 |
|
2004 Assisted Reproductive Technology (ART) Report: Section 2—ART
Cycles Using Fresh, Nondonor Eggs or Embryos |
|
This page contains figures 27–37
Section 2A | Section
2B | Section 2C
What are the success rates for couples
with male factor infertility when ICSI is used?
ICSI was developed to overcome problems with
fertilization that sometimes occur in couples diagnosed with male
factor infertility. In 2004, about 80% of couples diagnosed with
male factor infertility used IVF with ICSI.
Figure 27 presents the success
rates for these ICSI procedures among couples diagnosed with male
factor infertility. For comparison, these rates are presented
alongside the success rates for ART cycles that used standard IVF
without ICSI. This standard IVF comparison group includes couples
with all diagnoses except male factor. Because ICSI can be performed only when at least one egg has been retrieved, the live birth per
retrieval rates are presented.
In every age group, success rates for the IVF with
ICSI group were similar to the success rates for the groups that
used standard IVF without ICSI. These results show that when ICSI
was used for couples diagnosed with male factor infertility, their
success rates were close to those achieved by couples who were not
diagnosed with male factor infertility. Please note, however, that
review of select clinical records revealed that reporting of
infertility causes may be incomplete. Therefore, differences in
success rates by causes of infertility should be interpreted with
caution. (See
Findings from Validation Visits for 2004 ART Data for additional
information.)
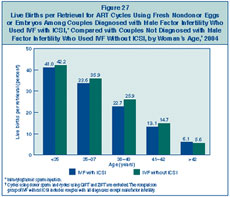
Figure 27: Live
Births per Retrieval for ART Cycles Using Fresh Nondonor Eggs or Embryos
Among Couples Diagnosed with Male Factor Infertility Who Used IVF with
ICSI, Compared with Couples Not Diagnosed with Male Factor Infertility
Who Used IVF Without ICSI, by Woman’s Age, 2004.
|
|
What are the success rates for couples
without a diagnosis of male factor infertility when ICSI is used?
As shown in Figure 26, a large number
of ICSI procedures are now performed even when couples are not diagnosed
with male factor infertility. Figure 28
presents success rates per retrieval for those cycles compared with ART
cycles among couples who used IVF without ICSI. For every age group, the
ICSI procedures were less successful. Please note, however, that review
of select clinical records revealed that reporting of infertility
causes may be incomplete. Therefore, differences in success rates by
causes of infertility should be interpreted with caution. (See
Findings from Validation Visits for 2004 ART Data for additional
information.) Additionally, information was not available to completely
determine whether this finding was directly related to the ICSI
procedure or whether the patients who used ICSI were somehow different
from those who use IVF alone. However, separate evaluation of various
groups of patients with an indication of being difficult to treat
revealed a pattern of results consistent with those presented below.
These difficult-to-treat groups included couples with previous failed
ART cycles, couples diagnosed with diminished ovarian reserve, and
couples with a low number of eggs retrieved (fewer than five). Within
each of these groups, ART cycles that used IVF with ICSI had lower
success rates compared with cycles that used IVF without ICSI.
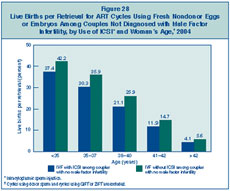
Figure 28: Live Births per Retrieval
for ART Cycles Using Fresh Nondonor Eggs or Embryos Among Couples Not
Diagnosed with Male Factor Infertility, by Use of ICSI and Woman’s Age,
2004.
|
|
How many embryos are transferred in an ART procedure?
Figure 29 shows that
approximately 52% of ART cycles that used fresh nondonor eggs or embryos
and progressed to the embryo transfer stage in 2004 involved the
transfer of three or more embryos, about 21% of cycles involved the
transfer of four or more, and approximately 7% of cycles involved the
transfer of five or more embryos.
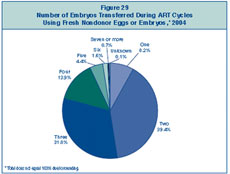
Figure 29: Number of Embryos
Transferred During ART Cycles Using Fresh Nondonor Eggs or Embryos,
2004.
|
|
In general, is an ART cycle more likely
to be successful if more embryos are transferred?
