatment is to destroy signs of
leukemia in the body and make symptoms go away.
This is called a remission. After people go into
remission, more therapy may be given to prevent a
relapse. This type of therapy is called consolidation therapy or maintenance therapy. Many people with
acute leukemia can be cured.
If you have chronic leukemia without symptoms,
you may not need cancer treatment right away. Your
doctor will watch your health closely so that treatment
can start when you begin to have symptoms. Not
getting cancer treatment right away is called watchful
waiting.
When treatment for chronic leukemia is needed, it
can often control the disease and its symptoms. People
may receive maintenance therapy to help keep the
cancer in remission, but chronic leukemia can seldom
be cured with chemotherapy. However, stem cell
transplants offer some people with chronic leukemia
the chance for cure.
Your doctor can describe your treatment choices, the
expected results, and the possible side effects. You and
your doctor can work together to develop a treatment
plan that meets your medical and personal needs.
You may want to talk with your doctor about taking
part in a clinical trial, a research study of new
treatment methods. See the Taking Part in Cancer
Research 4 section.
Your doctor may refer you to a specialist, or you
may ask for a referral. Specialists who treat leukemia
include hematologists, medical oncologists, and
radiation oncologists. Pediatric oncologists and
hematologists treat childhood leukemia. Your health
care team may also include an oncology nurse and a
registered dietitian.
Whenever possible, people should be treated at a
medical center that has doctors experienced in treating
leukemia. If this isn't possible, your doctor may
discuss the treatment plan with a specialist at such a
center.
Before treatment starts, ask your health care team to
explain possible side effects and how treatment may
change your normal activities. Because cancer
treatments often damage healthy cells and tissues, side
effects are common. Side effects may not be the same
for each person, and they may change from one
treatment session to the next.
You may want to ask your doctor these
questions before you begin treatment:
- What type of leukemia do I have? How do I
get a copy of the report from the pathologist?
- What are my treatment choices? Which do you
recommend for me? Why?
- Will I have more than one kind of treatment?
How will my treatment change over time?
- What are the expected benefits of each kind of
treatment?
- What are the risks and possible side effects of
each treatment? What can we do to control the
side effects?
- What can I do to prepare for treatment?
- Will I need to stay in the hospital? If so, for
how long?
- What is the treatment likely to cost? Will my
insurance cover the cost?
- How will treatment affect my normal
activities?
- Would a clinical trial be right for me? Can you
help me find one?
- How often should I have checkups?
|
People with chronic lymphocytic leukemia who do
not have symptoms may be able to put off having
cancer treatment. By delaying treatment, they can
avoid the side effects of treatment until they have
symptoms.
If you and your doctor agree that watchful waiting is
a good idea, you'll have regular checkups (such as
every 3 months). You can start treatment if symptoms
occur.
Although watchful waiting avoids or delays the side
effects of cancer treatment, this choice has risks. It may
reduce the chance to control leukemia before it gets
worse.
You may decide against watchful waiting if you
don't want to live with an untreated leukemia. Some
people choose to treat the cancer right away.
If you choose watchful waiting but grow concerned
later, you should discuss your feelings with your
doctor. A different approach is nearly always available.
You may want to ask your doctor these
questions before choosing watchful waiting:
- If I choose watchful waiting, can I change my
mind later on?
- Will the leukemia be harder to treat later?
- How often will I have checkups?
- Between checkups, what problems should I
report?
|
Many people with leukemia are treated with
chemotherapy. Chemotherapy uses drugs to destroy
leukemia cells.
Depending on the type of leukemia, you may
receive a single drug or a combination of two or more
drugs.
You may receive chemotherapy in several different
ways:
- By mouth: Some drugs are pills that you can
swallow.
- Into a vein (IV): The drug is given through a needle
or tube inserted into a vein.
