What seest thou else in the dark backward and abysm of time?
Shakespeare,
The Tempest
Beryllium is the fourth element in the periodic table and the second lightest metal known. Discovered as an oxide in 1798 by the French chemist L. N. Vauquelin, beryllium was first isolated in 1828, when it was called "glucinium" owing to the sweet taste of its salts. Beryllium is the lightest of all solid, chemically stable substances and has an unusually high melting point (1287°C). Silver gray and of low density (about one-third that of aluminum), with a close-packed hexagonal crystalline structure, beryllium metal has a very high strength-to-weight ratio. Although it is lighter than aluminum, it is 40% more rigid than steel. Beryllium has excellent electrical and thermal conductiveness but relatively pronounced brittleness, which restricts its applications.
Ubiquitous Beryllium
additive to glass, ceramic, plastics
aircraft engines and brakes
brass alloys
camera shutters
dental prostheses
electrical relays
golf clubs
gyroscopes
microelectronics
microwave devices
military vehicle armor
mirrors
missile guidance systems
nonsparking tools
nuclear reactors
pen clips
personal computers
precision instruments
rockets
satellites
springs
structural material in space technology
submarine cable housings
transistor mountings
wheels
x-ray tubes |
Principal uses of beryllium stem from the discovery in the 1920s that an addition of only 2% beryllium to copper results in an alloy six times stronger than copper. beryllium-copper alloys withstand high temperatures, are extraordinarily hard, resistant to corrosion, do not spark, and are nonmagnetic. These alloys are used in many critical moving parts of aircraft engines, in key components of precision instruments, electrical relays, and switches. Beryllium-copper hammers, wrenches, and other nonsparking tools are used in the petroleum industry where sparks from steel might cause explosions. In the electronics industry, including personal computers, Beryllium-copper alloys are found in integrated circuit sockets and electronic connectors. An alloy of 25% beryllium has some limited use in camera shutters. Beryllium-copper alloys are also used in golf clubs, springs, pivots, wheels, pinions, submarine cable housings, and dental prostheses.
Because of its low atomic number, beryllium is very permeable to X-rays. Its low neutron absorptance and high scattering cross-section make it a suitable moderator and reflector in structural materials within nuclear facilities. Beryllium metal can be used as structural material in space technology, in special windows for X-ray tubes, in gyroscopes, computer parts, and missle inertial guidance systems, as an additive in solid propellant rocket fuels, heat-sink material in high performance aircraft brakes, mirror components in satellite optical systems, and development of brass alloys.
Beryllium shares a number of chemical properties with aluminum. Upon exposure to air or water vapor, a thin film of beryllium oxide forms on its bare metal surface, rendering it highly resistant to corrosion, to hot and cold water, and to oxidizing acids. The ceramic properties of beryllium oxide make it ideal for production or protection of materials that are used at high temperatures in corrosive environments. Among its special applications are transistor mountings, semiconductor packages, and microelectronic substrates. Transparency to microwaves allow its use as windows, radomes, and antennae in microwave devices.
Beryllium's aerospace, nuclear energy, and military applications probably account for a paucity of reliable data on its production and consumption. Considerable fluctuations in its supply and demand result largely from variations in government programs in armaments, nuclear energy, and aerospace. Compared to available world production estimates of a dozen nations, the United States appears to be the largest producer of beryllium raw materials, with roughly 4339 tons produced in 1991. Russia is second, with approximately 1300 tons.
Warnings of Disease
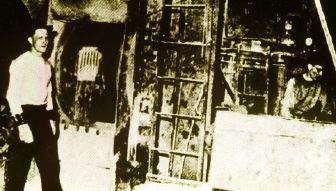 |
| Gross contamination. A beryllium sulfating mill in 1936 provided little protection for workers. |
The dermatological, pulmonary, and systemic toxicity of beryllium has been recognized only in the past 60 years. Although reports of beryllium-related lung disease resulting from inhalation of the metal during its extraction appeared in European and Soviet medical journals during the 1930s, these reports went generally unnoticed or disregarded in the United States. The role played by other chemicals, especially fluoride and oxyfluorides, was uncertain.