Figure 30
shows the relationship between the number of embryos transferred
during an ART procedure in 2004 and the number of infants born
alive as a result of that procedure. The success rate increased
when two or more embryos were transferred; however, transferring
multiple embryos also poses a risk of having a multiple-infant
birth. Multiple-infant births cause concern because of the
additional health risks they create for both mothers and
infants. Also, pregnancies with multiple fetuses can be
associated with the possibility of multifetal reduction.
Multifetal reduction can happen naturally (e.g., fetal death),
or a woman may decide to reduce the number of fetuses using a
procedure called multifetal pregnancy reduction. Information on
medical multifetal pregnancy reductions is incomplete and
therefore not provided here.
The relationships between number of embryos
transferred, success rates, and multiple-infant births are
complicated by several factors, such as the woman’s age and
embryo quality. See Figure 31
for more details on women most at risk for multiple births.
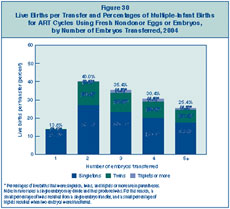
Figure 30: Live Births per Transfer
and Percentages of Multiple-Infant Births for ART Cycles Using Fresh
Nondonor Eggs or Embryos, by Number of Embryos Transferred, 2004.
|
|
Are live birth rates affected by the
number of embryos transferred for women who have more embryos available
than they choose to transfer?
Although, in general, transferring more than one embryo
tends to improve the chance for a successful ART procedure (see
Figure 30), other factors are also
important. Previous research suggests that the number of embryos
fertilized and thus available for ART is just as, if not more, important
in predicting success as the number of embryos transferred.
Additionally, younger women tend to have both higher success rates and
higher multiple-infant birth rates.
Figure 31 shows the relationship between the number of embryos
transferred, success rates, and multiple-infant births for a subset of
ART procedures in which the woman was younger than 35 and the couple
chose to set aside some embryos for future cycles rather than transfer
all available embryos at one time.
For this group, the chance for a live birth using ART
was about 45% when only one embryo was transferred. If one
measures success as the singleton live birth rate, the highest rate was
observed with one embryo transferred.
The proportion of live births that were multiple-infant
births was about 38% with two embryos and about 46% with three embryos.
Transferring three or more embryos also created an additional risk for
higher-order multiple births (i.e., triplets or more).
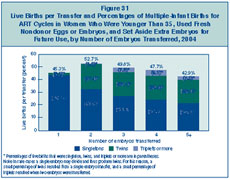
Figure 31: Live
Births per Transfer and Percentages of Multiple-Infant Births for ART
Cycles in Women Who Were Younger Than 35, Used Fresh Nondonor Eggs or
Embryos, and Set Aside Extra Embryos for Future Use, by Number of
Embryos Transferred, 2004.
|
|
How long after egg retrieval does embryo transfer occur?
Once an ART cycle has progressed from egg retrieval to fertilization, the
embryo(s) can be
transferred into the woman’s uterus in the subsequent 1 to 6 days.
Figure 32 shows that in
2004 approximately 72% of embryo transfers occurred on day 3. Day 5
embryo transfers were
the next most common, accounting for about 19% of ART procedures that
progressed to the
embryo transfer stage.
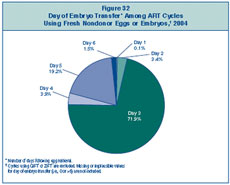
Figure 32: Day of Embryo Transfer
Among ART Cycles Using Fresh Nondonor Eggs or Embryos, 2004.
|
|
In general, is an ART cycle more likely to be successful
if embryos are transferred on day 5?
As shown in Figure 32,
in the vast majority of ART procedures, embryos were transferred on day
3 (72%) or day 5 (19%). Figure 33
compares success rates for day 3 embryo transfers with those for day 5
embryo transfers. In all age groups, the success rates were higher for
day 5 embryo transfers than for day 3 transfers. However, it should be
noted that day 5 embryo transfers may not be the best treatment option
for all patients undergoing ART because some embryos may not survive to
day 5.
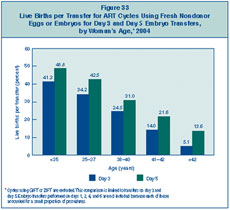
Figure 33: Live
Births per Transfer for ART Cycles Using Fresh Nondonor Eggs or Embryos
for Day 3 and Day 5 Embryo Transfers, by Woman’s Age, 2004.
|
|
Does the number of embryos
transferred differ for day 3 and day 5 embryo transfers?