- Through a catheter (a thin, flexible tube): The tube
is placed in a large vein, often in the upper chest. A
tube that stays in place is useful for patients who
need many IV treatments. The health care
professional injects drugs into the catheter, rather
than directly into a vein. This method avoids the
need for many injections, which can cause
discomfort and injure the veins and skin.
- Into the cerebrospinal fluid: If the pathologist
finds leukemia cells in the fluid that fills the spaces
in and around the brain and spinal cord, the doctor
may order intrathecal chemotherapy. The doctor
injects drugs directly into the cerebrospinal fluid.
Intrathecal chemotherapy is given in two ways:
- Into the spinal fluid: The doctor injects the
drugs into the spinal fluid.
- Under the scalp: Children and some adult
patients receive chemotherapy through a special
catheter called an Ommaya reservoir. The doctor
places the catheter under the scalp. The doctor
injects the drugs into the catheter. This method
avoids the pain of injections into the spinal fluid.
Intrathecal chemotherapy is used because many
drugs given by IV or taken by mouth can't pass
through the tightly packed blood vessel walls found
in the brain and spinal cord. This network of blood
vessels is known as the blood-brain barrier.
Chemotherapy is usually given in cycles. Each cycle
has a treatment period followed by a rest period.
You may have your treatment in a clinic, at the
doctor's office, or at home. Some people may need to
stay in the hospital for treatment.
The side effects depend mainly on which drugs are
given and how much. Chemotherapy kills fast-growing
leukemia cells, but the drug can also harm normal cells
that divide rapidly:
- Blood cells: When chemotherapy lowers the levels
of healthy blood cells, you're more likely to get
infections, bruise or bleed easily, and feel very weak
and tired. You'll get blood tests to check for low
levels of blood cells. If your levels are low, your
health care team may stop the chemotherapy for a
while or reduce the dose of drug. There also are
medicines that can help your body make new blood
cells. Or, you may need a blood transfusion.
- Cells in hair roots: Chemotherapy may cause hair
loss. If you lose your hair, it will grow back, but it
may be somewhat different in color and texture.
- Cells that line the digestive tract: Chemotherapy
can cause poor appetite, nausea and vomiting,
diarrhea, or mouth and lip sores. Ask your health
care team about medicines and other ways to help
you cope with these problems.
- Sperm or egg cells: Some types of chemotherapy
can cause infertility.
- Children: Most children treated for leukemia
appear to have normal fertility when they grow
up. However, depending on the drugs and doses
used and the age of the patient, some boys and
girls may be infertile as adults.
- Adult men: Chemotherapy may damage sperm
cells. Men may stop making sperm. Because
these changes to sperm may be permanent, some
men have their sperm frozen and stored before
treatment (sperm banking).
- Adult women: Chemotherapy may damage the
ovaries. Women may have irregular menstrual
periods or periods may stop altogether. Women
may have symptoms of menopause, such as hot
flashes and vaginal dryness. Women who may
want to get pregnant in the future should ask their
health care team about ways to preserve their
eggs before treatment starts.
You may find it helpful to read NCI's booklet
Chemotherapy and You 5.
People with chronic myeloid leukemia and some
with acute lymphoblastic leukemia may receive drugs
called targeted therapy. Imatinib (Gleevec) tablets were
the first targeted therapy approved for chronic myeloid
leukemia. Other targeted therapy drugs are now used
too.
Targeted therapies use drugs that block the growth of
leukemia cells. For example, a targeted therapy may
block the action of an abnormal protein that stimulates
the growth of leukemia cells.
Side effects include swelling, bloating, and sudden
weight gain. Targeted therapy can also cause anemia,
nausea, vomiting, diarrhea, muscle cramps, or a rash.
Your health care team will monitor you for signs of
problems.
You may want to read the NCI fact sheet Targeted Cancer Therapies: Questions and Answers.
Some people with leukemia receive drugs called
biological therapy. Biological therapy for leukemia is
treatment that improves the body's natural defenses
against the disease.