Gross contamination of equipment, work areas, and workers' clothing as well as open and unventilated tanks, alloy furnaces, and ore-sulfating ovens were typical of all three U.S. beryllium processing and production facilities throughout the 1930s and 1940s. Accidents and equipment failure were not uncommon, resulting in even greater exposures to beryllium oxide and hydroxide, as well as to beryllium's acid salts--sulfate, fluoride, and chloride. Skin contamination with beryllium splinters was commonplace among metal workers. From a number of rooftop stacks less than 40 feet above ground, beryllium effluent would blow toward residential areas.
In 1943, the first report was published in the United States on three cases of "chemical pneumonia" among Ohio beryllium extraction workers. This report, however, was overshadowed by NIH Public Health Service Bulletin No. 181 published in the same year, which asserted that beryllium was inert toxicologically and that any toxicity associated with beryllium usage could be attributed to other constituents of its compounds.
In 1946, cases of chronic beryllium disease (CBD) in the United States were suspected after instances of sarcoidoses (a disease characterized by nodules in the lungs) began occurring among fluorescent lamp manufacturing workers in Salem, Massachusetts. Zinc beryllium silicate was part of the phosphors in fluorescent lamps until 1949. Initially, four cases of Boeck's sarcoid, a chronic lung disease of unknown etiology, attracted attention because they were reported from a tuberculosis sanitorium in women who had worked previously in the same department of the same lamp factory. Thus, an occupational lung disease seemed more likely than tuberculosis, leading investigators to report on cases of "delayed chemical pneumonitis" among 17 more fluorescent lamp workers exposed to beryllium compounds. Still, doubt existed as to beryllium's role in the disease. Public Health Service scientists had failed to demonstrate toxicity in animals.
By 1947, more cases of both acute and chronic lung diseases were reported from U.S. Atomic Energy Commisssion laboratories as well as from additional lamp factories. By then, the AEC had become the major user of beryllium. By 1945, demand for beryllium in the United States created by the atomic bomb development program was about equivalent to total world demand up to 1940. A number of government laboratories had become involved in beryllium research during and immediately after World War II. Interest had expanded tremendously in military as well as civilian applications of beryllium.
From 1945 to 1950, when identification of beryllium as an occupational and environmental hazard led to control measures, acute and chronic beryllium disease occurred unchecked in the beryllium extraction, alloy, fluorescent lamp, and neon sign industries. By 1947, 40 cases of CBD, including 7 or more deaths, and about 500 cases of acute disease, with about 12 deaths, had been reported in the United States. At least 11 cases of nonoccupational CBD (also known as berylliosis) had been identified by AEC health and safety investigators among residents in the vicinity of the Lorain, Ohio, beryllium plant. One of these deaths from CBD was a homemaker, whose only exposure to beryllium occurred from laundering her husband's work clothes.
Through the auspices of its Health and Safety Laboratory located in New York, the AEC in 1947 began monitoring airborne beryllium concentrations and health hazards in and around the Lorain and Painseville plants near Cleveland. Merril Eisenbud, director of the AEC laboratory at the time, said "Both plants were having serious health problems, so management was extremely cooperative. A third plant near Reading, Pennsylvania, was also having a serious problem, but the management refused to acknowledge it was due to beryllium." This position, explains Eisenbud, was supported by Pennsylvania's Commissioner of Health, who agreed with the Public Health Service Bureau of Occupational Health that beryllium was not toxic. The AEC, he points out, had no legal basis for its monitoring mission, "and so the two Ohio plants and the surrounding communities became our field labs. Information from the Pennsylvania plant was incorporated when it became available."
