| | | | |
Research
|
| Obesity Is A Modifier of Autonomic Cardiac Responses to Fine Metal Particulates Jiu-Chiuan Chen,1,2 Jennifer M. Cavallari,2 Peter H. Stone,3,4 and David C. Christiani2,4 1Department of Epidemiology, University of North Carolina School of Public Health, Chapel Hill, North Carolina, USA; 2Department of Environmental Health, Harvard School of Public Health, Boston, Massachusetts, USA; 3Cardiovascular Division, Brigham and Women's Hospital, Boston, Massachusetts, USA; 4Harvard Medical School, Boston, Massachusetts, USA Abstract
Background: Increasing evidence suggests that obesity may impart greater susceptibility to adverse effects of air pollution. Particulate matter, especially PM2.5 (particulate matter with aerodynamic diameter ≤ 2.5 µm) , is associated with increased cardiac events and reduction of heart rate variability (HRV) . Objectives: Our goal was to investigate whether particle-mediated autonomic modulation is aggravated in obese individuals. Methods: We examined PM2.5-mediated acute effects on HRV and heart rate (HR) using 10 24-hr and 13 48-hr ambulatory electrocardiogram recordings collected from 18 boilermakers (39.5 ± 9.1 years of age) exposed to high levels of metal particulates. Average HR and 5-min HRV [SDNN: standard deviation of normal-to-normal intervals (NN) ; rMSSD: square-root of mean squared-differences of successive NN intervals ; HF: high-frequency power 0.15–0.4 Hz] and personal PM2.5 exposures were continuously monitored. Subjects with body mass index ≥ 30 kg/m2 were classified as obese. Mixed-effect models were used for statistical analyses. Results: Half (50%) of the study subjects were obese. After adjustment for confounders, each 1-mg/m3 increase in 4-hr moving average PM2.5 was associated with HR increase of 5.9 bpm [95% confidence interval (CI) , 4.2 to 7.7] and with 5-min HRV reduction by 6.5% (95% CI, 1.9 to 11.3%) for SDNN, 1.7% (95% CI, –4.9 to 8.4%) for rMSSD, and 8.8% (95% CI, –3.8 to 21.3%) for HF. Obese individuals had greater PM2.5-mediated HRV reductions (2- to 3-fold differences) than nonobese individuals, and had more PM2.5-mediated HR increases (9-bpm vs. 4-bpm increase in HR for each 1-mg/m3 increase in PM2.5 ; p < 0.001) . Conclusions: Our study revealed greater autonomic cardiac responses to metal particulates in obese workers, supporting the hypothesis that obesity may impart greater susceptibility to acute cardiovascular effects of fine particles. Key words: air pollution, environmental health, heart rate variability, obesity, risk factors, susceptibility. Environ Health Perspect 115:1002–1006 (2007) . doi:10.1289/ehp.9609 available via http://dx.doi.org/ [Online 26 February 2007]
Address correspondence to D.C. Christiani, Occupational Health Program, Harvard School of Public Health, Rm 1402, HSPH-1, 665 Huntington Ave., Boston, MA 02115, USA. Telephone: (617) 432-3323. Fax: (617) 432-3441. E-mail: dchristi@hsph.harvard.edu We thank E. Rodrigues, J. Hart, T.-M. Yeh, J. Natkin, J.-Y. Kim, and S. Mukherjee for their important contribution to data collection. Special thanks to the International Brotherhood of Boilermakers Local No. 29, Quincy, Massachusetts. This study was supported by National Institutes of Health grants ES09860 and ES00002. The authors declare they have no competing financial interests. Received 14 August 2006 ; accepted 26 February 2007. |
|
|
|
Altered autonomic cardiac activities, such as heart rate (HR) increases and overall heart rate variability (HRV) reduction (Zareba et al. 2001), in response to particulate matter (PM) exposure have been hypothesized as one of the major mechanistic pathways for PM-related adverse cardiac events. As reported in a recent extensive review on the health effects of fine particulate air pollution (Pope and Dockery 2006), PM exposure has generally been found to be associated with declines in most HRV measures, suggesting adverse effects on cardiac autonomic function. Pope and Dockery (2006) also noted that understanding of who is most at risk or susceptible is one of the most important gaps in our current knowledge regarding PM-related health effects.
