What Are Thalassemias?
Thalassemias (thal-a-SE-me-ahs) are inherited blood
disorders. "Inherited" means they're passed on from parents to children through
genes.
Thalassemias cause the body to make fewer healthy
red blood cells and less hemoglobin (HEE-muh-glow-bin) than normal. Hemoglobin
is an iron-rich protein in red blood cells. It carries oxygen to all parts of
the body. It also carries carbon dioxide (a waste gas) from the body to the
lungs, where it's exhaled.
People who have thalassemias can have mild or severe
anemia
(uh-NEE-me-uh). This condition is caused by a lower than normal number of red
blood cells or not enough hemoglobin in the red blood cells.
Overview
Normal hemoglobin, also called hemoglobin A, has
four protein chains—two alpha globin and two beta globin. The two major
types of thalassemia, alpha and beta, are named after defects in these protein
chains.
Four genes are needed to make enough alpha globin
protein chains. Alpha thalassemia trait occurs when one or two of the four
genes are missing. If more than two genes are missing, the result is moderate
to severe anemia.
The most severe form of alpha thalassemia is known
as alpha thalassemia major or hydrops fetalis. Babies with this disorder
usually die before or shortly after birth.
Two genes (one from each parent) are needed to make
enough beta globin protein chains. Beta thalassemia occurs when one or both
genes are altered.
The severity of beta thalassemia depends on how
badly one or both genes are affected. If both genes are affected, the result is
moderate to severe anemia. The severe form of beta thalassemia also is known as
thalassemia major or Cooley's anemia.
Thalassemias affect both males and females. They
occur most often among people of Italian, Greek, Middle Eastern, Asian, and
African descent. Severe forms usually are diagnosed in early childhood and are
lifelong conditions.
Doctors diagnose thalassemias using
blood
tests. The disorders are treated with
blood
transfusions, medicines, and other procedures.
Outlook
Treatments for thalassemias have improved greatly in
the past few years. People who have moderate and severe thalassemias are now
living longer and have better quality of life than before.
However, complications from thalassemias and their
treatments are frequent. People who have moderate or severe thalassemias must
closely follow their treatment plans. They need to take care of themselves to
remain as healthy as possible.
Other Names for Thalassemias
The various types of thalassemia have specific names
related to the severity of the disorder. (For more information about the types
of thalassemia, see "What Causes
Thalassemias?")
Alpha Thalassemias
- Alpha thalassemia silent carrier
- Alpha thalassemia minor, also called alpha
thalassemia trait
- Hemoglobin H disease
- Alpha thalassemia major, also called hydrops
fetalis
Beta Thalassemias
- Beta thalassemia minor, also called beta
thalassemia trait
- Beta thalassemia intermedia
- Beta thalassemia major, also called Cooley's
anemia or beta-zero (ß0) thalassemia
- Beta-plus (ß+) thalassemia
- Mediterranean anemia
What Causes Thalassemias?
Your body makes three types of blood cells: red
blood cells, white blood cells, and platelets (PLATE-lets). Red blood cells
contain hemoglobin, an iron-rich protein that carries oxygen from your lungs to
all parts of your body. Hemoglobin also carries carbon dioxide (a waste gas)
from your body to your lungs to be exhaled.
Hemoglobin has two kinds of protein
chains: alpha globin and beta globin. If your body doesn't make enough of
these protein chains, red blood cells don't form properly and can't carry
enough oxygen. Your body won't work well if your red blood cells don't make
enough healthy hemoglobin.
Genes control how the body makes hemoglobin protein
chains. When these genes are missing or altered, thalassemias occur.
Thalassemias are inherited disorders. That is,
they're passed on from parents to their children through genes. People who get
abnormal hemoglobin genes from one parent but normal genes from the other are
called carriers. Carriers often have no signs of illness other than mild
anemia.
However, they can pass the abnormal genes on to their children.
People with moderate to severe forms of thalassemia
have inherited abnormal genes from both parents.
Alpha Thalassemias
Four genes (two from each parent) are needed to make
enough alpha globin protein chains. If one or more of the genes is missing, you
will have alpha thalassemia trait or disease. This means that you don't make
enough alpha globin protein.
- If you have only one missing gene, you're a
silent carrier and won't have any signs of illness.
- If you have two missing genes, you have alpha
thalassemia trait (also called alpha thalassemia minor). You may have mild
anemia.
- If you have three missing genes, you likely will
have hemoglobin H disease (which a
blood
test can detect). This form of thalassemia causes moderate to severe
anemia.