One type of biological therapy is a substance called a
monoclonal antibody. It's given by IV infusion. This
substance binds to the leukemia cells. One kind of
monoclonal antibody carries a toxin that kills the
leukemia cells. Another kind helps the immune system
destroy leukemia cells.
For some people with chronic myeloid leukemia, the
biological therapy is a drug called interferon. It is
injected under the skin or into a muscle. It can slow the
growth of leukemia cells.
You may have your treatment in a clinic, at the
doctor's office, or in the hospital. Other drugs may be
given at the same time to prevent side effects.
The side effects of biological therapy differ with the
types of substances used, and from person to person.
Biological therapies commonly cause a rash or swelling
where the drug is injected. They also may cause a headache, muscle aches, a fever, or weakness. Your
health care team may check your blood for signs of
anemia and other problems.
You may find it helpful to read NCI's booklet
Biological Therapy 7.
You may want to ask your doctor these
questions before having chemotherapy, targeted
therapy, or biological therapy:
- Which drugs will I get? What will the
treatment do?
- Should I see my dentist before treatment
begins?
- When will treatment start? When will it end?
How often will I have treatments?
- Where will I go for treatment? Will I have to
stay in the hospital?
- What can I do to take care of myself during
treatment?
- How will we know the treatment is working?
- Will I have side effects during treatment? What
side effects should I tell you about? Can I
prevent or treat any of these side effects?
- Can these drugs cause side effects later on?
- How often will I need checkups?
|
Radiation therapy (also called radiotherapy) uses
high-energy rays to kill leukemia cells. People receive
radiation therapy at a hospital or clinic.
Some people receive radiation from a large machine
that is aimed at the spleen, the brain, or other parts of
the body where leukemia cells have collected. This
type of therapy takes place 5 days a week for several
weeks. Others may receive radiation that is directed to
the whole body. The radiation treatments are given
once or twice a day for a few days, usually before a
stem cell transplant.
The side effects of radiation therapy depend mainly
on the dose of radiation and the part of the body that is
treated. For example, radiation to your abdomen can
cause nausea, vomiting, and diarrhea. In addition, your
skin in the area being treated may become red, dry, and
tender. You also may lose your hair in the treated area.
You are likely to be very tired during radiation
therapy, especially after several weeks of treatment.
Resting is important, but doctors usually advise
patients to try to stay as active as they can.
Although the side effects of radiation therapy can be
distressing, they can usually be treated or controlled.
You can talk with your doctor about ways to ease these
problems.
It may also help to know that, in most cases, the
side effects are not permanent. However, you may
want to discuss with your doctor the possible long-term
effects of radiation treatment.
You may find it helpful to read NCI's booklet
Radiation Therapy and You 8.
You may want to ask your doctor these
questions before having radiation therapy:
- Why do I need this treatment?
- When will the treatments begin? How often
will they be given? When will they end?
- How will I feel during treatment? Will I be
able to continue my normal activities during
treatment?
- Will there be side effects? How long will they
last?
- Can radiation therapy cause side effects later
on?
- What can I do to take care of myself during
treatment?
- How will we know if the radiation treatment is
working?
- How often will I need checkups?
|
Some people with leukemia receive a stem cell
transplant. A stem cell transplant allows you to be
treated with high doses of drugs, radiation, or both.
The high doses destroy both leukemia cells and normal
blood cells in the bone marrow. After you receive highdose
chemotherapy, radiation therapy, or both, you
receive healthy stem cells through a large vein. (It's
like getting a blood transfusion.) New blood cells
develop from the transplanted stem cells. The new
blood cells replace the ones that were destroyed by
treatment.
Stem cell transplants take place in the hospital. Stem
cells may come from you or from someone who
donates their stem cells to you:
- From you: An autologous stem cell transplant uses
your own stem cells. Before you get the high-dose
chemotherapy or radiation therapy, your stem cells
are removed. The cells may be treated to kill any
leukemia cells present. Your stem cells are frozen
and stored. After you receive high-dose
chemotherapy or radiation therapy, the stored stem
cells are thawed and returned to you.
