Curator's Corner
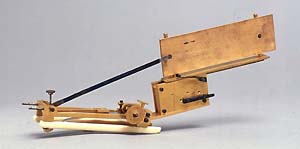
The Mahomed sphygmograph pictured above is included in the exhibition, Changing the Face of Medicine, Celebrating America's Women Physicians. Mary Putnam Jacobi, a physician featured in the exhibition, used a Mahomed sphygmograph to write her 1876 essay, "The Question of Rest for Women during Menstruation." In this influential paper she refuted the supposed physical limitations of women, an argument defined by Dr. Edward H. Clarke's publication Sex in Education; or, A Fair Chance for the Girls (1875). Using the scientific method to gather and evaluate evidence, Dr. Jacobi provided tables, statistics, and sphygmographic tracings of pulse rate, force, and variation to illustrate the stability of a woman's health, strength, and agility.
Illustration of a sphygmograph in motion created for Changing the Face of Medicine: http://www.nlm.nih.gov/exhibition/changingthefaceofmedicine/artifact/jacobi.html
The sphygmograph was at its peak of popularity in the mid 1800s, and was seen as a technical marvel by physicians and scientific researchers. Examine the following sections to learn about the history of the sphygmograph, and to see historical accounts and images of how it works, and what the tracings mean.
What is a sphygmograph?
Invented in the middle 1800s, and continually improved over the next 50 years, the sphygmograph allowed physicians to measure the pulse, and most importantly, to record it. Previously the pulse was measured by placing fingers on the wrist of the patient and applying pressure. The sphygmograph was a first step in standardizing the recording and evaluation of pulses using technology.
A sphygmograph provides a recording of the movement, form, and force of the pulse. The pulse is the rhythmic changes in diameter of an artery due to increases and decreases of blood volume passing through the artery as the heart pumps. The pulse is felt on any artery when the artery is compressed over a bone or firm tissue. The sphygmograph has a light plate which compresses the artery in the wrist against the bone. With each pulse, the plate moves up and down. This movement is amplified and etched onto a piece of smoked paper, resulting in a line with a series of peaks and valleys. This is referred to as a sphygmograph tracing.
Physicians used these tracings to view any irregularities in the pulse. As more recordings were made, physicians looked for similarities among patients with known conditions to see how these conditions were affecting the pulse. The resulting catalog allowed physicians to use pulse recordings as a diagnostic tool. Sphygmographs were also used to evaluate the general condition of patient, as a strong pulse was viewed as a sign of good health.
Etienne Jules Marey, a French physician who was interested in the visual representation of data, invented the first widely used sphygmograph in 1860. In 1872 physician F.A. Mohammed improved upon Marey's device by adding a wheel to adjust the downward pressure of the plate upon the artery in measurable increments. This improved standardization of the measurements taken, as it allowed the physician to apply the same pressure for every patient, as well as fine-tune readings for a specific patient or condition.
While the sphygmograph went a long way towards standardizing the measuring of the pulse, it never replaced palpation—the measurement of the pulse by touch. Many physicians preferred, and trusted, their own senses. The sphygmograph was difficult to use, and at times unreliable. It often produced inaccurate results if not carefully set up. As research into blood pressure rather than pulse progressed, devices such as sphygmomanometers overshadowed the sphygmograph.
How does a sphygmograph work?
The Mahomed sphygmograph in the exhibition improved upon the widely used Marey sphygmograph. The first historical account presented here is a step by step description of how the Marey sphygmograph works. The second historical account deals with the Mahomed model and its improvements.
Marey Sphygmograph
The following text and accompanying diagram are taken from the Handbook of the Sphygmograph: Being a Guide to its Use in Clinical Research by J. Burdon Sanderson, M.D. F.R.S. This book was published in 1867 by Robert Hardwicke, London, and is located in the History of Medicine Division collection, call number WBB B 949h 1867.