Very rarely, a baby will have all four genes
missing. This condition is called alpha thalassemia major or hydrops fetalis.
Babies with hydrops fetalis usually die before or shortly after birth.
Inheritance Pattern for Alpha
Thalassemia
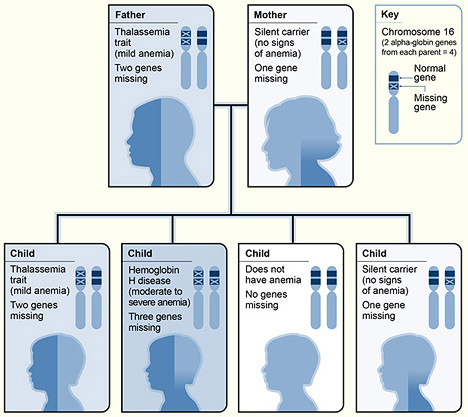
The diagram shows one example of how
alpha thalassemia is inherited. The alpha globin genes are located on
chromosome 16. A child inherits four alpha globin genes—two from each
parent. In this example, the father is missing two alpha globin genes and the
mother is missing one alpha globin gene.
Therefore, each child has a 25
percent chance of inheriting two missing genes and two normal genes
(thalassemia trait), three missing genes and one normal gene (hemoglobin H
disease), four normal genes (no anemia), or one missing gene and three normal
genes (silent carrier).
Beta Thalassemias
Two genes (one from each parent) are needed to make
enough beta globin protein chains. If one or both of these genes are altered,
you will have beta thalassemia. This means that you don't make enough beta
globin protein.
- If you have one altered gene, you're a carrier.
This condition is called beta thalassemia trait or beta thalassemia minor. It
causes mild anemia.
- If both genes are altered, you will have beta
thalassemia intermedia or beta thalassemia major (also called Cooley's anemia).
The intermedia form of the disorder causes moderate anemia. The major form
causes severe anemia.
Inheritance Pattern for Beta
Thalassemia
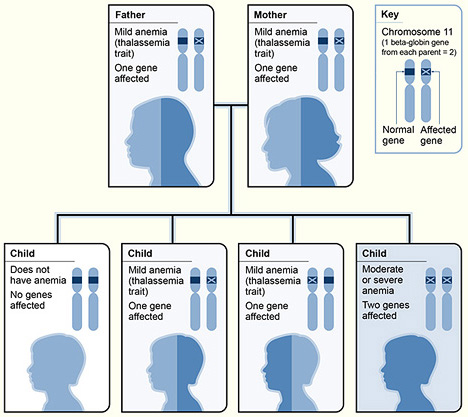
The diagram shows one example of how
beta thalassemia is inherited. The beta globin gene is located on chromosome
11. A child inherits two beta globin genes—one from each parent. In this
example, each parent has one altered beta globin gene.
Therefore, each child has a 25
percent chance of inheriting two normal genes (no anemia), a 50 percent chance
of inheriting one altered gene and one normal gene (beta thalassemia trait), or
a 25 percent chance of inheriting two altered genes (beta thalassemia
major).
Who Is At Risk for Thalassemias?
Family history and ancestry are the two risk factors
for thalassemias.
Family History
Thalassemias are inherited, which means they're
passed on from parents to their children. If your parents have missing or
altered hemoglobin-making genes, you may have a thalassemia.
Ancestry
Alpha thalassemias most often affect people of
Southeast Asian, Indian, Chinese, or Filipino origin or ancestry.
Beta thalassemias most often affect people of
Mediterranean (Greek, Italian, and Middle Eastern), Asian, or African origin or
ancestry.
What Are the Signs and Symptoms of Thalassemias?
Signs and symptoms of thalassemias are due to lack
of oxygen in the bloodstream. This occurs because the body doesn't make enough
healthy red blood cells and hemoglobin. The severity of symptoms depends on the
severity of the disorder.
No Symptoms
Alpha thalassemia silent carriers generally have no
signs or symptoms of the disorder. This is because the lack of alpha globin
protein is so small that hemoglobin works normally.
Mild Anemia
People who have alpha or beta thalassemia trait can
have mild
anemia.
However, many people with this type of thalassemia have no signs or symptoms.
Mild anemia can make you feel tired. It's often
mistaken for
iron-deficiency
anemia.