Acute Disease
Although few quantitative data exist on exposure to beryllium before 1947, data gathered by the International Agency for Research on Cancer between 1947 and 1948 leave little doubt that extremely high concentrations were encountered in the workplace. In U.S. beryllium extraction facilities, concentrations greater than 1000 micrograms per cubic meter (µg/m3) were not uncommon. Exposures measured late in 1946 using the filter-paper dust sampler method ranged from 110 to 4710 µg/m3 in an extraction plant's furnace area. Concentrations of 590-43,300 µg/m3 were monitored by AEC investigators in the Lorain, Ohio, plant in 1947-48.
Prevalence estimates of acute beryllium disease in workers ranged as high as 7% in the early literature. Caused mainly by dusts or fumes of soluble beryllium salts released during the extraction of beryllium hydroxide and production of beryllium oxide and metallic beryllium, two types of acute beryllium disease have been described clinically; their progression is either rapid or slow. A "fulminating" or rapid type develops within 72 hours of massive exposure, while an "insidious" version develops several days or weeks after exposure to lower concentrations of beryllium salts or low fired oxide. Common clinical signs include shortness of breath on exertion; a nonproductive, often paroxysmal, cough; chest pain; acrocyanosis (persistent discoloration of fingers, hands, toes, and feet, accompanied by cold and sweaty fingers and toes); sibilant rales over the lung bases (asthmalike hissing sound); and a sudden, marked drop in vital capacity. Rapid heart rate, weight loss, and anorexia might also occur. Death occurs in 10% of the cases, nearly all the fulminant type. Those with insidious-onset acute disease typically recover in one to three months, but in some cases recovery may take as long as six months and there's a risk of longer-lasting respiratory problems. Approximately 17% of workers with acute disease subsequently develop CBD.
In 1949, Eisenbud and his AEC associates recommended occupational and community ambient air standards for beryllium that remain intact today, adopted by OSHA. For occupational air exposures, a permissible level of 2.0 µg/m3 was established based on an 8-hour time-weighted average. A 30-minute maximum peak level was set at 25 µg/m3. Beryllium concentrations in air surrounding the factories is not to exceed 0.01 µg/m3. The latter air standard became the first ambient air quality standard in the United States, and it preceded all others by about 25 years.
Subsequent studies on the epidemiology of beryllium disease revealed these standards were effective in eliminating most acute lung disease. The U.S. Beryllium Case Registry (BCR), established in Massachusetts in 1952 and now maintained by NIOSH in Cincinnati, collects data on the epidemiology, diagnosis, clinical features, course, and complications of beryllium-related diseases, including cases of acute beryllium-related pneumonitis and chronic beryllium-related nonmalignant lung disease. Individuals referred to the BCR for evaluation of beryllium-related diseases were employed in a variety of occupations, but most have worked in beryllium extraction and smelting, metal production, and fluorescent tube production.
The BCR has admitted only 15 cases of acute disease since 1950. Some individuals may have developed a less severe, subacute form of the chemical pneumonitis due to beryllium exposure and were misdiagnosed as having a viral or other pulmonary infection. The potential for acute disease due to accidental exposure to high concentrations remains despite improvements in workplace ventilatory controls.
In 1983, Eisenbud, who became director of New York University's Institute of Environmental Medicine, and co-author Judith Lisson, a NIOSH epidemiologist, reviewed the BCR's 224 acute and 622 chronic cases, which include 65 CBD cases attributed to ambient air pollution in the vicinity of beryllium plants or to dust brought home on work clothes. An additional 45 CBD cases, along with a dozen acute reports not included in the BCR, were also examined. The authors observed a "striking reduction" in the number of CBD cases among workers first exposed after the 1950s, with no case reported for an individual first exposed after 1972. According to Eisenbud and Lisson, exposure control methods adopted in the 1950s accounted for these reductions despite a marked increase in the use of beryllium. However, in light of more recent research and clinical developments, the impact of beryllium control standards on the incidence of CBD is much less certain.