- From a family member or other donor: An
allogeneic stem cell transplant uses healthy stem
cells from a donor. Your brother, sister, or parent
may be the donor. Sometimes the stem cells come
from a donor who isn't related. Doctors use blood
tests to learn how closely a donor's cells match your
cells.
- From your identical twin: If you have an identical
twin, a syngeneic stem cell transplant uses stem
cells from your healthy twin.
Stem cells come from a few sources. The stem cells
usually come from the blood (peripheral stem cell transplant). Or they can come from the bone marrow
(bone marrow transplant). Another source of stem cells
is umbilical cord blood. Cord blood is taken from a
newborn baby and stored in a freezer. When a person
gets cord blood, it's called an umbilical cord blood transplant.
After a stem cell transplant, you may stay in the
hospital for several weeks or months. You'll be at risk
for infections and bleeding because of the large doses
of chemotherapy or radiation you received. In time, the
transplanted stem cells will begin to produce healthy
blood cells.
Another problem is that graft-versus-host disease
(GVHD) may occur in people who receive donated
stem cells. In GVHD, the donated white blood cells in
the stem cell graft react against the patient's normal
tissues. Most often, the liver, skin, or digestive tract is
affected. GVHD can be mild or very severe. It can
occur any time after the transplant, even years later.
Steroids or other drugs may help.
You may find it helpful to read NCI's fact sheet
Bone Marrow Transplantation and Peripheral Blood
Stem Cell Transplantation: Questions and Answers 9.
You may want to ask your doctor these
questions before having a stem cell transplant:
- What kind of stem cell transplant will I have?
If I need a donor, how will we find one?
- How long will I be in the hospital? Will I need
special care? How will I be protected from
germs? Will my visitors have to wear a mask?
Will I?
- What care will I need when I leave the
hospital?
- How will we know if the treatment is working?
- What are the risks and the side effects? What
can we do about them?
- What changes in normal activities will be
necessary?
- What is my chance of a full recovery? How
long will that take?
- How often will I need checkups?
|
Second Opinion
Before starting treatment, you might want a second
opinion about your diagnosis and treatment plan. Some
people worry that the doctor will be offended if they
ask for a second opinion. Usually the opposite is true.
Most doctors welcome a second opinion. And many
health insurance companies will pay for a second
opinion if you or your doctor requests it.
If you get a second opinion, the doctor may agree
with your first doctor's diagnosis and treatment plan.
Or the second doctor may suggest another approach.
Either way, you have more information and perhaps a
greater sense of control. You can feel more confident
about the decisions you make, knowing that you've
looked at your options.
It may take some time and effort to gather your
medical records and see another doctor. In most cases,
it's not a problem to take several weeks to get a second
opinion. The delay in starting treatment usually won't
make treatment less effective. To make sure, you
should discuss this delay with your doctor. Some
people with leukemia need treatment right away.
There are many ways to find a doctor for a second
opinion. You can ask your doctor, a local or state
medical society, a nearby hospital, or a medical school
for names of specialists. NCI's Cancer Information
Service at 1-800-4-CANCER can tell you about
nearby treatment centers. Other sources can be found
in NCI's fact sheet How To Find a Doctor or
Treatment Facility If You Have Cancer 10.
Nonprofit groups with an interest in leukemia may
be of help. Many such groups are listed in the NCI fact
sheet National Organizations That Offer Services to
People With Cancer and Their Families 11.
Supportive Care
Leukemia and its treatment can lead to other health
problems. You can have supportive care before, during,
or after cancer treatment.
Supportive care is treatment to prevent or fight
infections, to control pain and other symptoms, to
relieve the side effects of therapy, and to help you cope
with the feelings that a diagnosis of cancer can bring.
You may receive supportive care to prevent or control
these problems and to improve your comfort and
quality of life during treatment.
