PDF Version: http://aspe.hhs.gov/daltcp/reports/2007/07alcom1.pdf (61 PDF pages)
This compendium describes regulatory provisions and Medicaid policy for residential care settings in all 50 states and the District of Columbia. It updates an earlier report completed in 2005 with data for 2004.
The original intent for this edition of the compendium was to provide data for 2006. However, due to the increased availability of current data on states’ websites, we were able to collect data for 2007. Information was collected between February and August 2007 by reviewing state websites and regulations and calling key state contacts to verify information. Section 1 provides an overview of residential care and assisted living policy. Section 2 presents six tables, which compare states’ policy in selected areas. Section 3 provides summaries of each state’s regulations and policy for residential care settings, including assisted living facilities (ALFs).
The 2004 edition of the compendium differed from prior editions in that it used “residential care setting” or “residential care facility” (RCF) as the generic terms for all types of group residential care settings, rather than the term assisted living. The 2007 edition continues the use of these terms. Although many states use the term assisted living generically to cover virtually every type of group residential care on the continuum between home care and nursing homes, for many stakeholders the term assisted living still represents a unique model of residential care that differs significantly from traditional types of residential care such as board and care. When discussing state statutes and regulation, the compendium uses the terms that each state uses.
Adult foster care (AFC)/adult family care is a type of residential care. The most recent comprehensive study of AFC was conducted in 1995 so current information about these settings and their regulation is lacking.1 Although AFC has never been the focus of the compendium, some states now license adult foster/family care under their assisted living regulations. For example, North Carolina’s statute defines adult family homes (AFHs) as serving two to six residents and adult care homes serve seven or more residents, but licenses both settings as assisted living residences (ALRs).
Nine states -- Georgia, Louisiana, New Hampshire, New Mexico, Rhode Island, Oklahoma, North Carolina, South Carolina, and Vermont -- define at least one licensing category to include all residential care settings that serve two or more residents and eight states (Alaska, Arkansas, Colorado, Idaho, Illinois, Massachusetts, Missouri, and Vermont) have a threshold of three or more. A few states have different thresholds within a licensing category. (Information about regulatory thresholds is generally noted in the state summary definitions in Section 3 of this compendium.)
Consequently, in some states, the number of people served in a residential care setting is no longer a major factor distinguishing the licensing category of adult foster/family care from that of assisted living. This change raises questions about how regulations designed for larger facilities are applied to privately owned family homes compared to states that have separate licensing and regulatory standards for these models.
Each state summary provides information as to whether AFC is covered by assisted living/residential care regulations, or is licensed or certified under separate regulations. When available, the address for the website that hosts the regulations is listed.
Residential care is an important long-term care service option, particularly for individuals who cannot live alone but do not require the skilled level-of-care (LOC) that nursing homes provide. The purpose of this compendium is to inform residential care policy by providing detailed information about each state’s approach to regulating residential care, as well as its funding for services in these settings.
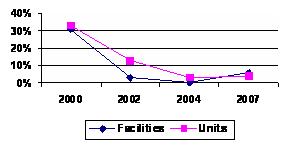
In 2007, states reported 38,373 licensed residential care facilities with 974,585 units/beds compared to 36,218 facilities with 935,364 units/beds in 2004; these numbers do not include facilities licensed separately as adult foster/family care or facilities licensed by Departments of Mental Retardation and Other Developmental Disabilities (MR/DD) or Mental Health.2 Compared to 2004, the supply of licensed facilities rose 6 percent and the number of units rose 4 percent. See Figure 1-1 for a comparison of growth rates since 2000.
| FIGURE 1-1. Supply Changes |
|
Changes in facility supply varied across states. About half reported an increase in the number of licensed facilities and half reported a decline. The supply of the number of licensed facilities rose over 10 percent since 2004 in 11 states (Alaska, 41 percent; Arizona, 29 percent; California, 14 percent; Georgia, 10 percent; Massachusetts, 11 percent; Minnesota, 33 percent; North Dakota, 26 percent; Wisconsin, 46 percent; and Wyoming, 33 percent). Supply declined more than 10 percent since 2004 in five states (Hawaii, 11 percent; Kansas, 12 percent; Nevada, 14 percent; New Mexico, 18 percent; and New York, 14 percent.) The decline in the number of licensed facilities did not always follow the direction in the supply in the number of units which suggests that smaller homes may have closed and a fewer number of larger homes were licensed leading to a decline in the number of facilities and a small increase in the number of units.
