No deaths occurred during either study. Chowdhury 2001 found no significant effect of peri-operative thyroid hormone supplementation in neonates on either length of hospital stay or duration of mechanical ventilation. Portman 2000 found no significant difference in dopamine requirements for the treatment versus control groups for the first 24 hours post operatively, while in the Chowdhury neonatal subgroup, inotrope requirements were significantly lower in the treatment group. Portman 2000 reported significant differences between the two groups at 1 and 24 hours post operatively for free T3 and at 1 hour post operatively for total T3 levels. Total T4 levels showed no significant difference between groups, either pre-cardiopulmonary bypass or up to 72 hours post operatively.
Alterations of plasma thyroid hormone concentration in non-thyroidal illness have been postulated to represent an adaptive response of the organism to minimise metabolic demands during the stress of non-thyroidal illness (Utiger 1980). To date, there has been particular interest in the post-operative course of infants undergoing cardiopulmonary bypass procedures for repair of congenital heart defects. Thyroid hormone suppression in infants and children post cardiopulmonary bypass is associated with increased length of mechanical ventilation, intensive care treatment, and requirements of inotropic drugs, vasoactive catecholamines and frusemide (Bettendorf 1997).
There are several proposed mechanisms to explain this phenomenon. Firstly, the surgical procedure itself triggers suppression of the hypothalamic-pituitary thyroid axis (Mainwaring 1994). Secondly, the cardiopulmonary bypass, hypothermia, haemodilution, dopamine infusion (Bettendorf 1997) and probable iodine antiseptic contamination (Brogan 1997) augment the inhibitory effect. Low post operative triiodothyronine concentration after cardiopulmonary bypass may also be triggered by endogenous release of mediators such as glucocorticoids (Milne 1986), tumour necrosis factor (van der Poll 1990) or IL-6 (Butler 1992). Several non-specific insults which occur in all major surgery such as fasting, anaesthetic agents and surgical stress may also contribute to a decline in the levels of free triiodothyronine. In addition, certain drugs such as dopamine (Van den Berghe 1994) and glucocorticoids (Brabant 1987), which may be administered after major surgery, have also been observed to produce a thyroid hormone deficiency.
Findings from paediatric studies suggest that cardiopulmonary bypass is associated with a decline in thyroid hormone levels with a trough at between 12 and 48 hours post bypass (Murzi 1995) and lasts for five to seven days post-operatively (Mitchell 1992). Mainwaring 2001 has demonstrated a decline in the levels of free triiodothyronine in serum by more than three-fifths in infants who undergo the first stage of the Norwood reconstruction for hypoplastic left heart syndrome. These peri and post operative T3 levels are substantially lower when compared to a normal value range for age matched normals (Zurakowski 1999). Mainwaring 1994 demonstrated an 80% decrease in TSH, free T3 and thyroglobulin levels in neonates following cardiopulmonary bypass and hypothermia. This transient, acquired hypothyroidism is thought to be associated with low cardiac output, left ventricular dysfunction, increased vascular resistance and impaired ventilatory drives (Bettendorf 1997).
Adult patients who undergo open heart surgery and receive triiodothyronine supplementation have demonstrated a dose-dependent increase in cardiac output (Klemperer 1995) which has been associated with an improved clinical outcome (Novitzky 1996). The changes in thyroid function after cardiopulmonary bypass in infants and neonates differ significantly from those of adults. Infants and neonates display a reduction in TSH, T3 and T4, whereas adults show decline in T3 only (Mainwaring 1994). Also, greater reductions have been reported in T3 in infants and neonates than adults (Mitchell 1992), hence, the question of thyroid hormone supplementation assumes a much more significant importance.
The use of thyroid hormone supplementation in infants undergoing cardiac surgery has been reported as a possible therapeutic option to improve outcome measures. This intervention would be of most clinical benefit in infants who have low cardiac output via an enhancement in left ventricular performance, a significant decrease in systemic vascular resistance and improved myocardial oxygen consumption. A recent case series reported on six paediatric patients who underwent complex open heart surgery and had low serum T3 levels in the post operative period (Chowdhury 1999). The single most important benefit observed was the conversion to sinus rhythm within 24 hours of T3 administration. In three patients in whom cardiac output could be reliably measured, the cardiac output increased by greater than 50% and systemic vascular resistance decreased by 25%. Urine output increased by 50% in all patients, resolution of metabolic acidosis was seen in four patients, and a reduction of additional inotropic support of up to 50% was reported. No side effects of treatment were documented in this series. Bialkowski 1997 and Mainwaring 1994 have also published non-randomised data which demonstrate an improvement in specific outcome measures with administration of intravenous triiodothyronine.