"In the sphygmograph of Marey, the movements recorded are not those of the artery, but those of an elastic tongue of steel which presses upon it. This spring is screwed, at the end opposite to that which is applied to the artery, to a frame of brass, which is maintained in a fixed position as regards the radius, so that the pressure exerted by the spring is continuous and constant. It is manifest that, inasmuch as the spring depresses the surface of the artery, its movements are not identical with those of the arterial wall; hence the extent of motion is inaccurately measured. As, however the duration of each motion can be determined with extreme precision by Marey’s instrument, it must be regarded as superior to any other which has been proposed, notwithstanding the defect above referred to."
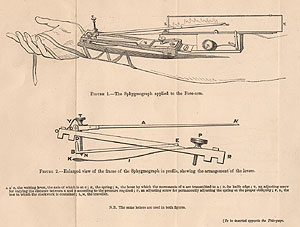
Labeled diagram of a sphygmograph as described below from Handbook of the Sphygmograph: Being a Guide to its Use in Clinical Research by J. Burdon Sanderson, M.D. F.R.S.
The sphygmograph "is secured in its position by a bandage passed around the wrist, and laced alternately from side to side round little hooks, which are arranged along the edges of the metal wings, attached by hinged joints to the opposite sides of the instrument. In the interior of the framework, D R (fig 2), seen in profile in the figure, is a flexible steel spring which descends obliquely, and is covered at its extremity by a plate of ivory, K. When the instrument is used, this plate rests upon the artery, which depresses by virtue of the elasticity of the spring. This being the case, each pulsation communicates slightly to the plate. To amplify these movements, a light wooden lever, A A', of the third order, is used, which is supported by steel points at C. B E is a second lever of the same order, which has its centre of movement at E. It terminates at D, in a vertical knife edge, and is traversed by the vertical screw, T. When the extremity, N, of the screw rests upon the spring above the ivory plate, every movement of the pate is transmitted to B E, and by means of the knife edge to the wooden lever, A A'. The purpose of the screw, T, is to vary at will the distance between the wooden lever and the upper surface of the spring, without interfering with the mechanism by which the movement is transmitted. As the distance between C and D is much less than they length of the lever, the oscillations of its extremity, A', are much more extensive than the vertical movements of the spring. The lever ends at a in fig. 1, in a pen of peculiar form, which writes on a slip of glazed paper supported on a metal frame. This frame moves by clockwork from M towards L, the rate of movement being such that about three inches are traversed in the tenth of a minute."
Mahomed sphygmograph
The following description and image of the Mahomed sphygmograph are taken from the Manual of the Physical Diagnosis of Diseases of the Heart Including the Use of the Sphygmograph and Cardiograph. This book was published in 1881 by J. & A. Churchill of London, and is in the History of Medicine Division collection, call number WG S229L 1881.
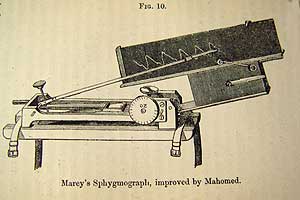
Figure 10 from the Manual of the Physical Diagnosis of Diseases of the Heart Including the Use of the Sphygmograph and Cardiograph
Mahomed's sphygmograph (fig. 10) consists essentially of a framework containing an arrangement of levers adaptable to the pulsating vessel. Contact with the artery, the radial being usually chosen for convenience, is made by a mainspring, the movements of which, consentaneous with those of the artery on which it is made to rest, are communicated to a lever of the third order, so that the slight motion may be much amplified (about ninety times). The writing lever consists of a fine slip of very light wood, and is so guarded as to allow vertical without lateral movements. The motions of the pulse are thus converted into up-and-down strokes of the free extremity of the lever; these are made to impinge upon a slide, which, by means of clockwork, is caused to travel at a known rate-about four inches in ten seconds. Thus movements of the free extremity of the lever, representing the amplified movements of the pulse, are described upon the traveling slide in a series of figures…
An essential point is to be able to apply the main—spring to the artery with definite degrees of pressure. This object Dr. Mahomed has attained with great success. By a very ingenious arrangement the pressure can be increased by turning a thumb-screw, and the pressure is measured in ounces (1 to 18 troy) upon a dial-plate.”
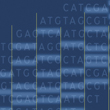
What do sphygmograph tracings show?