The 2007 review of state policy and activity found that regulation of residential care settings continues to evolve. Regulatory changes have tended to address the challenges posed by serving frailer and sicker residents as well as concerns among state licensing staff about inappropriate retention, adequacy of care, and the shortage of trained staff. States revised provisions in several areas, including staffing requirements; training requirements for direct care workers and administrators; criminal background checks; admission and retention criteria; disclosure requirements; and resident agreements.
Twenty-one states revised their regulations between 2004 and 2007, and 12 states reported current activity to revise regulations. Two states revised their residential care regulations to add a service philosophy, and Missouri and Pennsylvania adopted the term assisted living for residential care settings. Forty-three states and the District of Columbia now have a licensing category or statute that uses the term assisted living. Pennsylvania enacted a law creating a new licensing category for assisted living that requires units to have private bathroom, living and bedroom space and food preparation areas.
A few states reported changes in Medicaid coverage since 2004. Indiana and Ohio implemented Medicaid home and community-based services (HCBS) waiver to cover services in assisted living settings. While Alabama and the District of Columbia received approval to cover services in residential care settings under waiver programs, they have not yet implemented them due to lack of funding (Alabama) and promulgation of regulations (District of Columbia). California implemented a new 1915(c) waiver program that covers services in assisted living as a demonstration project. West Virginia withdrew an approved Medicaid HCBS waiver to establish a pilot assisted living program (ALP) in public housing sites in four counties.
The reported number of Medicaid beneficiaries served in residential care settings -- including assisted living but excluding adult foster/family care -- declined modestly from 121,000 in 2004 to about 115,000 in 2007.3 Most of the decline occurred in Medicaid state plan programs in Michigan and Florida.
In the past few years, the information available about assisted living and other residential care settings on websites hosted by state agencies has expanded considerably. A review of licensing agency websites identified a wide range of information useful to consumers and their families, as well as owners, operators, and developers (e.g., licensing regulations, survey guidelines, and incident reporting forms). See Table 1-1. Links to each website are included in the state summaries.4 States also post information to assist consumers and family members to determine whether residential care can meet their needs and to compare facilities (e.g., guides, disclosure forms, and survey findings).
All 50 states and the District of Columbia post links to their licensing regulations and statutes.
Thirty-nine states post additional information primarily for facility owners, administrators, and managers. For example, documents relating to the survey process, survey guidelines, training requirements, background check requirements, forms, and notices.
Forty-two states list all licensed facilities and some sites include their address and phone numbers, and the number of units.
Sixteen states post a consumer guide or a list of questions to help consumers and family members understand residential care options and to compare and select a facility.
Thirteen states include information from survey reports and complaint investigations. Survey reports are prepared by state monitoring staff following on-site visits to assess compliance with state licensing requirements.
| TABLE 1-1. Information Provided on States’ Websites | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| State | Rules | List
of Facilities |
Provider Tools |
Survey Findings |
Consumer Tools |
State | Rules | List
of Facilities |
Provider Tools |
Survey Findings |
Consumer Tools |
| AL | x | x | x | x | MT | x | x | x | x | ||
| AK | x | x | x | x | NE | x | x | x | |||
| AZ | x | x | x | x | x | NV | x | x | x | ||
| AR | x | x | NH | x | x | x | |||||
| CA | x | x | x | NJ | x | x | x | x | x | ||
| CO | x | x | x | x | NM | x | x | x | |||
| CT | x | NY | x | x | x | x | |||||
| DE | x | x | x | NC | x | x | x | x | |||
| DC | x | x | x | ND | x | x | x | ||||
| FL | x | x | x | OH | x | x | x | ||||
| GA | x | x | x | x | OK | x | x | x | |||
| HI | x | x | OR | x | x | x | |||||
| ID | x | x | PA | x | x | x | x | ||||
| IL | x | x | x | RI | x | x | |||||
| IN | x | x | x | SC | x | x | x | ||||
| IA | x | x | x | x | SD | x | x | ||||
| KS | x | x | x | TN | x | x | x | ||||
| KY | x | x | x | x | TX | x | x | x | x | ||
| LA | x | x | UT | x | x | x | |||||
| ME | x | x | VT | x | x | ||||||
| MD | x | x | x | x | VA | x | x | x | x | x | |
| MA | x | x | x | WA | x | x | x | x | |||
| MI | x | x | x | x | WV | x | x | ||||
| MN | x | x | x | x | WI | x | x | x | x | ||
| MS | x | WY | x | ||||||||
| MO | x | x | x | x | Total | 51 | 42 | 39 | 13 | 16 | |
| TABLE 1-2. Summary of Major Activities in Residential Care Policy Since 2004 | |
|---|---|
| State | Activities |
| Alabama | The state revised rules for ALFs and special care ALFs in 2005, 2006 and 2007. A system to profile facilities was implemented in 2004. A Medicaid waiver to serve persons with dementia in ALFs has been approved but not implemented due to budget constraints. |