Misclassifications and Populations at Risk
 |
| Pebbles and Bam-Bam. Beryllium nuggets are melted down for use in products including nuclear reactors. |
It is generally agreed that the epidemiology of CBD has been limited by misclassification of the disease and of exposure status in the BCR. Until 1970, entry into the BCR was based on two criteria: significant exposure to beryllium and evidence of chronic lower respiratory tract disease. Chronic beryllium disease was initially confused with sarcoidosis, from which it was clinically indistinguishable before the advent of current immunologic tests. Some cases of CBD may have been excluded from the BCR, and some cases of sarcoidosis may have been erroneously included. Thus, limited conclusions can be drawn from published studies in the 1950s and 1960s regarding the prevalence of beryllium disease. Estimates of CBD prevalence in most series range from about 2 to 5%.
The size of the population at risk is unknown, with estimates of the number of U.S. workers exposed ranging from 30,000 to 800,000, which includes more than 20 industries and trades in which there is potential exposure to beryllium. Summarizing data on occupational exposure to beryllium for the period 1 June 1979 to 31 January 1984, based on inspections of workplaces, OSHA found levels in excess of 2 µg/m3, mainly in the traditional beryllium industry, but also in high-technology industries (semiconductor, precision electronics, spacecraft, and missile manufacture industries).
CBD Reconsidered
In its early stages, CBD may be completely asymptomatic, as observed in apparently healthy individuals with lung X-ray abnormalities. In other cases, CBD may begin with nonspecific respiratory symptoms, including mild shortness of breath and cough, but no recognizable changes on chest films. Gradually, the majority of patients develop symptoms more characteristic of chronic disease: cough, burning chest pain, progressive shortness of breath (dyspnea) with exertion, weakness, fatigue, dyspnea at rest, and, characteristic of advanced disease, anorexia, weight loss, acrocyanosis, and clubbing of finger and toe bones. Signs of right heart failure and cor pulmonale (enlargement and strain of the right side of the heart due to increased pressure in the pulmonary artery from lung damage) may also be detected in advanced cases.
CBD's clinical course is extremely variable. Some individuals remain stable for many years, others progress more precipitously, developing severe respiratory symptoms within a few months. The majority experience a slow, inexorable decline in pulmonary function. Mortality from CBD occurs in an estimated one-third of cases.
 |
| Lee S. Newman--The chronic form of beryllium disease is far from extinct. |
"Most clinicians are taught that beryllium disease is a dinosaur," states Lee S. Newman of the Occupational and Environmental Medicine Division, National Jewish Center for Immunology and Respiratory Medicine, in Denver. "But the chronic form of the disease is far from extinct. In fact, with increasing usage of beryllium in industry, the absolute number of cases can be expected to increase as well."
Newman points out that even with careful ventilatory controls and monitoring, CBD continues to occur because it is due to a hypersensitivity to beryllium, in which an antigen-specific immune response plays a central role in pathogenesis. Exposed individuals become sensitized to beryllium and accumulate pathologic clusters of cells called granulomas around beryllium particles in the walls of alveoli. "Such hypersensitivity can develop in some individuals following even low-level exposures well within permissible exposure limits," Newman explains.
Indeed, the original theory that CBD was a delayed chemical pneumonitis due to direct toxicity was problematic. Beryllium levels in tissue did not correlate with the presence of CBD, nor did disease incidence correlate with exposure history; the majority of workers with high exposures never developed disease, while some with seemingly low or minor exposures developed severe disease, as did others whose duration of exposure was relatively brief.
As early as 1951, Eisenbud and others proposed that CBD was immunologically mediated, a proposition that became more valid that same year when skin-patch testing with beryllium salts demonstrated that beryllium could be sensitizing. In 1959, biopsies of patch test sites after 6 weeks demonstrated the presence of epithelioid cell granulomas, further evidence of a cell-mediated immunologic response. More recently, laser microprobe mass spectrometry has identified beryllium in these lesions.