- Infections: Because people with leukemia get
infections very easily, you may receive antibiotics
and other drugs. Some people receive vaccines
against the flu and pneumonia. The health care team
may advise you to stay away from crowds and from
people with colds and other contagious diseases. If
an infection develops, it can be serious and should
be treated promptly. You may need to stay in the
hospital for treatment.
- Anemia and bleeding: Anemia and bleeding are
other problems that often require supportive care.
You may need a transfusion of red blood cells or
platelets. Transfusions help treat anemia and reduce
the risk of serious bleeding.
- Dental problems: Leukemia and chemotherapy can
make the mouth sensitive, easily infected, and likely
to bleed. Doctors often advise patients to have a
complete dental exam and, if possible, undergo
needed dental care before chemotherapy begins.
Dentists show patients how to keep their mouth
clean and healthy during treatment.
You can get information about supportive care on
NCI's Web site at http://www.cancer.gov/cancerinfo/coping and from NCI's Cancer Information
Service at 1-800-4-CANCER or
LiveHelp 1
(http://www.cancer.gov/help).
Nutrition and Physical Activity
It's important for you to take care of yourself by
eating well and staying as active as you can.
You need the right amount of calories to maintain a
good weight. You also need enough protein to keep up
your strength. Eating well may help you feel better and
have more energy.
Sometimes, especially during or soon after
treatment, you may not feel like eating. You may be
uncomfortable or tired. You may find that foods do not
taste as good as they used to. In addition, the side
effects of treatment (such as poor appetite, nausea,
vomiting, or mouth sores) can make it hard to eat well.
Your doctor, a registered dietitian, or another health
care provider can suggest ways to deal with these
problems. Also, the NCI booklet Eating Hints for
Cancer Patients 12 has many useful ideas and recipes.
Research shows that people with cancer feel better
when they are active. Walking, yoga, and other
activities can keep you strong and increase your
energy. Exercise may reduce nausea and pain and make
treatment easier to handle. It also can help relieve
stress. Whatever physical activity you choose, be sure
to talk to your doctor before you start. Also, if your
activity causes you pain or other problems, be sure to
let your doctor or nurse know about it.
Follow-up Care
You'll need regular checkups after treatment for
leukemia. Checkups help ensure that any changes in
your health are noted and treated if needed. If you have
any health problems between checkups, you should
contact your doctor.
Your doctor will check for return of the cancer. Even
when the cancer seems to be completely destroyed, the
disease sometimes returns because undetected
leukemia cells remained somewhere in your body after
treatment. Also, checkups help detect health problems
that can result from cancer treatment.
Checkups may include a careful physical exam,
blood tests, cytogenetics, x-rays, bone marrow
aspiration, or spinal tap.
The NCI has publications to help answer questions
about follow-up care and other concerns. You may find
it helpful to read the NCI booklet Facing Forward:
Life After Cancer Treatment 13. You may also want to
read the NCI fact sheet Follow-up Care After Cancer
Treatment: Questions and Answers 14.
You may want to ask your doctor these
questions after you have finished treatment:
- How often will I need checkups?
- Which follow-up tests do you suggest for me?
- Between checkups, what health problems or
symptoms should I tell you about?
|
Sources of Support
Learning you have leukemia can change your life
and the lives of those close to you. These changes can
be hard to handle. It's normal for you, your family, and
your friends to have new and confusing feelings to
work through.
Concerns about treatments and managing side
effects, hospital stays, and medical bills are common.
You may also worry about caring for your family,
keeping your job, or continuing daily activities.
Here's where you can go for support:
- Doctors, nurses, and other members of your health
care team can answer many of your questions about
treatment, working, or other activities.
- Social workers, counselors, or members of the
clergy can be helpful if you want to talk about your
feelings or concerns. Often, social workers can
suggest resources for financial aid, transportation,
home care, or emotional support.