The following description and accompanying diagram are taken from the On the Use of the Sphygmograph by Balthazar W. Foster, M.D., F.L.S. This book was published in 1866 by John Churchill & Sons, London, and is located in the History of Medicine Division collection, call number WBB F754o 1866.
In describing the different sections of a tracing, the author is making a case for the usefulness of the instrument. Differences in the amplified illustration of the regularity and force of the pulse as shown in the tracing, can be compared between patients or in a series of tracings for one patient.

a typical sphygmograph tracing, from On the Use of the Sphygmograph by Balthazar W. Foster, M.D., F.L.S.
The sphygmograph, when in action, enables us to obtain an exact reproduction on paper the pulse form; it also tells us the frequency of pulsations and their regularity. It enables us, in addition, to see at a glance any peculiarity in the entire series, or in any single pulsation. A trace is composed of a series of curves, each of which corresponds to a complete revolution of the heart, and is called a pulsation. Each pulsation is composed of three parts: the line of the ascent, the summit, and the line of descent.
The line of ascent is caused by the flow of blood into the arterial system after each cardiac systole; and tells us, by its form the manner in which the blood enters the vessel. The more rapid the afflux, the more quickly the pressure in the arteries will be elevated, and the more vertical will be the ascent of the lever. When the entry of the blood is slow, the line of ascent will be traced by the lever obliquely, sometimes in curved form. The line of ascent, in certain morbid conditions, exhibits a mixed form—the first part of the trace being vertical, the latter part curved.
The summit of the pulsation corresponds to the duration of the arrival of blood in the artery, and designates the period during which the entrance balances the outward flow-in other words, the afflux and efflux are exactly equal. This period varies in length; it may be so short, that the summit becomes a mere mathematical point between the lines of ascent and descent, or it may be so long as to render the summit a horizontal line of some length. In the latter case the lever traces the horizontal line, whilst the entry of blood into the vessel and its passage onwards mutually balance one another, and this line indicates the duration of the cardiac systole. The summit of the pulsation, when of any length, is not always horizontal; it may be formed by an ascending or descending plane, according as the afflux predominates over the onward flow, and vice versa. In some cases a little hooked point may precede the summit; and this is a very valuable diagnostic element in the trace, as we shall see further on.
"The line of descent corresponds to the fall of the pressure in the arterial system , and is synchronous with the interval between the closure of the sigmoid valves and the next ventricular contraction. This line, by its obliquity, marks the celerity of the fall of the pressure within the vessels, and indicates the facility with which the blood passes on its course. The frequency and amplitude of the pulse are pointed out by the obliquity of this line. The form may vary very much; sometimes it is purely oblique, at others a curve convex upwards, and occasionally one or more undulations may be seen in it. The last peculiarity is often very marked, and in some cases is perceptible to the finger; it has been termed dicrotism. By this term, we should only understand undulations occurring in the descent. Similar peculiarities have been pointed out in organic diseases of the heart; but in these cases the dicrotism belongs to the period of ascent, and is due to very different causes. The sphygmograph here gives us valuable aid; for it enables us to recognize in which period the peculiarity occurs."
In his description of sphygmograph tracings Dr. Foster goes decribed looking for regularity among a series of pulses. "In examining a pulse-trace, one should note, in addition to the form of each pulsation, whether the summits of al of them can be joined by a straight line, and whether the bases can also be connected by a similar line parallel to the former. In some instances, this ceases to be the case, and a series of pulsations cannot be contained between such imaginary lines. The pulsations become irregular, and the line to join their summits or bases must cease to be straight."
Dr. Foster also notes that because the plate with the tracing on it moves at a uniform ten seconds, one can accurately examine and then compare frequency of the pulse.
Click the image to see detail.
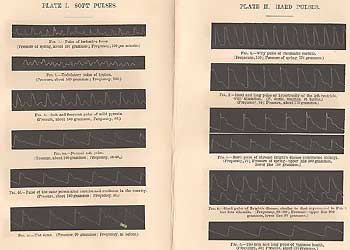
A series of sphygmograph tracings from Handbook of the Sphygmograph: Being a Guide to its Use in Clinical Research by J. Burdon Sanderson, M.D. F.R.S. Each pulse is listed along with a description, associated with either an activity or a medical condition.