Figure 34 shows the
number of embryos transferred on day 3 and day 5. Overall, fewer embryos
were transferred on day 5 than on day 3. Approximately 60% of day 3
embryo transfers and 25% of day 5 embryo transfers involved the transfer
of three or more embryos. The decrease in the number of embryos
transferred on day 5, however, did not translate into a lower risk for
multiple-infant births. See Figure 35
for more details on the relationship between multiple-infant birth risk
and day of embryo transfer.
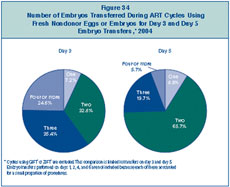
Figure 34: Number
of Embryos Transferred During ART Cycles Using Fresh Nondonor Eggs or
Embryos for Day 3 and Day 5 Embryo Transfers, 2004.
|
|
In general, how does the multiple-birth risk vary
by the day of embryo transfer?
Multiple-infant births are associated with greater problems for both
mothers and infants, including higher rates of caesarean section,
prematurity, low birth weight, and infant disability or death. Part A of
Figure 35 shows that among the
17,634 live births that occurred following day 3 embryo transfer, 69%
were singletons, 29% were twins, and about 3% were triplets or more.
Thus, approximately 31% of these live births produced more than one
infant.
In 2004, 6,297 live births occurred following day 5 embryo transfer.
Part B of Figure 35 shows that 37%
of these live births produced more than one infant (approximately 35%
twins and 2% triplets or more).
As shown in Figure 34, fewer
embryos were transferred on day 5 than on day 3. While the reduction in
the number of embryos transferred on day 5 was associated with a
decrease in triplet or more births, it also was associated with an
increase in twin births. Thus, the risk of having a multiple-infant
birth was higher for day 5 embryo transfers. Multiple-infant birth rates
for both day 3 and day 5 embryo transfers are much higher overall than
those found in the general U.S. population (about 3%).
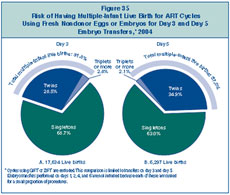
Figure 35: Risk of Having
Multiple-Infant Live Birth for ART Cycles Using Fresh Nondonor Eggs or
Embryos for Day 3 and Day 5 Embryo Transfers, 2004.
|
|
What are the success rates for women who use
gestational carriers?
In some cases a woman has trouble carrying a pregnancy. In such cases the
couple may use ART
with a gestational carrier, sometimes called a surrogate. A gestational
carrier is a woman who agrees to carry the developing embryo for a couple
with infertility problems (the intended parents). Gestational carriers were
used in 0.8% of ART cycles using fresh nondonor embryos in 2004 (710
cycles). Figure 36 compares success
rates per transfer for ART cycles that used a gestational carrier in 2004
with cycles that did not. In all age groups, success rates for ART cycles
that used gestational carriers were higher than success rates for those
cycles that did not.
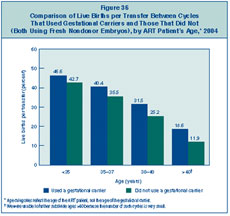
Figure 36: Comparison of Live
Births per Transfer Between Cycles That Used Gestational Carriers and Those
That Did Not (Both Using Fresh Nondonor Embryos), by ART Patient’s Age,
2004.
|
|
How is clinic size related to success rates?
The number of ART procedures carried out every year varies among
fertility clinics in the United States. In 2004, success rates were similar
for all clinics regardless of the number of cycles performed. For
Figure 37, clinics were divided equally
into four groups (called quartiles) based on the size of the clinic as
determined by the number of cycles it carried out. The percentage for each
quartile represents the average success rate for clinics in that quartile.
For the exact number of cycles and success rates at an individual clinic,
refer to the clinic table section of this report.
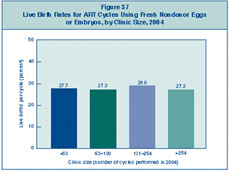
Figure 37: Live Birth Rates for
ART Cycles Using Fresh Nondonor Eggs or Embryos, by Clinic Size, 2004.
|
|
Section
1 | Section 2 |
Section
3 | Section 4 |
Section
5
Previous ART Reports
Implementation of the Fertility
Clinic Success Rate and Certification Act of 1992
Assisted Reproductive Technology: Embryo
Laboratory
Date last reviewed:
01/15/2007
Content source: Division
of Reproductive Health,
National Center for Chronic Disease
Prevention and Health Promotion
|
|
|