Mild to Moderate Anemia and Other Signs and
Symptoms
People with beta thalassemia intermedia have mild to
moderate anemia. They also may have other health problems, such as:
- Slowed growth and delayed puberty. Anemia can
slow down a child's growth and development.
- Bone problems. Thalassemia may make bone marrow
(the spongy material inside bones that makes blood cells) expand. This causes
wider bones than normal. Bones also may be brittle and break easily.
- An enlarged spleen. The spleen is an organ that
helps your body fight infection and remove unwanted material. When a person has
a thalassemia, the spleen has to work very hard. As a result, the spleen
becomes larger than normal. This makes anemia worse. If the spleen becomes too
large, it must be removed.
Severe Anemia and Other Signs and Symptoms
People with hemoglobin H disease or beta thalassemia
major (also called Cooley's anemia) have severe thalassemia. Signs and symptoms
occur within the first 2 years of life. They may include severe
anemia and other serious health problems, such as:
- Pale and listless appearance
- Poor appetite
- Dark urine
- Slowed growth and delayed puberty
- Jaundice (a yellowish color of the skin or
whites of the eyes)
- Enlarged spleen, liver, and heart
- Bone problems (especially bones in the
face)
Complications of Thalassemias
Better treatments now allow people who have moderate
and severe thalassemias to live much longer. As a result, these people must
cope with complications of the disorder that occur over time.
Heart and Liver Disease
Regular
blood
transfusions are a standard treatment for thalassemias. (See
"How Are Thalassemias Treated?") As a
result, iron can build up in the blood. This can damage organs and tissues,
especially the heart and liver.
Heart disease caused by iron overload is the main
cause of death in people who have thalassemias. Heart disease includes
heart
failure,
arrhythmias
(irregular heartbeats), and
heart
attack.
Infection
Among people who have thalassemias, infections are a
key cause of illness and the second most common cause of death. People who have
had their spleens removed are at even higher risk, because they no longer have
this infection-fighting organ.
Osteoporosis
Many people who have thalassemias have bone
problems, including osteoporosis (OS-te-o-po-RO-sis). This is a condition in
which bones are weak and brittle and break easily.
How Are Thalassemias Diagnosed?
Doctors diagnose thalassemias using
blood
tests, including a complete blood count (CBC) and special hemoglobin tests.
- A CBC provides information about the amount of
hemoglobin and the different kinds of blood cells, such as red blood cells, in
a sample of blood. People who have thalassemias have fewer healthy red blood
cells and less hemoglobin in their blood than normal. People who have alpha or
beta thalassemia trait may have smaller than normal red blood cells.
- Hemoglobin tests measure the types of hemoglobin
in a blood sample. People who have thalassemias have problems with the alpha or
beta globin protein chains of hemoglobin.
Moderate and severe thalassemias usually are
diagnosed in early childhood. This is because signs and symptoms, including severe
anemia,
appear within the first 2 years of life.
People who have milder forms of thalassemia may be
diagnosed after a routine blood test shows they have anemia. Doctors suspect
thalassemia if a child has anemia and is a member of an ethnic group that's at
increased risk for thalassemia. (See "Who Is At
Risk for Thalassemias?")
Doctors also do tests on the amount of iron in the
blood to find out whether the anemia is due to iron deficiency or thalassemia.
Iron-deficiency
anemia occurs when the body doesn't have enough iron to make hemoglobin.
The anemia in thalassemia occurs because of a problem with either the alpha
globin chain or the beta globin chain of hemoglobin, not because of a lack of
iron.
Because thalassemias are passed on from parents to
children, family genetic studies also can help diagnose the disorder. This
involves taking a family medical history and doing blood tests on family
members to show whether any have missing or altered hemoglobin genes.
If you know of family members who have thalassemias
and you're thinking of having children, consider talking with your doctor
and/or a genetic counselor. They can help determine your risk for passing on
the disorder to a child.
If you're expecting a baby and you and your partner
are thalassemia carriers, you may want to consider prenatal testing.
Prenatal testing involves taking a sample of
amniotic fluid or tissue from the placenta. (Amniotic fluid is the fluid in the
sac surrounding a growing embryo. The placenta is the organ that attaches the
umbilical cord to the mother's womb.) Tests done on the fluid or tissue
can show whether your baby has thalassemia and how severe it's likely to be.
How Are Thalassemias Treated?
Treatments for thalassemias depend on the type and
severity of the disorder. People who are carriers or who have alpha or beta
thalassemia trait have mild or no symptoms. They need little or no treatment.