While it might seem relatively simple to administer thyroid hormone supplements in these infants peri-operatively, that might not be without risks. Supplementation may aggravate a reduction in TSH secretion which may prolong the duration of transient hypothyroidism (Murzi 1995). Maternal thyroxine treatment has been associated with newborn encephalopathy (Adamson 1995; Badawi 2000) and cerebral palsy (Nelson 1985; Girling 2001) and there have been concerns about supplementation of premature babies with transient hypothyroxinaemia (Osborn 2002). Van Wassenaer 1999 showed lower developmental index and higher risk of cerebral haemorrhage in infants born between 27 and 30 weeks gestation when treated thyroid hormone supplementation compared with infants that were not treated.
Other direct signs of thyroid hormone toxicity include tachycardia, cardiac dysrhythmia and hyperthermia.
Triiodothyronine has a half life of seven hours (Mainwaring 2000) and achieves its peak effects by two hours when administered intravenously. T4, however, may take up to two weeks to reach steady state and hence would not be an appropriate drug of choice in the peri-operative cardiac surgery setting in infants. A supplementation dose of triiodothyronine would specifically aim to restore serum T3 levels to within normal limits. Published dosage for the replacement of triiodothyronine intravenously in infants is 0.1-0.4 micrograms/kg/dose, 8 to 12 hourly (Shann 2001). The optimal timing of the commencement of thyroid hormone supplementation, whether intra-operatively or post-operatively, and the duration of therapy are at present uncertain and will require sub-group analysis within this review.
Bolus doses and intermittent infusions of triiodothyronine may need to be considered separately. It has been shown that T3 adsorbs onto plastic and therefore the type of plastic materials employed in the intravenous fluid administration system and the use of specific drug carriers in dilute solutions must be considered when calculating appropriate dosage for intermittent infusion. A polypropylene syringe with minimum volume polyvinyl chloride (PVC) extension tubing with albumin as a drug carrier is most efficacious in limiting T3 adsorption (Odgers 1984).
Thus, both biological plausibility and some observational evidence suggest that peri-operative thyroid hormone therapy for infants undergoing cardiac surgery might lead to improved post-operative cardiac function and improved outcomes. However, the benefits and possible harms of supplementation of triiodothyronine in this clinical setting are not clear.
Planned sub group analyses will include:
Age of infant - neonates (less than one month of age), infants (between one and twelve months of age)
Method of intravenous thyroid hormone administration - bolus, intermittent infusion or continuous infusion
Timing and duration of drug administration - intra-operative administration
only, supplementation commenced and ceased within 24 hours of operation,
supplementation commenced intra-operatively and continued for greater than
24 hours post-op, supplementation commenced within 24 hours of operation
and continued for greater than 24 hours post-op, supplementation which is
commenced greater than 24 hours after operation
Primary clinical outcome measures:
Mortality
Morbidity:
- length of hospital stay in days
- duration of respiratory assistance (IPPV, CPAP, oxygen supplementation) in days
Secondary clinical outcome measures:
Morbidity
- weight (in kilograms) in the first year and at five years
- length (in centimetres) in the first year and at five years
- head circumference (in centimetres) in the first year
- development: neurological abnormality (cerebral palsy) or developmental
delay on standardised tests in the first year and at age five
Adverse effects of thyroid hormone supplementation:
- toxicity - tachycardia (>160 beats per minute), cardiac dysrhythmia, hyperthermia (>37.5 degrees C)
- thyroid depression (<79 nmol/L for T4, <1.58 nmol/L for T3 and
0.8 nmol/L for TSH) for greater than one week on cessation of thyroid hormone
replacement (reference standards as per Zurakowski 1999)
Cardiac dysfunction - use of support such as post operative cardiopulmonary bypass (in hours), inotropes (duration, dose, number)
Thyroid hormone levels in the first week post operatively (T3, T4, rT3, TSH)
Additional hand searching was conducted of the Journal of Thoracic and Cardiovascular Surgery (Jan 1990 - Jan 2003) and Thyroid (Jan 1990 - Jan 2003) and abstracts of Paediatric surgery conference proceedings.