The marked increases in prevalence of overweight and obesity over the last two decades in the United States has imposed a major public health concern (Hedley et al. 2004). Recent research findings point to the possibility that obesity may impart greater susceptibility to the adverse effects of PM exposure. In an inhalation study of healthy children 6–13 years of age, body mass index (BMI) was associated with a graded increase in the estimated total lung dose of deposited fine particles (i.e., deposited particles/time) (Bennett and Zeman 2004). In a panel study of 44 senior citizens, vascular inflammatory response (measured by C-reactive protein) to ambient levels of PM2.5 (particulate matter with aerodynamic diameter ≤ 2.5µm) averaged over 1–7 days is greater in obese (BMI ≥ 30 kg/m2) than in nonobese subjects (Dubowsky et al. 2006). However, no prior studies have examined the differential autonomic cardiac responses in obese versus nonobese individuals.
The objective of this study is to investigate whether autonomic cardiac responses to metal particulates are aggravated in the obese subpopulation. We hypothesized that obese participants would experience greater autonomic modulation than those without obesity.
Study population. The study was approved by the Human Subject Committee of Harvard School of Public Health, and written informed consent was obtained from each participant. The study population came from a cohort of boilermakers in eastern Massachusetts. Between 2003 and 2004, subjects were recruited to participate in a study to assess acute cardiopulmonary and inflammatory responses to particulates. None met any predetermined exclusion criteria (unstable angina, bundle branch or atrioventricular block, atrial fibrillation or flutter, or other rhythms or clinical conditions compromising HRV analysis). Of 35 eligible workers who had completed physical examination (medical histories, weight and height measurement, and resting blood pressure), 20 volunteered for the intensive monitoring of autonomic cardiac activities, personal PM2.5 exposures, and daily activities for 24–48 hr during the same winter period (25 January to 8 February in 2003 and 31 January to 8 February in 2004). There were two defective ambulatory electrocardiogram (AECG) recordings, leaving 18 subjects included in the current study. All workers were at a welding school on the sampling day. This indoor work environment was well ventilated and temperature controlled, and workers were exposed to fine particulates while arc welding, grinding, cutting, or involved in other activities on mild steel. We have previously documented high levels of fine metal particulates in the studied workplace (Kim et al. 2003; Liu et al. 2005).
Personal characteristics. We used a modified American Thoracic Society questionnaire (Ferris 1978) to collect information on respiratory symptoms, personal medical histories, and current use of medication. Also, we solicited information on demographic features, lifestyle factors (e.g., smoking, drinking, exercise), and recent occupational activities. Self-reported status of diabetes mellitus and smoking was furthered verified by structured interviews and urine tests for sugar and cotinine. Because both HRV and PM exposure levels are potentially affected by other activities, all workers were asked to record the times when they performed different occupational activities in the workplace and also times spent in usual daily activities, such as cigarette smoking, coffee drinking, eating, alcohol consumption, exercising, and sleeping. All participants had their body weights (kilograms) and standing heights (meters) measured in the early morning by trained personnel. Subjects were classified as obese if their calculated BMI was ≥ 30 kg/m2. Two to three blood pressure determinations were made by the same physician after subjects had been sitting and resting for 10–15 min before the work shift, and the average was used for analyses.
AECG monitoring. AECG recordings (24-hr or 48-hr) were performed using Applied Cardiac Systems AM cassette recorders (Laguna Beach, CA). Recorded signals from two leads (aVF and modified V5) were synchronized with personal air samplers. Recordings were analyzed in the AECG Core Laboratory at Brigham and Women's Hospital.