In vitro lymphocyte proliferation testing has been applied since the 1980s to beryllium disease. Lymphocytes from individuals sensitive to beryllium proliferate extensively. Blood cells drawn peripherally, or lung cells retrieved via intranasal insertion of a bronchoscope into the lung, are cultured in the presence of beryllium salts. Using a radiolabeled DNA precursor such as thymidine, a determination of the cells' level of radioactivity provides an index of proliferation. Studies show proliferation testing is a specific and sensitive indicator of the cell-mediated immune response to beryllium. The less invasive peripheral blood test allows screening for beryllium sensitization and early CBD among beryllium-exposed workers and offers a reliable method for differentiating CBD from sarcoidosis. However, no consensus exists on whether the patch test or proliferation test is the best for CBD diagnosis or surveillance screening.
Newman and his Denver colleagues have used blood proliferation testing in epidemiologic studies of beryllium workers in Colorado at the Rocky Flats nuclear weapons plant and at a beryllium ceramics company. They've noted that about 2% of all beryllium-exposed workers who have volunteered for testing are either sensitized to beryllium or have evidence of CBD. A DOE screening program for all current and former Rocky Flats workers, now in its second year, is confirming that percentage.
"Some people who haven't been exposed in over 30 years now have beryllium disease, with symptoms manifested very recently. So it seems latency has a range from a few months up to 30 or more years," said Newman. "We don't truly know the latency for either beryllium sensitization or beryllium disease. We don't actually know how long it takes from the time you're exposed to the time you first become sensitized, nor do we know the length of time it takes from sensitization to development of granulomas or other lung function reactions to beryllium. Despite what is in the literature, we truly don't know."
According to Newman, about half of those who are simply sensitized without disease will develop pulmonary granulomas, most doing so within three to four years of sensitivity testing. Another subset of individuals followed for six years has not developed any sign of disease nor developed lung granulomas. "It's possible that some who become sensitive to beryllium may never develop the disease. Only a longitudinal study will answer that question," said Newman.
"There's a wide spectrum of severity and rate of disease progression," Newman continues. "It's becoming clear that CBD is a disease that results from at least two hits: there may be an element of individual genetic risk and the element of exposure."
In terms of exposure, Newman believes that the Rocky Flats and beryllium ceramics company studies contain findings that suggest a challenge to the "old immunologic dogma of no dose-response relationship in CBD." While several CBD cases were associated with trivial or unrecognized beryllium exposure (a secretary, a security guard at Rocky Flats; a sweeper with the ceramics company), there were also CBD rates higher than 2% in both workplaces--15.8 percent in some jobs--among work groups with presumed greater beryllium exposure: beryllium machinists, workers with sawing tasks, metallurgical operators, chemical control operators, beryllium dry pressers, and those involved in beryllium process development/engineering.
For Newman, the implications are clear: further control of the amount of exposure and kind of exposure will lower beryllium disease rates. "So there is a place for improved industrial hygiene and primary prevention here," he said. Moreover, in terms of secondary prevention, Newman recommends broad-based medical surveillance with the beryllium lymphocyte proliferation test in all beryllium-using industries, in conjunction with chest X-rays, to identify sensitivity and subclinical disease among former and current workers. Those identified as such should be enrolled in research follow-up for defining a prognosis and in clinical intervention trials. As to a consensus on frequency of surveillance, that too remains to be reached.
The Cancer Connection
Four IARC working groups (1972, 1980, 1987, 1993) have carefully sifted through and interpreted animal and epidemiologic data on beryllium's potential as a human carcinogen. The first group considered the four epidemiogical studies available at that time to be inadequate to evaluate the human carcinogenic effects of beryllium. In the 1980 evaluation, IARC concluded that beryllium and its compounds are carcinogenic in rats, rabbits, and monkeys. IARC also concluded that lung tumors had been produced in rats and monkeys by inhalation or intratracheal exposure to many beryllium metals, sulfates, and alloys.