The RCTs which satisfied the inclusion criteria for this review were then graded for their methodological quality - blinding of randomisation to treatment or control, blinding of intervention, complete follow up and blinding of outcome measurement.
Portman 2000 provided additional data relevant to outcomes for his study, in the form of mean and standard deviations at specific post operative times.
Data were extracted by two reviewers. One reviewer entered the data into Review Manager (RevMan) computer software package. Treatment effects for categorical outcomes were expressed as relative risk (RR), risk difference (RD) and number needed to treat (NNT). Continuous data were analysed using mean difference. Ninety-five percent confidence intervals were used. Meta-analysis was not carried out because of differences between the two included studies.
Four studies were identified; however, only two were included in this review (Chowdhury 2001; Portman 2000). Mainwaring 1997 was excluded as all subjects were older than one year. Bettendorf 2000 included subjects aged between 2 days and 10 years, but did not report these subjects according to age groups. This meant that an analysis of a population of infants within this study aged from birth to one year was not possible. The study was therefore excluded.
Types of participants: All participants were undergoing surgery with cardiopulmonary bypass for congenital heart defects. Their ages ranged from birth to one year (Portman 2000), and up to 18 years of age (Chowdhury 2001). Chowdhury 2001 included a subgroup analysis of nine neonates (up to one month of age), however, they did not report their findings for the remainder of study subjects according to age. The neonatal subgroup was able to be included in this review, while the remainder of the subjects have been excluded from the review.
Portman 2000 included infants less than one year undergoing repair of a ventricular septal defect or tetralogy of Fallot, while Chowdhury 2001 included subjects whose serum total T3 level was less than 40ng/dL (or <60 ng/dL for newborns) on postoperative days 0, 1 or 2 and who required mechanical ventilation.
It was not clear from the study of Chowdhury 2001 as to the exclusion criteria of this study. Portman 2000 excluded infants with pulmonary atresia or severe pulmonary artery hypoplasia and those requiring additional surgical procedures such as repair of coarctation of the aorta.
Interventions: In Chowdhury 2001 the treatment group received a continuous T3 infusion at 0.05 - 0.15µg/kg/hr to maintain serum levels within the normal range (80-200ng/dL), compared to the control group who received no treatment. In Portman 2000, the treatment group received tri-iodothyronine 0.4µg/kg immediately before the start of cardiopulmonary bypass and again with myocardial reperfusion. The control group received saline placebo solution or no treatment.
Outcome measures:
Primary outcome measures for this review that were reported in Chowdhury 2001
included the length of post-operative hospital stay and duration of mechanical
ventilation (days). Both studies reported mortality.
The secondary outcome measures for this review that were reported in Chowdhury 2001 were serum T3 level (24 hours post operatively) and degree of inotrope support. In Portman 2000, the secondary outcome measures evaluated in this study included: Serum thyroid hormone levels measured at 1, 24 and 72 hours (free T3, total T3, total T4), inotropic requirements for the initial 24 hour post operative period and adverse events (cardiac dysrhythmias).
Outcome measures included post hoc in this review included Therapeutic Interventional Scoring System (TISS) score from Chowdhury 2001 and post operative heart rate.
Ongoing research into peri-operative thyroid hormone supplementation in infants undergoing cardiac surgery on cardiopulmonary bypass with an aim to improve post-operative morbidity and mortality is currently being undertaken by two groups whose studies were included in this review. Portman and colleagues are currently undertaking a Food and Drug Administration funded trial of peri-operative thyroid hormone supplementation in children under 2 years of age. It is the intention of this trial to enrol at least 100 patients in each of the treatment and control groups. Dr Irwin Klein, a member of the Chowdhury group, is continuing with the randomised controlled trial discussed in this review and to date has enrolled a further 71 subjects (See Table, Characteristics of ongoing studies).
Chowdhury 2001 evaluated 75 consecutive patients undergoing cardiac surgery between the ages of birth and 18 years. Subjects were assigned to the treatment arm of the study if the serum total T3 level was less than 40ng/dL (or <60 ng/dL for newborns) on postoperative days 0, 1 or 2 and the subject required mechanical ventilation. Twenty-eight subjects were deemed eligible and were randomised using a standard biostatistical randomisation method. This included 5 neonates who were randomised to the treatment group and 4 to the control group. There were no significant differences after randomisation between the neonate treatment and control groups in number of subjects requiring cardiopulmonary bypass, total bypass time, duration of cross clamping and the duration of hypothermic cardiac arrest. The control group was not treated, hence, blinding of the intervention was not undertaken. The length of follow up was five days post randomisation and all patients were appropriately accounted for at the conclusion of the study period. Whether outcome assessments were blinded was not stated by the authors.