Measurement of autonomic cardiac activities. We used HRV and HR as measures of autonomic cardiac activities in response to PM exposure. Using a Marquette MARS Workstation (Milwaukee, WI), an AECG research specialist reviewed and, when necessary, corrected automatically determined categorization of QRS complexes into normal or ectopic beats. After regions of noise and artifact were eliminated, software facilities on the MARS were used to export beat timing and annotation information for analysis and creation of response variables through customized PC-based software written in C-language. Only normal-to-normal (NN) intervals between 150 and 5,000 msec with NN ratios between 0.8 and 1.2 were submitted to HRV analyses. Linear interpolation was constructed to replace missing beats including the removed ectopic beats and epochs with noise and artifacts. All HRV measures were computed on each 5-min epoch from a rate tachogram constructed from acceptable NN intervals (Berger et al. 1986). For time-domain parameters, including SDNN (standard deviation of NN intervals; in milliseconds), rMSSD (square root of the mean squared differences of successive NN intervals; in milliseconds) and average HR (in beats per minute), the tachogram gaps were set to the mean tachogram rate over all available intervals to avoid spurious variance that might result from interpolation, and all variance measures were appropriately scaled for the available tachogram duration. We used the high-frequency (HF) power of HRV (0.15–0.4 Hz) as the index of vagal activity. Our quality control data indicated an excellent agreement (intraclass correlation coefficient > 0.95) between results of repeated analyses for all time-domain and frequency-domain parameters.
Measurement of particulate exposure. PM2.5 was the main particulate exposure characterized in this study, and both occupational and nonoccupational sources were noted. Welding fume, which has a rich content of ultrafine particles (diameter ≤ 0.1 µm) and transition metals, was the main occupational source of PM2.5 in our study population (Zimmer 2002). The levels of metal particulates, although expected to be high, were not directly measured because real-time personal monitoring of airborne transition metals was not available. Nonoccupational sources of fine particles included tobacco smoke, food preparation, vehicle exhaust, and ambient air pollution. A DustTrak model 8520 aerosol monitor (TSI Inc., St. Paul, MN) was used to continuously monitor PM2.5 within the participant's breathing zone, and moving averages from ≥ 5 min were generated. Subjects were instructed to wear the monitors while awake and to place the DustTrak on a nightstand while asleep. For participants who slept on the preceding night in the same room as on the sampled night, their previous night PM2.5 concentrations were approximated by data from the sampled night. Otherwise, the previous night's PM2.5 data were omitted. Only 4-hr moving averages were used in the statistical analyses, to parallel previous reports (Gold et al. 2000; Magari et al. 2001). We also quantified cross-shift PM2.5 exposures using a model 200 personal exposure monitor (PEM; MSP Corporation, Minneapolis, MN) in 2003 and Harvard Cyclones (BGI Inc., Waltham, MA) in 2004 to collect gravimetric air samples. We have documented a good agreement (Spearman's r > 0.90) between real-time readings by DustTrak and gravimetric measures in this occupational setting (Kim et al. 2004).
Statistical analysis. Becauseour study subjects were moving freely during concurrently continuous AECG and personal PM2.5 exposure monitoring, there were unavoidable time periods when either AECG tracings contained much noise or real-time PM readings were missing. To reduce artifacts of these measurements, we restricted our analyses to AECG segments with > 90% valid beats matched to 5-min epochs with uninterrupted measures of PM2.5 in the preceding 4 hr. Also, the length of AECG recording sessions was not uniform across all subjects. As a result, we had an unbalanced data structure with different numbers of repeated measures of 5-min epochs that were not equally spaced in time. Therefore, models with either an exchangeable or a common autoregressive covariance structure, which assume that the time intervals of repeated measures are equal and the same for all individuals, may not be appropriate for our data.
To fully account for the autocorrelation of repeated measures within each subject, we constructed mixed-effect models with a time-dependent covariance structure as an exponential function of temporal distances, such that the correlations of repeated measurements are smaller than observations that were further apart (programming codes available on request). The main effects of 4-hr moving average PM2.5 exposure on HRV and HR were first estimated directly from these mixed-effect models, and then the interaction term between PM2.5 and obesity was added to evaluate the differential responses between obese and nonobese subjects. In adjusted analyses, we first included age, smoking and drinking habits, calendar year, blood pressure measured at baseline, and obesity. Pulse pressure (i.e., the difference of systolic and diastolic) entered the mixed model, because our empirical data suggested it predicted HRV parameters better than either systolic or diastolic component alone. After accounting for the potential confounding by these time-independent covariates, we then entered each recorded time-varying activity (eating, smoking, coffee drinking, alcohol drinking, exercising, sleeping, and work day) as an indicator variable, and the circadian patterns of HRV and HR were represented by three other indicator variables representing time of day [morning (0700–1100 hr), afternoon (1200–1700 hr), evening (1800–2200 hr), and nighttime (2300–0600 hr)]. All mixed-effects models include a subject-specific random effect to account for any unmeasured between-subject difference in the HRV and HR measures. All these statistical analyses were carried out using SAS 8.0 software package (SAS Institute Inc., Cary, NC), using PROC MIXED procedures and SP(POW) structures with spatial processes replaced by temporal distances. We used the autocorrelation plots of residuals estimated from the final models to evaluate the appropriateness of assumed time-dependent covariance structure. We also carried out sensitivity analyses to assess any potential biases arising from residual confounding by unmeasured time-varying activities, the sensitivity of our results to different model specifications, and the influence of other comorbidities.