- Support groups can also help. In these groups,
patients or their family members meet with other
patients or their families to share what they have
learned about coping with the disease and the effects
of treatment. Groups may offer support in person,
over the telephone, or on the Internet. You may want
to talk with a member of your health care team
about finding a support group.
- Information specialists at 1-800-4-CANCER and
at
LiveHelp 1 (http://www.cancer.gov/help) can help
you locate programs, services, and publications.
They can give you names of national organizations
that offer services to people with cancer and their
families.
For tips on coping, you may want to read the NCI
booklet Taking Time: Support for People With Cancer 15.
Taking Part in Cancer Research
Cancer research has led to real progress in leukemia
treatment. Because of research, adults and children
with leukemia can look forward to a better quality of
life and less chance of dying from the disease.
Continuing research offers hope that, in the future,
even more people with this disease will be treated
successfully.
Doctors all over the country are conducting many
types of clinical trials (research studies in which people
volunteer to take part). Clinical trials are designed to
answer important questions and to find out whether
new approaches are safe and effective.
Doctors are studying methods of new and better
ways to treat leukemia, and ways to improve quality of
life. They are testing new targeted therapy, biological
therapy, and chemotherapy. They also are working with
various combinations of treatments.
Even if people in a trial do not benefit directly, they
still make an important contribution by helping doctors
learn more about leukemia and how to control it.
Although clinical trials may pose some risks, doctors
do all they can to protect their patients.
If you are interested in being part of a clinical trial,
talk with your doctor. You may want to read the NCI
booklet Taking Part in Cancer Treatment Research
Studies 16. This booklet describes how treatment studies
are carried out and explains their possible benefits and
risks.
NCI's Web site includes a section on clinical
trials at http://www.cancer.gov/clinicaltrials. It
has general information about clinical trials as well
as detailed information about specific ongoing
studies of leukemia. Information specialists at
1-800-4-CANCER or at
LiveHelp 1 at
http://www.cancer.gov/help can answer questions and
provide information about clinical trials.
National Cancer Institute Information Resources
You may want more information for yourself, your
family, and your doctor. The following NCI services
are available to help you.
NCI's Cancer Information Service (CIS) provides
accurate, up-to-date information about cancer to
patients and their families, health professionals, and the
general public. Information specialists translate the
latest scientific information into plain language, and
they will respond in English or Spanish, as well as
through TRS providers for the hearing or speech
impaired. Calls to the CIS are confidential and free.
|
Telephone:
|
1-800-4-CANCER (1-800-422-6237)
|
NCI's Web site provides information from numerous
NCI sources. It offers current information about cancer
prevention, screening, diagnosis, treatment, genetics,
supportive care, and ongoing clinical trials. It has
information about NCI's research programs, funding
opportunities, and cancer statistics.
If you're unable to find what you need on the Web
site, contact NCI staff. Use the online contact form at
http://www.cancer.gov/contact
or send an email to
cancergovstaff@mail.nih.gov.
Also, information specialists provide live,
online assistance through
LiveHelp 1 at
http://www.cancer.gov/help.
National Cancer Institute Publications
NCI provides publications about cancer, including
the booklets and fact sheets mentioned in this booklet.
Many are available in both English and Spanish.
You may order these publications by telephone, on
the Internet, or by mail. You may also read them online
and print your own copy.
- By telephone: People in the United States and its
territories may order these and other NCI
publications by calling the NCI's Cancer
Information Service at 1-800-4-CANCER.
- On the Internet: Many NCI publications may be
viewed, downloaded, and ordered from
http://www.cancer.gov/publications on the
Internet. People in the United States and its
territories may use this Web site to order printed
copies. This Web site also explains how people
outside the United States can mail or fax their
requests for NCI booklets.
- By mail: NCI publications may be ordered by
writing to the address below:
Publications Ordering Service
National Cancer Institute
P.O. Box 24128
Baltimore, MD 21227
|