For Portman 2000, although the authors state that randomisation was conducted, the specific randomisation procedure was not stated. The control and treatment groups showed no significant differences after randomisation in age, cardiopulmonary bypass time or aortic cross clamping time. The intervention, which was administered during the surgery, was not blinded. Although some of the control group received a saline solution placebo, other control subjects received no treatment. The outcome assessment was blinded as staff responsible for post-operative care were blinded to subject allocation. The duration of follow up was 72 hours post operation and all subjects were treated in their allocated groups with no exclusions after subject randomisation.
Chowdhury 2001 included subjects whose ages ranged from one day to 18 years. This study conducted a subgroup analysis of nine neonates who are included in this review. The data for the remainder of subjects were excluded from this review as they were not reported according to age group.
Primary clinical outcome measures:
Mortality:
There were no deaths in either the treatment or control groups in the Chowdhury 2001 and Portman 2000 studies.
Morbidity:
Length of hospital stay in days (Table 01.01):
In the neonate subgroup of Chowdhury 2001,
there was a mean length of hospital stay 38 days shorter in neonates treated
with T3 compared with neonates in the control group. This was not statistically
significant. Portman 2000 did not report length of hospital stay as a study outcome.
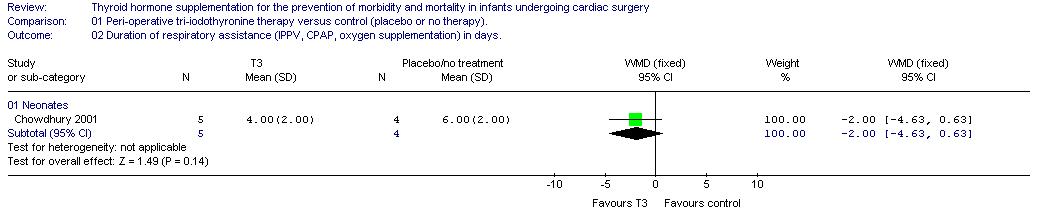
Duration of respiratory assistance (IPPV, CPAP, oxygen supplementation) in days (Table 01.02):
Chowdhury 2001 reported the mean duration
of mechanical ventilation was two days less in neonates treated with T3 compared
with neonates in the control group, which was not statistically significant.
Portman 2000 did not consider duration of respiratory assistance as a study outcome.
Chowdhury 2001 analysed the overall degree of post operative care by using the Therapeutic Interventional Scoring System (TISS) score; this was a post hoc outcome variable for this review. This involved the scoring of 76 different therapeutic and monitoring procedures which were scaled according to the degree of invasiveness, intensity and complexity of care with which the patient was provided. For the neonatal subgroup within this study, on post-randomisation days one to three these scores were significantly lower (P=0.037) in the treatment group (40 +/- 3ng/dL) compared with the untreated group (49 +/- 3 ng/dL). While this was not a primary outcome measure of this review, this score is a potentially important clinical tool and may be interpreted as an indirect measure of the review's primary outcomes.
Secondary clinical outcome measures:
Morbidity:
The studies did not provide data on subsequent growth (weight, length
and head circumference) and neurodevelopment (cerebral palsy or developmental
delay) in subjects.
Adverse effects of thyroid hormone supplementation:
Tachycardia (>160 beats per minute):
In Portman 2000, dichotomous values for
heart rate were unable to be obtained. It can be extrapolated from the study
graph that an unspecified number of treatment group subjects had a heart
rate of greater than 160 beats per minute at one and three hours post cardiopulmonary
bypass. A post hoc analysis of heart rate values from this study (Table
01.08) showed the mean post-operative heart rate was also significantly higher
for the treatment group versus the control group at these two specific points
in time (P <0.05). At one and three hours post operatively the treatment
group means were 155.7 and 156.8 respectively versus 131.0 and 142.0 for
the control group respectively.
Cardiac dysrhythmia (Table 01.03):
In the Portman 2000 study, a brief period
of supraventricular tachycardia was experienced by one subject in the treatment
group. No dysrhythmias were reported in the control group. Chowdhury 2001 reported that there were no cardiac dysrhythmias in the treatment or control groups.
Hyperthermia (>37.5 degrees C):
Temperature measurements in subjects were not reported in either of the studies.