The characteristics of study population are presented in Table 1. No major differences in personal and occupational characteristics were noted between the current study population and the other eligible subjects (n = 17). Of the 18 participants of the AECG study, all were male, with 16 white (three Hispanics) and three African Americans. Although 50% (n = 9) were classified as obese, no participant had reported or had laboratory evidence of diabetes. None of them were taking any medication at the time of examination. No significant correlation between cross-shift PM2.5 concentrations and individual's BMI was noted (Spearman's r = 0.16, p = 0.48). Of all 23 AECG recordings, 12 were collected for 24 hr and 11 were for 48 hr. The SDNN index (mean of standard deviation of all RR intervals for all 5-min segments throughout the entire recordings) was 115.3 ± 7.5 msec and 24-hr average HR was 90.3 ± 1.9 bpm. Higher resting systolic and diastolic blood pressures before the exposure were noted among obese participants than among the nonobese (Table 1). Obese subjects also had slightly higher average HR than nonobese subjects (93.5 ± 2.8 vs. 86.9 ± 2.6 bpm; p = 0.07), but their 24-hr SDNN index were similar (117 ± 8 vs. 114 ± 13 msec; p = 0.82). Neither the 5-min SDNN (64.5 ± 4.5 msec), rMSSD (52.0 ± 5.2 msec), HF power (801.7 ± 119.1 msec2), nor average HR (84.8 ± 2.3 bpm) significantly differed between obese and nonobese subjects. The 4-hr moving average PM2.5 concentration was 0.48 ± 0.01 mg/m3, ranging from nearly nondetectable to 4.23 mg/m3.
Table 1.

|
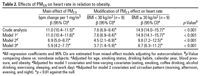
Table 2.
|
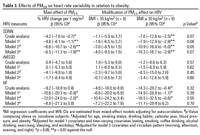
Table 3.
|
Effects of PM2.5 on HR and HRV. Tables 2 and 3 show statistically significant effects, as estimated from mixed-effect models, of PM2.5 on autonomic cardiac activities. For each 1-mg/m3 increase in 4-hr average PM2.5, HR increased by 6.9 bpm [95% confidence interval (CI), 5.0 to 8.7; p < 0.0001]; 5-min HRV reduced by 6.6% (95% CI, 2.6 to 10.7) for SDNN (p = 0.001), 4.1% (95% CI, –1.8 to 9.9) for rMSSD (p = 0.17), and 13.0% (95% CI, 2.0 to 24.0) for HF power (p = 0.02), after adjustment for age, smoking status, drinking habit, calendar year, baseline pulse pressure, obesity and time-varying activities (all main effects in model 2 of Tables 2 and 3). There were only few changes to the observed significant associations of PM2.5 with average HR and 5-min SDNN after additionally adjusting for the circadian rhythm (morning, afternoon, evening, and night), but the estimated effect on HF power of HRV was diminished (from 13% to 8.8% reduction) and became statistically nonsignificant. Autocorrelation plots did not reveal any remaining temporal correlation among the residuals of constructed mixed effect models with time-dependent covariance structure, indicating a goodness of fit to our data.