The 1980 IARC working group also reviewed four epidemologic cohort studies and concluded that the evidence for an increased risk for lung cancer from occupational exposure to beryllium was limited. No new study was available at the time of the third review; however, on the basis of evidence of carcinogenicity of some beryllium compounds on the above three species of animals, IARC stated that beryllium should be considered a suspect carcinogen to humans.
A 1991 study of workers enrolled in the BCR by NIOSH epidemiologists Kyle Steenland and Elizabeth Ward, found an excess risk of lung cancer two times greater than normal, which was most pronounced among workers with acute disease.
In a 1992 evaluation of the mortality experience of workers exposed to beryllium, Ward and her NIOSH associates reported results of a cohort study of 9225 male workers employed by two companies at seven beryllium plants in Ohio and Pennsylvania. A total of 280 cancers were observed, versus 221.5 expected based on U.S. rates. In this study, however, the population was not drawn from the BCR but from personnel records matched against records of individuals from the Social Security Administration. These were obtained from the study plants for all quarters from 1940 through 1967. Vital status of all workers in the study was determined as of 31 December 1988 from the Social Security Administration, IRS, post office cards mailed to the last address, Veteran's Administration records, the Health Care Financing Administration, and the National Death Index. Death certificates were obtained from state vital statistics offices.
Significant excess mortality rates for lung cancer were observed from two of the oldest plants located in Lorain, Ohio, and Reading, Pennsylvania. Lung cancer mortality rates did not increase with longer duration of employment, but did increase with longer latency (time since first exposure). Lung cancer was particularly elevated among workers at the Lorain plant with a history of acute beryllium disease. However, this lung cancer excess was not restricted to plants operating in the 1940s. Elevated rates were also observed for four of the five study plants that operated in the 1950s for workers hired during that decade.
Decade of hire was one of the strongest correlates of lung cancer mortality in the total cohort. The IARC working group noted that, given the much higher exposures to beryllium before 1950, and the fact that 73% of the cohort worked for less than five years, duration of employment did not separate that segment of the cohort that received the highest exposures to beryllium.
In their summation of the human carcinogenicity data, the IARC working group said it was satisfied that cigarette smoking was not a confounding factor and that it did not appear to explain the increased lung cancer risk. However, the group did point to aspects of the 1991 and 1992 studies that would limit the interpretation that occupational exposure to beryllium compounds is the "most plausible explanation" of the increased lung cancer risk observed. These included absence of any individual measurements of exposures to beryllium, relatively low excess risk for lung cancer, and absence of any mention of exposure of workers to other lung carcinogens in the workplace (although the working group stated it saw no evidence that other carcinogens were present). Still, upon scrutinizing the experimental and epidemiological evidence, IARC decided there was sufficient evidence for both animal and human carcinogenicity of beryllium.
 |
| Carl Shy--A pattern of excess lung cancers indicates a link between exposure and disease. |
Commenting on the relatively small excesses of lung cancer deaths observed, Carl Shy, professor of epidemiology at the University of North Carolina, and a member of the fourth IARC Working Group, says, "We have to look at the whole pattern, the consistency of the evidence, to say there's likely to be a relationship between exposure and disease. If it were a chance relationship, you wouldn't expect to find a pattern of excess as has been demonstrated here."
In the face of the IARC decision, controversy continues. The beryllium industry contends that the oncogenicity of beryllium compounds has not been unequivocally established and that environmental exposure controls in the workplace reduce whatever risk may exist to negligible levels. Industry scientific advisers have also put forth the possibility that inhalation exposure to acid mists resulting from the sulfate ore extraction process may account for excess lung cancer observed in the NIOSH studies. According to Ward and Steenland, however, such exposure would usually be accompanied by an increase in laryngeal cancer, which hasn't been demonstrated in beryllium studies. They say a paucity of monitoring information makes it difficult to determine if the acid mist levels at plants using ore sulfating were high or low and how widespread they were within these plants. (Apart from the Lorain plant where the highest excess of lung cancer was found, a sulfating process was also used at three plants that began operating after the 1950s.) In any event, the beryllium industry must comply with OSHA's Hazard Communication Regulation that warning labels and material safety data sheets to employees and customers must state that beryllium is a human carcinogen. In addition, NIOSH must notify current and former beryllium industry employees that they may have been exposed to cancer-causing substances in the workplace.