Thyroid depression (<79 nmol/L for T4, <1.58 nmol/L for T3 and 0.8 nmol/L for TSH) for greater than one week on cessation of thyroid hormone replacement was not reported in the studies.
Cardiac dysfunction:
Use of support such as post operative cardiopulmonary bypass (in hours) was not assessed in either of the two studies.
Inotropes (duration, dose, number):
The authors of Chowdhury 2001 used an equation first described by Wernovsky 1995
for calculating total inotrope dose by adding the doses of dopamine and dobutamine
in micrograms per kilogram per minute and assigning an arbitrary equivalent
value of 10 µg · kg-1 · min-1 inotrope for each 0.1 µg
· kg-1 · min-1 epinephrine. For the neonatal subgroup in this
study, the treatment group had a score of 5 with a standard deviation of
3, while the score for the control group was 23 with a standard deviation
of 26. This was reported as being a statistically significant difference
(P = 0.037) in inotrope usage.
Portman 2000 reported that mean dopamine dose ranged between 1 to 3 ug/kg/min through the initial 24 hour post operative period for both the treatment and control groups. Dopamine requirements were not significantly different between groups evaluated at 1 and 6 hours after cardiopulmonary bypass. Two patients from each group received identical doses of amrinone during the same time period.
Thyroid hormone levels in the first week post operatively - T3, T4, rT3, TSH (Tables 01.04, 01.05, 01.06):
In Chowdhury 2001, measures of thyroid hormone levels were not reported for the specific age group required for this review. Portman 2000
reported that free and total T3 levels were substantially different between
the two groups, being higher in the treatment group for the first 24 hours
post operatively (significant difference (P <0.05) at 1 and 24 hours for
free T3 and at 1 hour post operatively for total T3 levels). Free and total
T3 levels were similar between groups by 72 hours post operatively. Total
T4 levels were similar between treatment and control groups at all times
from pre-cardiopulmonary bypass to 72 hours post operatively.
Major limitations of the review:
Two studies were identified in this review (Chowdhury 2001, Portman 2000).
These studies differed in inclusion criteria, the age of subjects they recruited
and in the method, dose and timing of tri-iodothryonine administration.
The included two studies were very small (total numbers of subjects were
14 and 28) which limited the power of this review.
The two studies assessed in this review used different dosing and timing of tri-iodothryonine administration. These differences limit the ability of this review to make specific conclusions regarding both the efficacy and optimal administration of peri-operative tri-iodothyronine. No single outcome, either primary or secondary, could be assessed using a meta-analysis of the two studies.
| Study | Methods | Participants | Interventions | Outcomes | Notes | Allocation concealment |
| Chowdhury 2001 | Randomised using standard biostatistical randomisation method. Intervention - not blinded (control group untreated). Completeness of follow up - all subjects were accounted for at the completion of the trial. Outcome assessment blinding - not stated. | 28 subjects. Subgroup of 9 neonates have been included in this review. Inclusion criteria: serum total T3 level of less than 40ng/dL (or <60 ng/dL for newborns). Exclusion criteria: not stated. | Treatment group: continuous T3 infusion at 0.05 - 0.15 microgram/kg/hr to maintain serum levels within normal range (80-200ng/dL) (N=5). Control group: intervention not stated (N=4). | Primary outcome measures: degree of inotropic support,
length of post-operative hospital stay and duration of mechanical ventilation
(days). Secondary outcome measures: serum T3 level (24 hours post operatively).