Effect modification by obesity status. We noted that the effects of PM2.5 on increases in average HR and reduction of HRV depended on individual's obesity status, with more aggravated electrophysiologic responses observed in obese subjects. For instance (effect modification in model 3 of Table 2), each 1-mg/m3 increase in PM2.5 was associated with an 8.7-bpm increase in average HR among obese subjects and a 3.7-bpm increased in nonobese subjects (p < 0.001 comparing obese vs. nonobese). Among those with obesity, for each 1-mg/m3 increase in PM2.5, there were statistically significant associations with a 10.3% reduction in SDNN and 11.1% reduction in HF power of HRV; but the associated 3.4% reduction in rMSSD was statistically nonsignificant. The corresponding responses were 4.0%, 7.2%, and 0.7% for nonobese individuals, and none of these associations were statistically significant (effect modification in all model 3 of Table 3). Only the between-subgroup comparison of the PM-mediated effect on average HR was statistically significant, and a marginally significant difference (p = 0.07) was noted for PM2.5–SDNN association, probably because of the small sample size. However, there was a very consistent pattern of effect modification by individual's obesity status across all adjusted models for all time- and frequency-domain measures of HRV. Greater PM2.5-mediated HRV reductions (2- to 3-fold differences) in SDNN, rMSSD, and HF power were observed in obese than in nonobese subjects.
Sensitivity analyses. First, the observed changes to estimated effects of PM2.5 on HRV measures (from model 1 estimates to model 2 estimates of Table 3) suggested that PM2.5–HRV association could be confounded by time-varying activities. Although we had accounted for several activities in the analyses, we might have missed other important time-varying covariates that correlate both PM2.5 exposure and HRV over time. To address this concern with residual confounding, we added to the mixed-effect model (model 2) 23 indicator variables representing the effects of unmeasured activities that presumably affect the SDNN hour by hour. We found that the negative association between PM2.5 and SDNN remained statistically significant (–6.6%; 95% CI, –11.3 to –1.9; p = 0.006), and the observed SDNN reduction in response to PM2.5 was still greater in obese than in nonobese subjects (10.6% vs. 3.9%, p = 0.07).
Second, previous air pollution studies on HRV changes have estimated the short-term effects of PM2.5 on HRV using different model forms, such as fixed-effect models (Gold et al. 2000; Pope et al. 1999) and generalized estimation equation (GEE) models (Holguin et al. 2003). When we reanalyzed our data by including individual intercepts (fixed-effect models with either 18 or 23 intercepts) or re-estimated PM effects using GEE models assuming a first-order autoregressive correlation among repeated measures, the PM2.5–SDNN association remained statistically significant and the difference between obese and nonobese subjects persisted (data not shown).
Third, because obesity and hypertension tend to be clustered together, the observed differential effect of PM2.5 on HRV might simply reflect the enhanced susceptibility to PM-mediated HRV reduction among those with hypertension, as reported by others (Holguin et al. 2003; Liao et al. 2004). After we excluded two obese subjects who also had physician-diagnosed hypertension, the observed PM2.5-mediated acute SDNN reduction was still greater among obese subjects (7.1%; 95% CI, 4.9 to 9.4) than the corresponding effect in nonobese subjects (2.0%; 95% CI, –0.1 to 4.0). Finally, few studies on PM–HRV associations had included adjustment for time-varying average HR in the multivariable models (Magari et al. 2001, 2002). Average HR is strongly correlated with ventilation (Mermier et al. 1993; Samet et al. 1993), which is affected by unmeasured physical activities and can influence HRV measures. Therefore, to adjust further for influence of ventilation, we additionally included average HR in the SDNN models. Still, we observed a statistically significant effect of PM2.5 on SDNN (7.1% reduction, p = 0.003), and the greater response in obese (11.4% reduction in SDNN) versus nonobese subjects (4.3% reduction in SDNN) remained (p = 0.06). Sensitivity analyses also yielded consistent findings for effects of PM2.5 on average HR and statistically significant effect modification by obesity.
Our study suggests that autonomic cardiac activities in response to PM are differential, depending on individual's obesity status. In obese subjects (BMI ≥ 30 kg/m2), there was an 8.7-bpm increase in HR, whereas the nonobese individuals experienced a 3.7-bpm increase in HR when exposed to the same level (1 mg/m3) of PM2.5 exposure. Greater PM2.5-mediated HRV reductions (2- to 3-fold differences) in SDNN, rMSSD, and HF power were observed in obese subjects, although these differences did not reach statistical significance. These observed alterations in autonomic cardiac activities in response to PM2.5 exposure may indicate either activated sympathetic stress response or diminished vagal control. The consistent associations between PM2.5 and increased HR and reduced HRV (SDNN and HF), which remained even after adjustment of many time-varying confounders, add to existing literature on the adverse effect of particulate air pollution on autonomic modulation.