| Alaska | Licensing for multiple entities was centralized in 2004. Safety and sanitation requirements were changed in 2006. A background check unit (BCU) was established in 2007 to centralize checks for direct care workers for programs administered by the Department of Health and Social Services (DHSS) that are subject to the licensing and certification authority of or are eligible to receive payments, in whole or in part, from the department. |
| Arizona | A general review of the regulations is underway. The governor issued an executive order in 2007 directing the state agency to develop a three year strategy to improve quality in nursing homes, assisted living and community care. |
| Arkansas | No new changes. |
| California | A law requiring additional training on assistance with self-administration of medications was enacted and will be effective in 2008. A Medicaid waiver pilot program covering assisted living was implemented. |
| Colorado | The state approved rules changing the licensing category for residential care facilities to assisted living and added intermediate sanctions for violations in March 2004. Further changes concerning donated medications were made in 2006 and provisions covering administrator qualifications, staffing and hospice services in licensed settings are being reviewed. |
| Connecticut | None. |
| Delaware | Changes in the definition of “incident” and “reportable” were approved in 2004. The state is phasing out the rest home licensing category. Those that meet the standard are converting to ALFs. Homes that do not meet the standards will continue to operate as rest homes. |
| District of Columbia | ALFs will be licensed in 2007. The new Medicaid waiver will be implemented once facilities are licensed. |
| Florida | The state modified training requirements in 2005 and “elopement” standards for persons with dementia were adopted in 2006. The Department of Elder Affairs transferred responsibility for training administrators and direct care workers to private organizations. |
| Georgia | The Office of Regulatory Services (ORS) has formed a workgroup to develop a method for rating facilities based on survey findings. The rating system is expected to be available on the ORS website in early 2008. |
| Hawaii | The licensing agency is planning to establish licensing fees that would be used for training and other licensing-related activities. The state is considering changes to the structural requirements for facilities, nutrition, staffing, and service plans. |
| Idaho | Significant revisions to the regulations became effective in October 2006. |
| Illinois | The number of licensed assisted living and shared housing facilities grew dramatically. Changes were made to the requirements for criminal background checks. Legislation passed in 2005 that expands shared housing establishments from 12 to 16 residents; allows licensed health professionals to administer sliding scale insulin, and requires that all applicants must complete their application within six months of the initial filing if portions of the application were incomplete. Supportive living facility (SLF) rules were amended in 2005 and 2006. |
| Indiana | The licensing regulations expired and were reissued in 2007. Medicaid Rates for assisted living providers were increased. |
| Iowa | Revised regulations became effective in May 2004. The state has transferred all rule making and oversight authority from the Department of Elder Affairs to the Department of Inspection and Appeals. |
| Kansas | Regulations are being reviewed in 2007, and minor changes are expected in 2008. |
| Kentucky | Changes to the certification requirements for assisted living communities will be finalized by the end of 2007. |
| Louisiana | No changes have been made to the regulations since 1999. |
| Maine | Minor changes to the regulations were made in 2006. |
| Maryland | Revisions to the regulations are expected to be final in 2007. Legislation passed in 2006 requires facilities to file a uniform assisted living disclosure statement with the licensing application. The disclosure form is posted on the licensing agency’s website. |
| Massachusetts | The regulations were revised in August 2006. Several changes were made, including the addition of special care facility training requirements and sanctions. |
| Michigan | Revisions to the Homes for the Aged regulations were promulgated. |
| Minnesota | Laws governing the licensing of home care agencies that provide services in housing with services establishment were changed in 2006. Coverage of assisted living services under the state-funded alternate care program was terminated. |
| Mississippi | The state revised rules in 2007. |
| Missouri | The Department of Health and Senior Services revised its regulations in 2007. Legislation addressing sprinkler system requirements was passed in 2007. A Medicaid HCBS waiver is being developed. |
| Montana | Regulations allowing the Board of Nursing to implement a medication aide program were issued in 2006. |
| Nebraska | Changes in 2007 added definitions, extended the occupancy certificate from 12 to 18 months, modified criminal background check requirements and raised licensing fees. Facilities may not call themselves assisted living unless they are licensed. |