Post hoc analysis: Therapeutic interventional scoring system. | The authors of this study were contacted for further information regarding method of randomisation, blinding of intervention and outcome assessment and what, if any, placebo was given to the control group. Data for all study parameters were also requested for all subjects aged from birth to one year. The authors provided information regarding method of randomisation, but none of the other of the requested information was provided. | B |
| Portman 2000 | Randomised controlled trial. Method of randomisation was not stated. Intervention blinding: no - some control patients did not receive any placebo treatment. Completeness of follow up: there were no exclusions after randomisation. Outcome assessment blinding: yes. | 14 subjects. Inclusion criteria: Infants less than one year undergoing ventricular septal defect or tetralogy of Fallot repair. Exclusion criteria: infants with pulmonary atresia or severe pulmonary artery hypoplasia and those requiring additional surgical procedure such as repair of coarctation of the aorta. | Treatment group: tri-iodothyronine 0.4 microgram/kg immediately before the start of cardiopulmonary bypass and again with myocardial reperfusion (N=7). Control group: saline solution placebo or no treatment (N=7). | Primary outcome measures: inotropic requirements for the initial 24 hour post operative period. Secondary outcome measures: Serum thyroid hormone levels measured at 1, 24 and 72 hours (free T3, total T3, total T4) and adverse events (cardiac dysrhythmias). Post hoc measures: heart rate, systolic and diastolic blood pressure. | All staff in post operative period were said to be blinded to subject allocation. The authors were contacted for further information regarding method of randomisation and blinding of allocation and outcome assessment. Data were also requested for free T3, total T3, total T4, heart rate, blood pressure which were presented as graphs in the study paper. The authors responded with data relating to the graph study parameters. | B |
| Study | Reason for exclusion |
| Bettendorf 2000 | The study included subjects aged between one day to 10 years. However, there was no specific reporting of results for subjects aged between birth and one year. The authors were contacted for data regarding the outcomes of study parameters for this population, however, no response was received. |
| Mainwaring 1997 | All 28 participants were older than one year. |
| Study | Trial name or title | Participants | Interventions | Outcomes | Starting date | Contact information | Notes |
| Klein 2003 | Use of triiodothryonine in the postoperative period in pediatric patients undergoing heart surgery. | 71 patients. 18 aged between newborn and 3 months of age and 18 aged between 3 months and 1 year. | Continuation of randomised controlled trial (Chowdhury 2001) listed in this review. Hence, intervention is continuous T3 infusion at 0.05-0.15 mg/kg/hr to maintain serum levels within normal range (80-200ng/dL) | Degree of inotropic support, Therapeutic interventional scoring system, serum T3 level, length of hospital stay, mechanical ventilation (days). | Irwin Klein MD. Chief, Division of Endocrinology. North Shore
University Hospital. NYU School of Medicine. Manhasset, New York 11030. iklein@nshs.edu | ||
| Portman 2003 | The Triiodothyronine for Infants and Children undergoing Cardiopulmonary bypass (TRICC) study: Design and rationale. | Approximately 200 children under 2 years of age undergoing surgical procedures for congenital heart disease. | Triiodothyronine administered as a bolus of 0.04 micrograms/kg immediately prior to CPB, 0.4 micrograms/kg on the release of the aortic cross clamp and then 0.2 micrograms/kg at intervals of 3, 6 and 9 hours versus placebo. | Primary outcome measure: duration of mechanical ventilation after completion of cardiopulmonary bypass. Secondary outcome measures: fluid balance, length of time dependent on inotropic agents, duration of critical care unit stay, post operative mortality within the first 72 hours after surgery, requirement for mechanical-circulatory support and requirement for delayed chest closure. Multiple haemodynamic and Doppler echocardiographic parameters will also be assessed | August 2001 | Michael A Portman MD, Children's Hospital and Regional Medical Centre 4G-1, 4800 Sand Point Way NE, Seattle WA 98105. E-mail: Michael.Portman@seattlechildrens.org Phone: 206-987-2015 | This study is listed in NIH Clinical trials on Pubmed. |
Chowdhury D, Ojamaa K, Parnell VA, McMahon C, Sison CP, Klein I. A prospective randomized clinical study of thyroid hormone treatment after operations for complex congenital heart disease. Journal of Thoracic and Cardiovascular Surgery 2001;122:1023-5.
Portman 2000 {published data only}
Portman MA, Fearneyhough C, Ning XH, Duncan BW, Rosenthal GL, Lupinetti FM. Triiodothyronine repletion in infants during cardiopulmonary bypass for congenital heart disease. Journal of Thoracic and Cardiovascular Surgery 2000;120:604-8.
Bettendorf M, Schmidt KG, Grulich-Henn J, Ulmer HE, Heinrich UE. Tri-iodothyronine treatment in children after cardiac surgery: a double-blind, randomised, placebo-controlled study. Lancet 2000;356:529-34.
Mainwaring 1997 {published data only}
Mainwaring RD, Lamberti JJ, Nelson JC, Billman GF, Carter TL, Shell KH. Effects of tri-iodothyronine supplementation following modified Fontan procedure. Cardiology in the Young 1997;7:194-200.
Klein I. Use of triiodothryonine in the postoperative period in pediatric patients undergoing heart surgery.