The observed differential responses between obese and nonobese individuals support the concept that obesity may impart greater susceptibility to PM-associated acute cardiovascular effects. Recent laboratory data on toxicokinetic features of obese subjects exposed to air pollutants did provide supportive evidence for this concept (Bennett and Zeman 2004). Acute changes in lung mechanics have been suggested to result in the enhanced airway hyperresponsiveness and inflammatory responses to ozone in ob/ob obese mice (Rivera-Sanchez et al. 2004; Shore et al. 2003), although the confirmatory data for aggravated PM responses in obese subjects are still lacking. Interestingly, two recent epidemiologic studies showed that the reduction in pulmonary function measures associated with both short-term and long-term PM exposures were several times higher for obese children/adolescents than those of normal weight (Luttmann-Gibson and Dockery 2004; Occhiuto et al. 2004). In one small panel study on individuals with chronic obstructive pulmonary diseases (n = 18) or recent myocardial infarction (n = 12), it was reported that the positive PM2.5–SDNN association increased with decreasing baseline forced expiratory volume in the first second (Wheeler et al. 2006). Whether changes in pulmonary functions also contribute to greater susceptibility to developing PM-mediated acute cardiovascular effects in obese individuals need further investigation.
If confirmed by other studies, the identification of obesity as a secondary modifier may have mechanistic implications for the cardiovascular effects of air pollution. Airway or parenchymal inflammatory responses to PM have been hypothesized to be the inciting event followed by a cascade of pathophysiologic changes in autonomic cardiac, systemic inflammation, and hemostatic activities, all of which may ultimately lead to the acute cardiac events associated with PM exposure (Lippmann et al. 2003). More recent data have shown a positive correlation between exhaled nitric oxide, a marker of pulmonary inflammation, and BMI in healthy adults (De Winter-de Groot et al. 2005; Kazaks et al. 2005). Future studies should investigate whether this presumed pulmonary inflammation in obese individuals translates into an enhancement of local inflammatory response to air pollution, thus contributing to the greater PM-mediated HRV reduction in obese individuals.
Previous studies have attempted to identify subpopulations susceptible to acute HRV responses to PM exposure, but the results were varied. Among 21 Boston residents (Gold et al. 2000), smokers were found to have a greater reduction in HRV associated with PM exposures than nonsmokers (p = 0.08). A small panel study on 19 subject (9 young and 10 elderly) in Taipei, Taiwan (Chan et al. 2004), revealed a larger decrease in HRV among the elderly with impaired lung functions. Also, there is evidence suggesting that those with hypertension may be more susceptible. In a study among 34 elderly subjects living in Mexico City (Holguin et al. 2003), those with hypertension had a greater reduction in the HF power of HRV in response to PM2.5 than those without hypertension. Using data from 497 elderly men in the Normative Aging Study (NAS), investigators showed that the negative associations between PM2.5 and HRV were greater for those with hypertension and diabetes mellitus (Park et al. 2005). Because most of these studies were conducted on the elderly population with prevalent comorbidities, it remained unclear whether the observed greater PM–HRV associations were imparted by the comorbid disease processes or attributed to other personal physical characteristics (e.g., obesity) that are closely associated with both hypertension and diabetes mellitus. For instance, in a recent analysis on gene-by-drug-by-environment interaction for PM2.5-mediated autonomic effects (Schwartz et al. 2005), descriptive data from 441 subjects in the NAS did suggest that elderly obese people had greater HRV reduction than elderly nonobese subjects. However, it was unclear where such differential response would have persisted, had the analysis accounted for other comorbid conditions (67% hypertensive and 15% diabetic). As indicated in our sensitivity analyses, in this working population of healthy men without overt cardiovascular diseases and diabetes, it is noteworthy that the aggravated response to acute PM2.5 in those who were obese remained even after we excluded two participants with both obesity and hypertension.
Exposure characteristics of workplace particulates in our study have implications for future epidemiologic studies on PM-mediated cardiovascular effects. First, PM2.5 levels in this occupational setting are much higher than ambient particulate concentrations. Community-based studies need to be conducted to examine whether modification of acute PM effect by obesity status depends on the PM levels. Second, our study findings lend support for ongoing efforts in understanding the cardiotoxicity of metal particulate, especially among the obese subpopulations. Future studies should also examine whether the population susceptibility to PM-mediated cardiovascular effects could be related to differences in the PM compositions, including metal constituents.