An upcoming conference on beryllium-related diseases co-sponsored by NIEHS, DOE, OSHA, and NIOSH is scheduled. Meanwhile, general agreement seems to exist on both sides of the cancer argument that the issue of CBD is of far greater magnitude and significance. Indeed, it may well be that any future OSHA proposals to lower current occupational beryllium exposure standards would be determined more by concerns over CBD than cancer. Peter Infante, who directs the Office of Standards Review at OSHA, says he believes there will be more cases of CBD than lung cancer from low-dose beryllium exposures. "The issue, in my opinion now, is how are we going to prevent these people from getting chronic beryllium disease? Cases are being recognized at very low exposures. That's the challenge."
A Genetic Test for Beryllium Disease
 |
| Martin Powers--Keeping susceptible people out of the beryllium industry is intelligent and sensible. |
The advent of a genetic screening test for CBD is viewed by some individuals associated with the beryllium industry like the proverbial light at the end of the tunnel, a way to eventually eradicate CBD from the workplace. Martin Powers, former vice president of Brush-Wellman, Inc. (the world's largest beryllium processor and producer), and now executive director of BISAC, the Beryllium Industry Scientific Advisory Committee, says "For years we've been searching for this, trying to find people who were susceptible so we could, in effect, protect them or take them out of the industry. If we could take that small percentage and screen them out, we could eliminate disease, eliminate the marketing problem that comes with having a toxic material, and we could begin doing away with some of those very expensive control measures." Genetic screening, however, raises ethical concerns about workplace discrimination such as who will make these decisions and how such decisions will affect a worker's ability to obtain health insurance or other employment.
Last October in Science, researchers from Italian universities in Rome and Modena, partially supported by a grant from BISAC, described for the first time a genetic marker for CBD. The authors, Luca Richeldi, Rosa Sorrentino, and Cesare Saltini, presented evidence that a small difference in the genetic sequence in the major histocompatibility complex (MHC) allele, HLA-DPB1, identifies people at increased risk of developing CBD if exposed to beryllium. They observed that 32 of 33 occupationally exposed workers with CBD exhibit the amino acid glutamate in a potentially critical location (position 69) in a cell-surface glycoprotein of MHC HLA-DPB1, which may participate in antigen recognition. Of a control group of 44 beryllium-exposed workers without CBD, 70% did not have glutamate in this position.
Because lymphocyte proliferation tests neither predict beryllium disease nor its risk, Richeldi and his co-authors see a possible role for the genetic marker in association with lymphocyte testing to identify and follow-up persons at risk for beryllium disease. Newman concurs. He says the addition of a genetic marker would allow employers to potentially reduce beryllium exposure for high-risk individuals and more effectively target them for intensified medical monitoring and early disease detection.
Commenting on their findings, however, Newman states we have a lot to learn about the interaction between exposure to beryllium and inheritance of the marker. He also states that it's premature to advocate that employers deny or discourage employment of workers with genetic risk of CBD. Social and ethical issues need consideration. And given that almost all people in the study with CBD have the marker, while many without CBD also have the marker, only a population-based investigation can answer the questions that are necessary for designing a genetic screening test: What proportion of employees with the marker will develop the disease, and what proportion of workers with the marker will not? "Even if most CBD patients test positive for the marker, it may not be helpful to identify up to 30% of the potential workforce as at risk if the prevalence of CBD among beryllium-exposed workers is only two to five percent," said Newman.