Portman 2003 {unpublished data only}
Portman MA. The Triiodothyronine for Infants and Children undergoing Cardiopulmonary bypass (TRICC) study: Design and rationale.
* indicates the primary reference for the study
Adamson SJ, Alessandri LM, Badawi N, Burton PR, Pemberton PJ, Stanley FJ. Predictors of neonatal encephalopathy in full term infants. BMJ 1995;311:598-602.
Badawi N, Kurinczuk JJ, Mackenzie CL, Keogh JM, Burton PR, Pemberton PJ, Stanley FJ. Maternal thyroid disease: a risk factor for newborn encephalopathy in term infants. British Journal of Obstetrics and Gynaecology 2000;107:798-801.
Bettendorf M, Schmidt KG, Tiefenbacher U, Grulich-Henn J, Heinrich UE, Schonberg DK. Transient secondary hypothyroidism in children after cardiac surgery. Pediatric Research 1997;41:375-9.
Bialkowski J. Use of thyroid hormones after cardiopulmonary bypass in children. Cardiology in the Young 1997;7 (Suppl 1):378.
Brabant G, Brabant A, Ranft U, Ocran K, Kohrle J, Hesch RD, von-zur-Muhlen A. Circadian and pulsatile thyrotropin secretion in euthyroid man under the influence of thyroid hormone and glucocorticoid administration. The Journal of Clinical Endocrinology and Metabolism 1987;65:83-8.
Brogan TV, Bratton SL, Lynn AM. Thyroid function in infants following cardiac surgery: comparative effects of iodinated and noniodinated topical antiseptics. Critical Care Medicine 1997;25:1583-7.
Butler J, Chong GL, Baigrie RJ, Pillai R, Westaby S, Rocker GM. Cytokine response to cardiopulmonary bypass with membrane and bubble oxygenation. The Annals of Thoracic Surgery 1992;53:833-8.
Chowdury D, Parnell VA, Ojamaa K, Boxer R, Cooper R, Klein I. Usefulness of triiodothyronine (T3) treatment after surgery for complex congenital heart disease in infants and children. American Journal of Cardiology 1999;84:1107-9.
Dillmann WH. Cardiac function in thyroid disease: clinical features and management considerations. The Annals of Thoracic Surgery 1993;56:S9-S14.
Girling J, De Swiet M. Maternal thyroid disease: a risk factor for newborn encephalopathy (letter). British Journal of Obstetrics and Gynaecology 2001;108:769-70.
Klemperer JD, Klein I, Gomez M, Helm RE, Ojamaa K, Thomas SJ, Ison OW, Krieger K. Thyroid hormone treatment after coronary-artery bypass surgery. The New England Journal of Medicine 1995;333:1522-7.
Larsen PR, Ingbar SH. The thyroid gland. In: Wilson JD, Foster DW, editor(s). Textbook of Endocrinology. Philadelphia: WB Saunders, 1992:357-487.
Mainwaring RD, Lamberti JJ, Billman GF, Nelson JC. Suppression of the pituitary thyroid axis after cardiopulmonary bypass in the neonate. The Annals of Thoracic Surgery 1994;58:1078-82.
Mainwaring RD, Capparelli E, Schell K, Acosta M, Nelson JC. Pharmacokinetic evaluation of triiodothyronine supplementation in children after modified Fontan procedure. Circulation 2000;101:1423-9.
Mainwaring RD, Healy RM, Meier FA, Nelson JC, Norwood WI. Reduction in the levels of triidothyronine following the first stage of the Norwood reconstruction for hypoplastic left heart syndrome. Cardiology in the Young 2001;11:295-300.
Milne EMG, Elliott MJ, Pearson DT, Holden MP, Orskov H, Alberti KGMM. The effect on intermediary metabolism of open-heart surgery with deep hypothermia and circulatory arrest in infants less than 10 kilograms body weight. A preliminary study. Perfusion 1986;1:29-40.
Mitchell IM, Pollock JC, Jamieson MP, Donaghey SF, Paton RD, Logan RW. The effects of cardiopulmonary bypass on thyroid function in infants weighing less than five kilograms. Journal of Thoracic and Cardiovascular Surgery 1992;103:800-5.
Murzi B, Iervasi G, Masini S, Moschetti R, Vanini V, Zucchelli G, Biagini A. Thyroid hormones homeostasis in pediatric patients during and after cardiopulmonary bypass. The Annals of Thoracic Surgery 1995;59:481-5.