We recognize several study limitations. First, measured changes in 5-min HRV reflect only short-term autonomic modulation in response to particulates. Definitive clinical significance of such changes should be elucidated. Second, external validity or generalizability of our results may be limited by the small sample size of 18 subjects. Whether regular exposure to high levels of toxic metal particulates makes subjects more susceptible to acute PM effects than is the general population is unknown, although our ad hoc analyses did not reveal any effect modification by the years of tenure as professional boilermakers (data not shown). Nevertheless, the internal validity of our findings is supported by the representativeness of our study subjects. Finally, because we did not simultaneously measure other co-pollutants (e.g., ozone, nitrogen dioxide), we failed to directly evaluate the potential confounding by any of these co-pollutants. Also, we were unable to address the possibility that the aggravated HRV reduction in response to PM2.5 might be attributable to obese subjects' enhanced sensitivity to some co-pollutants (e.g., O3) which could with PM2.5 affect autonomic system activities. Nevertheless, the documented levels of O3 and NO2 in this occupational cohort were low (Liu et al. 2005), and findings on gaseous co-pollutants in relation to HRV are limited and inconsistent. Personal indoor measures of PM2.5 do not covary with personal measures of O3, NO2 and sulfur dioxide (Sarnat et al. 2000). Thus, the likelihood of such unmeasured confounding is low.
We found that adverse cardiovascular responses to PM2.5 exposures, reflected in reduction of HRV and increases in HR, were aggravated in obese men who did not have overt cardiovascular diseases but were exposed to high levels of metal particulates. These findings support the concept that obesity may impart greater susceptibility to PM-associated acute cardiovascular effects.
|
|
|
| [References Listed in PubMed]
References Bennett WD, Zeman KL. 2004. Effect of body size on breathing pattern and fine-particle deposition in children. J Appl Physiol 97:821–826.
Berger RD, Akselrod S, Gordon D, Cohen RJ. 1986. An efficient algorithm for spectral analysis of heart rate variability. IEEE Trans Biomed Eng 33:900–904.
Chan CC, Chuang KJ, Shiao GM, Lin LY. 2004. Personal exposure to submicrometer particles and heart rate variability in human subjects. Environ Health Perspect 112: 1063–1067.
De Winter-de Groot KM, Van der Ent CK, Prins I, Tersmette JM, Uiterwaal CS. 2005. Exhaled nitric oxide: the missing link between asthma and obesity? J Allergy Clin Immunol 115:419–420.
Dubowsky SD, Suh H, Schwartz J, Coull BA, Gold DR. 2006. Diabetes, obesity, and hypertension may enhance associations between air pollution and markers of systemic inflammation. Environ Health Perspect 114:992–998.
Ferris BG. 1978. Epidemiology Standardization Project (American Thoracic Society). Am Rev Respir Dis 118:1–120.
Gold DR, Litonjua A, Schwartz J, Lovett E, Larson A, Nearing B, et al. 2000. Ambient pollution and heart rate variability. Circulation 101:1267–1273.
Hedley AA, Ogden CL, Johnson CL, Carroll MD, Curtin LR, Flegal KM. 2004. Prevalence of overweight and obesity among US children, adolescents, and adults, 1999–2002. JAMA 291:2847–2850.
Holguin F, Tellez-Rojo MM, Hernandez M, Cortez M, Chow JC, Watson JG, et al. 2003. Air pollution and heart rate variability among the elderly in Mexico City. Epidemiology 14:521–527.
Kazaks A, Uriu-Adams JY, Stern JS, Albertson TE. 2005. No significant relationship between exhaled nitric oxide and body mass index in people with asthma. J Allergy Clin Immunol 116:929–930.
Kim JY, Hauser R, Wand MP, Herrick RF, Amarasiriwardena CJ, Christiani DC. 2003. The association of expired nitric oxide with occupational particulate metal exposure. Environ Res 93:158–166.
Kim JY, Magari SR, Herrick RF, Smith TJ, Christiani DC. 2004. Comparison of fine particle measurements from a direct-reading instrument and a gravimetric sampling method. J Occup Environ Hyg 1:707–715.