| Nevada | The rules were revised in 2005 and 2006. Facilities that are marketed as providing assisted living services must have an endorsement on their license and provide potential residents with a disclosure statement that describes the personal care services that will be available. |
| New Hampshire | New rules for a new type of ALR called supported residential health care were effective in October 2006. Additional rules for a second model -- assisted living residence-residential care (ALR-RC) -- will be issued in 2007. |
| New Jersey | The regulations were revised in February 2007. The Medicaid payment methodology changed from a monthly to a daily amount. |
| New Mexico | Revised rules will be issued in late 2007 or early 2008. Additional funding was approved to hire more surveyors for adult residential care facilities. A new statute expanding criminal history background checks is being implemented. |
| New York | In 2004, the state enacted an assisted living reform law creating a new level of service for ALFs and rules implementing the changes will be final in 2007. Facilities may obtain a certificate allowing them to offer enhanced assisted living services to support aging-in-place. |
| North Carolina | Rules were amended in 2005 and further changes are expected in 2008 that will cover assessment and care planning, staff training, staffing, and special care units (SCUs). |
| North Dakota | None. |
| Ohio | RCF rules were revised in 2007. The changes affected special populations, admission/retention, staffing, training, dietary standards, and fire safety. Adult care facility rules were updated in 2006. A new Medicaid HCBS waiver to cover services in assisted living was implemented in 2006. |
| Oklahoma | In 2007, the Department of Health revised rules regarding medication administration, staffing in special care facilities, complaint procedures, incident reports, and other areas. |
| Oregon | A four-year review of the regulations was completed in 2007. Rules for assisted living and residential care facilities were consolidated. The state extended a moratorium on new ALFs until June 2009. |
| Pennsylvania | Regulations for personal care homes (PCHs) were revised in 2005. Legislation establishing an assisted living licensing category was signed by the governor in 2007. |
| Rhode Island | Legislation affecting administrator qualifications, inspections, and staff training passed in 2006. |
| South Carolina | None. |
| South Dakota | Changes to the regulations were adopted in 2006. The state is planning to amend its Medicaid waiver to broaden coverage of services available in assisted living centers. |
| Tennessee | Assisted care living facility (ACLF) rules were revised in 2007. Legislation passed in 2007 that allows facilities to serve Medicaid HCBS waiver participants. |
| Texas | The regulations were revised in 2007 and further changes may be made in 2008. |
| Utah | The state revised the regulations in 2005. The state plan managed care program that covers assisted living was converted to a 1915(c) HCBS waiver. |
| Vermont | None. |
| Virginia | Revisions were adopted in 2006. Legislation passed in 2007 that supports aging-in-place by allowing residents who do not meet the retention requirements to continue to live in the facility. |
| Washington | None. |
| West Virginia | Minor revisions to the regulations were effective in 2006. |
| Wisconsin | Revisions to the community-based residential facilities (CBRFs) rules are expected to be final in 2007. Information from inspection reports are now being posted on the licensing agency’s website. |
| Wyoming | Legislation establishing an adult family care home pilot and expanding funding for HCBS assisted living slots was approved in 2007. |
The widespread use of the term assisted living and the considerable state variability in its definition continues to fuel debate about what assisted living is and should be, how it should be regulated, particularly as the number of residents with higher levels of need increases, and whether facilities that do not support key assisted living principles should use the term.
States historically have licensed two general types of residential care: (1) AFC or family care, which typically serves five or fewer residents in a provider’s home although several states use a lower threshold; and (2) group residential care that typically serves six or more residents in a range of settings (from large residential homes to settings that look like commercial apartment buildings or nursing homes). States have used many names for these larger group residential care settings, including: board and care homes, rest homes, adult care homes, domiciliary care homes, PCHs, CBRFs, and assisted living. Until the mid-1990s, the most frequently used term was board and care. Today all types of group residential care are generally referred to as assisted living.
The physical character of a substantial portion of older group residential care facilities is quite institutional, with two to four persons sharing a bedroom, and as many as 8-10 residents sharing a bathroom. Concerned about the institutional character of these settings, policymakers in Oregon -- and gradually in other states -- developed a new licensing category called assisted living. What was new and desirable about assisted living was that it offered residents what traditional board and care facilities did not -- a philosophy of care that emphasized privacy and the ability to have greater control over daily activities such as sleeping, eating, and bathing.