Doctors use three standard treatments for moderate
and severe forms of thalassemia. These include
blood
transfusions, iron chelation (ke-LAY-shun) therapy, and folic acid
supplements. Other treatments have been developed or are being tested, but
they're used much less often.
Standard Treatments
Blood Transfusions
Transfusions of red blood cells are the main
treatment for people who have moderate or severe thalassemias. A blood
transfusion, given through a needle in a vein, gives you healthy red blood
cells with normal hemoglobin. Red blood cells live for only about 120 days. So,
you may need repeated transfusions to maintain a supply of healthy red blood
cells.
If you have hemoglobin H disease or beta thalassemia
intermedia, you may need blood transfusions on occasion. For example, you may
need this treatment when you have an infection or other illness, or when your
anemia
is severe enough to cause tiredness.
If you have beta thalassemia major, or Cooley's
anemia, you need regular blood transfusions (often every 2 to 4 weeks). These
will help you maintain normal hemoglobin levels and red blood cell numbers.
Blood transfusions allow you to feel better, enjoy normal activities, and live
into adulthood.
Blood transfusions are lifesaving, but they're
expensive and carry a risk of transmitting infections and viruses (for example,
hepatitis). However, this risk is very low in the United States because of
careful blood screening.
Iron Chelation Therapy
Because the hemoglobin in red blood cells is an
iron-rich protein, regular blood transfusions can lead to a buildup of iron in
the blood. This condition is called iron overload. It damages the liver, heart,
and other parts of the body.
To prevent this damage, iron chelation therapy is
needed to remove excess iron from the body. Two medicines are used for iron
chelation therapy.
- Deferoxamine is a liquid medicine that's given
slowly under the skin, usually with a small portable pump used overnight. This
therapy takes time and can be mildly painful. Side effects include loss of
vision and hearing.
- Deferasirox is a pill taken once a day. Side
effects include headache, nausea (feeling sick to the stomach), vomiting,
diarrhea, joint pain, and fatigue (tiredness).
Folic Acid Supplements
Folic acid is a B vitamin that helps build healthy
red blood cells. You may need to take folic acid supplements in addition to
blood transfusions and/or iron chelation therapy.
Other Treatments
Other treatments have been developed or are being
tested, but they're used much less often.
Blood and Marrow Stem Cell Transplant
A
blood
and marrow stem cell transplant replaces your abnormal or faulty stem cells
with healthy ones from another person (a donor). Stem cells are the cells
inside bone marrow that make red blood cells and other types of blood cells.
A stem cell transplant is the only treatment that
can cure thalassemia. But only a small number of people who have the severe
form of the disorder are able to find a good match among donors and have the
risky procedure.
Possible Future Treatments
Researchers are working to find new treatments for
thalassemias. For example, it may be possible someday to insert a normal
hemoglobin gene into stem cells in bone marrow. This will allow people to make
their own healthy red blood cells and hemoglobin.
Researchers also are studying ways to trigger a
person's ability to make fetal hemoglobin after birth. This type of hemoglobin
is found in fetuses and newborns. After birth, the body switches to making
adult hemoglobin. Making more fetal hemoglobin may make up for the lack of
healthy adult hemoglobin.
Treating Complications
Better treatments now allow people who have moderate
and severe thalassemias to live much longer. As a result, these people must
cope with complications that occur over time.
An important part of managing thalassemias is
treating complications. Treatment may be needed for heart or liver diseases,
infections, osteoporosis, and other problems.
Can Thalassemias Be Prevented?
Thalassemias can't be prevented because they're
inherited (passed on from parents to children). However, these bleeding
disorders can be found before birth through prenatal tests.
Family genetic studies may help find out whether
people have missing or altered hemoglobin genes that cause thalassemias. (For
more information, see "How Are
Thalassemias Diagnosed?")
If you know of family members who have thalassemias
and you're thinking of having children, consider talking with your doctor
and/or a genetic counselor. They can help determine your risk for passing on
the disorder to your child.
Living With Thalassemias
Survival and quality of life are now much better for
people who have moderate or severe forms of thalassemia. This is because:
- More people are able to get
blood
transfusions now.
- Blood screening has reduced the number of
infections from blood transfusions. Also, treatments for other kinds of
infections have improved.
- New iron chelation treatments are available that
are easier for some people to take.
- Some people have been cured through
blood
and marrow stem cell transplants.
Living with thalassemia can be challenging, but
several approaches can help you cope.