Nelson KB, Ellenberg JH. Antecedents of cerebral palsy. I. Univariate analysis of risks. American Journal of Diseases of Children 1985;139:1031-8.
Novitzky D, Fontanet H, Snyder M, Coblio N, Smith D, Parsonnet V. Impact of triiodothyronine on the survival of high-risk patients undergoing open heart surgery. Cardiology 1996;87:509-15.
Odgers CL, Phillips PJ, Shanks G. Intravenous liothyronine sodium (T3) for myxodema coma - pharmaceutical considerations. Australian Journal of Pharmacy 1984;14:181-8.
Osborn DA. Thyroid hormones for preventing neurodevelopmental impairment in preterm infants (Cochrane Review). In: Cochrane Library, Issue 2, 2002. Oxford: Update Software.
Schell D, Chin C, Chin R. Drug doses for children. Sydney: Children's Hospital at Westmead, 2004.
Shann F. Drug Doses. 11th edition. Parkville, Australia: Collective Pty Ltd, 2001, p40.
Stein SA, Adams PM, Shanklin DR, Mihailoff GA, Palnitkar MB. Thyroid hormone control of brain and motor development: molecular, neuroanatomical, and behavioural studies. In: Bercu B, Shulman DI, editor(s). Advances in Perinatal Thyroidology. New York: Plenum Press, 1991.
Utiger RD. Decreased extrathyroidal triiodothyronine production in nonthyroidal illness: benefit or harm? American Journal of Medicine 1980;69:807-10.
Van den Berghe G, de Zegher F, Lauwers P. Dopamine suppresses pituitary function in infants and children. Critical Care Medicine 1994;22:1747-53.
van der Poll T, Romijn JA, Wiersinga WM, Sauerwein HP. Tumor necrosis factor: a putative mediator of the sick euthyroid syndrome in man. Journal of Clinical Endocrinology and Metabolism 1990;71:1567-72.
Van Wassenaer AG, Kok JH, Briet JM, Pijning AM, de Vijlder JJ. Thyroid function in very preterm newborns: possible implications. Thyroid 1999;9:85-91.
Wernovsky G, Wypij D, Jonas R, Mayer J, Hanley F, Hickey P et al. Postoperative course and hemodynamic profile after the arterial switch operation in neonates and infants. A comparison of low-flow cardiopulmonary bypass and circulatory arrest. Circulation 1995;92:2226-35.
Zurakowski D, Di Canzio J, Majzoub JA. Pediatric reference intervals for serum thyroxine, triiodothyronine, thyrotropin and free thyroxine. Clinical Chemistry 1999;45:1087-91.
01.01 Length of hospital stay (days)
01.02 Duration of respiratory assistance (IPPV, CPAP, oxygen supplementation) in days.
01.03 Adverse events
01.04 Free T3 measurement (pg/ml)
01.05 Total T3 measurement (ng/ml)
01.06 Total T4 Measurement (ug/dl)
01.07 Heart Rate
| Comparison or outcome | Studies | Participants | Statistical method | Effect size |
|---|---|---|---|---|
| 01 Peri-operative tri-iodothyronine therapy versus control (placebo or no therapy) | ||||
| 01 Length of hospital stay (days) | WMD (fixed), 95% CI | Subtotals only | ||
| 02 Duration of respiratory assistance (IPPV, CPAP, oxygen supplementation) in days. | WMD (fixed), 95% CI | Subtotals only | ||
| 03 Adverse events | RR (fixed), 95% CI | Subtotals only | ||
| 04 Free T3 measurement (pg/ml) | WMD (fixed), 95% CI | Subtotals only | ||
| 05 Total T3 measurement (ng/ml) | WMD (fixed), 95% CI | Subtotals only | ||
| 06 Total T4 Measurement (ug/dl) | WMD (fixed), 95% CI | Subtotals only | ||
| 07 Heart Rate | WMD (fixed), 95% CI | Subtotals only | ||
Dr Tabitha Randell
Consultant Paediatrician
Mid Staffordshire General Hospitals
Weston Road
Stafford
UK
ST16 3SA
E-mail: tabitha.randell@msgh-tr.wmids.nhs.uk
| This review is published as a Cochrane review in The
Cochrane Library 2004, Issue 3, 2004 (see www.CochraneLibrary.net for information).
Cochrane reviews are regularly updated as new evidence emerges and in response
to comments and criticisms, and The Cochrane Library should be consulted
for the most recent version of the Review. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}