Consumer preference for the new assisted living model of residential care led providers to market all types of residential care facilities as “assisted living” -- whether or not they provided private units or operated with a service philosophy that ensures resident autonomy. Forty-three states and the District of Columbia now use the term assisted living in their residential care regulations. In some states, assisted living is a specific model with a consumer-centered service philosophy, private apartments or units, and a broad array of services which support aging-in-place. In others states, residential care licensing categories have been consolidated under a new general set of “assisted living” rules that might cover the new model of assisted living, as well as board and care, multi-unit elderly housing, congregate housing and sometimes even adult family or foster care (e.g., Maine, Maryland, and North Carolina).
Many states view assisted living as a licensed setting in which services are delivered. Four states (Connecticut, Maine, Minnesota, and New Jersey) define assisted living as a service that may be provided in various settings, which do not have to be licensed. Connecticut and Minnesota license service providers, which may be different entities than the organization that owns or operates the building. Others states see assisted living as a licensed building in which supportive and health-related services are provided. The operator of the building is licensed, and services may be provided by the operator’s staff or contracted to an outside agency. See Box 1-1 for a more detailed description of states’ licensing and regulatory approaches.
| BOX 1-1. State Licensing and Regulatory Approaches |
|---|
| Institutional Model. This model has minimum building and unit requirements; typically, multiple occupancy bedrooms without attached baths, and shared toilets, lavatories, and tub/shower areas. Generally, states permit these facilities to serve people who need assistance with activities of daily living (ADLs). But they either do not allow nursing home eligible residents to be admitted or do not allow facilities to provide nursing services. Historically, this model did not allow residents who met the criteria for placement in a nursing home to be served. However, as residents have aged in place, some states have made their rules more flexible to allow a higher level of service. For example, some states allow skilled nursing services to be provided in residential care settings for limited periods by a certified home health agency. North Carolina is one of the states using this approach. |
| Housing and Services Model. This model licenses or certifies facilities to provide a broad range of long-term care services in apartment settings to persons with varying service needs, some of whom may be nursing home eligible. The state allows providers to offer relatively high levels of care, although licensed facilities may set their own admission/retention polices within state parameters and may choose to limit the acuity of its residents. Depending on the state, some or all of the needs met in a nursing home may also be met in residential care settings. By creating a separate licensing category for this model and retaining other categories, states distinguish these facilities from board and care facilities. Vermont is one of the states using this approach. |
| Service Model. This model licenses the service provider, whether it is the residence itself or an outside agency, and allows existing building codes and requirements -- rather than new licensing standards -- to address the housing structure. This model simplifies the regulatory environment by focusing on the services delivered rather than the physical structure. Approaches for regulating services may also specify the type of buildings, apartment or living space that can qualify as assisted living. Minnesota is one of the states using this approach. |
| Umbrella Model. This model uses one set of regulations to cover two or more types of housing and services arrangements: residential care facilities, congregate housing, multi-unit or conventional elderly housing, adult family care, and assisted living. Maine is one of the states using this approach. |
| Multiple Levels of Licensing for a Single Category. Some states set different licensing requirements for facilities in a single category, based on the extent of the assistance the facility provides or arranges and on the type of residents served. For example, Maryland licenses facilities based on the characteristics of residents they serve. The state categorizes low, moderate, and high-need residents based on criteria for health and wellness, functional status, medication and treatment, behavior, psychological health, and social/recreational needs. The state may grant a limited number of waivers to facilities allowing them to serve residents who develop needs that exceed the facility’s licensing level. |
| Several of these approaches are not mutually exclusive and may be combined. |
Generic use of the term assisted living obscures the differences between types of residential care settings, and makes it difficult for individuals to determine which setting will best meet their current and future needs. A 2004 study of six states’ use of Medicaid to fund services in residential care settings found that stakeholders in five of the states cited public confusion about residential care options as a major problem.5
At a hearing in 2000, the U.S. Senate Aging Committee challenged the assisted living industry to address concerns raised in a Government Accountability Office (GAO) report, one of which was the lack of a common definition of assisted living and resulting consumer confusion about this long-term care option. This and subsequent hearings led to the formation of the Assisted Living Workgroup (ALW) designed to bring together assisted living stakeholders to make recommendations to ensure high-quality care for all assisted living residents and to develop a common definition. The workgroup included over 50 organizations with a variety of interests including industry associations, professional organizations, consumer and advocacy groups, and regulators. See Box 1-2 for examples of various definitions of assisted living, including the one proposed by the ALW.