Liao D, Duan Y, Whitsel EA, Zheng ZJ, Heiss G, Chinchilli VM, et al. 2004. Association of higher levels of ambient criteria pollutants with impaired cardiac autonomic control: a population-based study. Am J Epidemiol 159: 768–777.
Lippmann M, Frampton M, Schwartz J, Dockery D, Schlesinger R, Koutrakis P, et al. 2003. The U.S. Environmental Protection Agency Particulate Matter Health Effects Research Centers Program: a midcourse report of status, progress, and plans. Environ Health Perspect 111: 1074–1092.
Liu Y, Woodin MA, Smith TJ, Herrick RF, Williams PL, Hauser R, et al. 2005. Exposure to fuel-oil ash and welding emissions during the overhaul of an oil-fired boiler. J Occup Environ Hyg 2:435–443.
Luttmann-Gibson H, Dockery DW. 2004. Short-term effects of air pollution on lung function: are obese children at higher risk? [Abstract]. Am J Respir Crit Care Med 169:A19.
Magari SR, Hauser R, Schwartz J, Williams PL, Smith TJ, Christiani DC. 2001. Association of heart rate variability with occupational and environmental exposure to particulate air pollution. Circulation 104:986–991.
Magari SR, Schwartz J, Williams PL, Hauser R, Smith TJ, Christiani DC. 2002. The association between personal measurements of environmental exposure to particulates and heart rate variability. Epidemiology 13:305–310.
Mermier CM, Samet JM, Lambert WE, Chick TW. 1993. Evaluation of the relationship between heart rate and ventilation for epidemiologic studies. Arch Environ Health 48: 263–269.
Occhiuto JS, Dockery DW, Speizer FE. 2004. Obesity as a modifier of the association of pulmonary function with air pollution in adolescents [Abstract]. Am J Respir Crit Care Med 169:A19.
Park SK, O'Neill MS, Vokonas PS, Sparrow D, Schwartz J. 2005. Effects of air pollution on heart rate variability: the VA Normative Aging Study. Environ Health Perspect 113:304–309.
Pope CA III, Dockery DW. 2006. Health effects of fine particulate air pollution: lines that connect. J Air Waste Manag Assoc 56:709–742.
Pope CA III, Verrier RL, Lovett EG, Larson AC, Raizenne ME, Kanner RE, et al. 1999. Heart rate variability associated with particulate air pollution. Am Heart J 138: 890–899.
Rivera-Sanchez YM, Johnston RA, Schwartzman IN, Valone J, Silverman ES, Fredberg JJ, et al. 2004. Differential effects of ozone on airway and tissue mechanics in obese mice. J Appl Physiol 96:2200–2206.
Samet JM, Lambert WE, James DS, Mermier CM, Chick TW. 1993. Assessment of heart rate as a predictor of ventilation. Res Rep Health Eff Inst 59:19–55.
Sarnat JA, Koutrakis P, Suh HH. 2000. Assessing the relationship between personal particulate and gaseous exposures of senior citizens living in Baltimore, MD. J Air Waste Manag Assoc 50:1184–1198.
Schwartz J, Park SK, O'Neill MS, Vokonas PS, Sparrow D, Weiss S, et al. 2005. Glutathione-S-transferase M1, obesity, statins, and autonomic effects of particles: gene-by-drug-by-environment interaction. Am J Respir Crit Care Med 172:1529–1533.
Shore SA, Rivera-Sanchez YM, Schwartzman IN, Johnston RA. 2003. Responses to ozone are increased in obese mice. J Appl Physiol 95:938–945.
Wheeler A, Zanobetti A, Gold DR, Schwartz J, Stone P, Suh HH. 2006. The relationship between ambient air pollution and heart rate variability differs for individuals with heart and pulmonary disease. Environ Health Perspect 114: 560–566.
Zareba W, Nomura A, Couderc JP. 2001. Cardiovascular effects of air pollution: what to measure in ECG? Environ Health Perspect 109(suppl 4):533–538.
Zimmer AT. 2002. The influence of metallurgy on the formation of welding aerosols. J Environ Monit 4:628–632.
Last Updated: June 12, 2007
|
|
|
|
| |