Follow Your Treatment Plan
It's important to follow the treatment plan your
doctor gives you. Get blood transfusions as he or she recommends.
Take your iron chelation medicine. This is important
because the leading cause of death among people with thalassemias is heart
disease caused by iron overload. Iron buildup can damage your heart, liver, and
other organs. Although the iron chelation treatment can take time and be mildly
painful, it's important that you don't stop taking your medicine.
Several chelation treatments are now available,
including injections and pills. Your doctor will talk to you about which
treatment is best for you.
Take folic acid supplements if your doctor
prescribes them. Folic acid is a B vitamin that helps build healthy red blood
cells.
Get Ongoing Medical Care
It's important that you keep your scheduled medical
appointments and get any tests that your doctor recommends.
These tests may include:
- Monthly complete blood counts, and tests for
blood iron levels every 3 months
- Yearly tests for heart function, liver function,
and viral infection (for example, hepatitis B and C and HIV)
- Yearly tests to check for iron buildup in your
liver
- Yearly vision and hearing tests
- Regular checkups to make sure blood transfusions
are working
- Other tests as needed (such as lung function
tests, genetic tests, and tests to match your tissues against a possible donor
if a stem cell transplant is being considered)
Children who have thalassemias should receive yearly
checkups to monitor their growth and development. The checkup includes a
physical exam, including a height and weight check, and any necessary tests.
Take Measures To Stay Healthy
Take steps to stay as healthy as possible. Follow a
healthy eating plan. Follow your doctor's instructions about taking iron
supplements.
Get vaccinations as needed, especially if you've had
your spleen removed. You may need vaccinations for flu, pneumonia, hepatitis B,
and meningitis. Your doctor can tell you which vaccines you need.
Watch for signs of infections (such as fever) and
take steps to lower your chance of getting an infection. This is especially
important if you've had your spleen removed.
- Wash your hands often.
- Avoid crowds during cold and flu season.
- Keep the skin around the site where you get
blood transfusions as clean as possible.
- Call your doctor if fever develops.
Seek Help and Support
Joining a support group may help you cope with
thalassemia if you or your child has it. Talking to others who live with the
same issues can help you see how they've coped with them. To find a local
support group, contact the
Cooley's Anemia Foundation.
Key Points
- Thalassemias are inherited blood disorders.
"Inherited" means they're passed on from parents to children.
- Thalassemias cause the body to make fewer
healthy red blood cells and less hemoglobin than normal.
- People who have thalassemias can have mild or
severe
anemia.
This condition is caused by a lower than normal number of red blood cells or
not enough hemoglobin in the red blood cells.
- The two major types of thalassemia are alpha
thalassemia and beta thalassemia. There are different forms of each type.
- Thalassemias occur when the genes that control
the production of hemoglobin are missing or altered. Your body won't work
properly if your red blood cells don't make enough healthy hemoglobin.
- Family history and ancestry are the two risk
factors for thalassemias. If your parents have missing or altered
hemoglobin-making genes, you may have thalassemia. Thalassemias occur most
often among people of Italian, Greek, Middle Eastern, Asian, and African
descent.
- Signs and symptoms of thalassemias are due to
lack of oxygen in the bloodstream. They may include mild to severe anemia;
slowed growth and delayed puberty; bone problems; and enlarged spleen, liver,
or heart; a pale and listless appearance; poor appetite; dark urine; and
jaundice (a yellowish color of the skin or whites of the eyes). Symptoms depend
on the type of thalassemia you have. Silent carriers have no symptoms.
- Doctors diagnose thalassemias using
blood
tests, including a complete blood count and special hemoglobin tests.
Prenatal testing can show whether an unborn baby has thalassemia and how severe
it's likely to be.
- People who have mild thalassemia often need
little or no treatment. There are three standard treatments for moderate and
severe forms of thalassemia. These include
blood
transfusions, iron chelation therapy, and folic acid supplements.
- Better treatments now allow people who have
moderate and severe thalassemias to live much longer. As a result, these people
must cope with complications of the disease that develop over time.
Complications include heart and liver disease, infections, osteoporosis, and
other problems.
- Thalassemias can't be prevented because they're
inherited. However, these blood disorders can be found before birth through
prenatal testing.
- Living with thalassemia can be challenging, but
several approaches can help you cope. Follow your doctor's treatment plan, get
ongoing medical care, take measures to stay healthy, and seek help and support.
Links to Other Information About Thalassemias
NHLBI Resources
Non-NHLBI Resources
Clinical Trials
|