Chronic beryllium disease may eventually have the distinction of becoming the first model for assessing the value of genetic testing in preventing occupational disease. However, the possibility of genetic screening in the workplace is already raising concerns that go beyond science. Current screening programs for beryllium sensitization and disease have created issues surrounding worker compensation for occupational disability and insurance. Because there is currently no way to accurately predict the natural course of CBD, questions have been raised about whether former or current workers who've been defined as having subclinical disease would qualify for occupational disability, compensation for health care costs, and lost income.
 |
| Anthony Mazzocchi--The question of worker compensation has to take on a very broad character. |
"I think the whole question of compensation has to take on a very broad character," says Anthony Mazzocchi of the Oil, Chemical and Atomic Workers Union. "There's a responsibility on the part of government and employers for continuing medical surveillance and treatment of workers, and to follow this population for life."
For some, the concerns take on major societal implications if genetic testing is used for pre-employment worker selection. Sheldon W. Samuels, executive vice president of The Workplace Health Fund, says the purpose of the international beryllium industry's support of a genetic testing research program "is to defend what they have already proclaimed oxymoronically as the discovery of the 'first occupational genetic disease'. One overt purpose of the research, as stated before witnesses, is to establish a case for the exclusion of purportedly defective workers from employment on the basis of a genetic difference."
Samuels sees this as a harbinger of an eventual caste system created by industry and warns that genetic screening, like any other kind of screening, has the potential for unjust application and shortsighted social policy. "Marketplace corporate policies could create a caste of susceptibles, of socially defined lepers," he said.
According to Samuels, given computerization and existing international records linkage, woefully inadequate provisions for protecting worker confidentiality, poorly regulated informed consent, and the ease of implementing widespread testing, a specter has been raised of a bleak tomorrow, one in which many thousands of workers would be tagged for life, and their offspring tagged as well, as insurance, employment, and perhaps even mating risks. Says Samuels: "Industrial genetic screening should only take place in a society that has created a system of screening within neutral community structures that economically and socially protect the individual and family before, during, and after a voluntary, confidential counseling process. It must not take place in the coercive milieu of the typical industrial setting."
Powers says he is not persuaded by the social argument and is astounded by objections to screening people. "The worker is entitled to a clean workplace. The employer should provide it. But the facts are that the beryllium industry hasn't been able to do it completely. Keeping susceptible people out is intelligent and sensible. The beryllium industry is one industry where a good faith effort has been made even before it was legally required to get exposures down to a safe level. But we're still getting [CBD] cases in the plants. The beryllium employer cannot guarantee a safe workplace. It seems almost criminal to give people the right to go in there and get sick if they want to."
Yet Samuels envisions another reason behind the industry's interest in a molecular biological research program. The program may be used to successfully marshall data for use against all claims for compensation on health care costs and income replacement, and against calls for more stringent environmental protection. Samuels says the laws of most states archaically assume a "single cause" in cases of workers' compensation for occupational disease. Thus, reasons Samuels, the hypothesis of CBD being caused by a defective worker, rather than a defective workplace, would be an economically appealing defense for an industry no longer protected by government, as it once was during the nuclear arms race, and which must now confront the recent IARC classification of beryllium as a human carcinogen. This classification, which may carry more weight in Europe than in the United States, might have implications for continued use of beryllium-copper alloy in certain industries where it can be replaced.
Few would doubt that improved industrial hygiene standards for beryllium have prevented many cases of beryllium disease. But total compliance with a peak standard is difficult in this industry; equipment malfunctions, accidents, start-up problems, and new employee inexperience can all contribute to significant deviations beyond allowable air concentrations. It seems that disease is likely to occur even when current exposure standards are maintained, yet it remains unknown whether more stringent allowable exposure levels would prevent sensitization, chronic beryllium disease, or cancer.
Leslie Lang
Leslie Lang is a freelance writer in Chapel Hill, North Carolina.
Last Update: July 30, 1998