As states allow residential care settings to provide more health-related and nursing services, many observers believe that the key challenge in defining and regulating assisted living is to distinguish it from nursing homes while recognizing that both settings may provide some of the same services and serve some similar residents.
| BOX 1-2. Examples of Definitions of Assisted Living |
|---|
| Assisted Living Workgroupa |
Assisted
living is a state regulated and monitored residential long-term care option.
Assisted living provides or coordinates oversight and services to meet the
residents’ individualized scheduled needs, based on the residents’
assessments and service plans, and their unscheduled needs as they arise.
Services that are required by state law and regulation to be provided or
coordinated must include but are not limited to:
|
| Joint Commission on Accreditation of Healthcare Organizations (JCAHO) |
| An ALR is “a congregate residential setting that provides or coordinates personal services, 24-hour supervision and assistance (scheduled and unscheduled), activities, and health-related services. It is designed to minimize the need to move as needs increase; accommodate individual residents’ changing needs and preferences; maximize residents’ dignity, autonomy, privacy, independence, choice and safety; and encourage family and community involvement.”b |
| Oregon |
| Assisted living means a building, complex or distinct part thereof, consisting of fully self-contained individual living units where six or more senior and persons with disabilities may reside. The facility offers and coordinates a range of supportive personal services available on a 24-hour basis to meet the ADL, health services, and social needs of the residents described in these rules. A program approach is used to promote resident self-direction and participation in decisions that emphasize choice, dignity, privacy, individuality, independence and home-like surroundings. No facility in Oregon may use the term assisted living unless they are licensed. |
|
Federal law defines a nursing facility as an institution (or a distinct part of an institution) that is primarily engaged in providing skilled nursing care and related services for residents who require medical or nursing care, rehabilitation services for injured, disabled, or sick persons (a skilled LOC), or on a regular basis, health-related care and services to individuals who because of their mental or physical condition require care and services (above the level of room and board) which can be made available to them only through institutional facilities (the minimum LOC.)6
Many individuals who qualify for Medicaid coverage of nursing home care -- particularly those who do not require a skilled LOC -- receive care at home from family members, home health agencies and publicly funded programs such as the Medicaid HCBS waiver program. Because HCBS programs may only serve Medicaid beneficiaries who meet each state’s nursing home criteria, their emergence challenged the assumption that persons who needed the care provided in nursing homes could only be served in a nursing home. It is now recognized that many nursing home eligible persons can be appropriately served in multiple-settings, including residential care settings, particularly those who do not need skilled nursing services.
Because HCBS waiver programs serve some nursing home eligible persons in home and residential care settings, it is not really possible to develop mutually exclusive definitions for nursing homes and residential care, except for the provision of a skilled LOC. Doing so would severely limit states’ ability to offer these residential care settings as a service alternative for nursing home eligible persons. States want to be able to serve at least some nursing home eligible individuals in more home-like residential care settings without imposing the nursing homes’ regulatory structure.
Some observers believe there is perhaps too much emphasis on developing a common definition of assisted living given that all 50 states have the authority to define it how they want. Some believe that a better approach would describe assisted living in a way that recognizes the overlap of needs that can be met and the services that can be offered by both nursing homes and assisted living, yet highlights differences between them. One state regulator has suggested the following definition -- “Assisted living is a facility which provides housing, meals and long-term care services in a group residential setting that is not a nursing home” -- adding that specific requirements for different types of assisted living should then be spelled out in regulation. At the same time, providers need to understand what their liability is when serving medically fragile individuals as well as their requirements to meet these residents’ needs.7
To help prospective residents understand the differences between nursing homes and different types of residential care, some states require -- as Oregon, Washington and others do -- that facilities use standardized disclosure forms to describe their scope of service, rate structure, caregiver and nursing staff levels. Many believe that this approach will be much more helpful for consumers than a uniform definition of assisted living.
In short, individuals with health needs and impaired abilities can be served in a range of settings by a variety of service providers: home health agencies, home care agencies, adult day care (ADC), different types of residential care (AFC, board and care, assisted living), and nursing homes. Residential care is an important service option for people who cannot live alone and do not have informal care.
States have the responsibility for regulating residential care settings and their definitions and approaches reflect each state’s unique policy environment and preferences. Consequently, development of a standard definition of assisted living is unlikely. The approach to defining and categorizing residential care for research purposes depends on the research question. One national survey grouped facilities according to the level of services and the amount of privacy they offered (high and low).8 A study comparing resident outcomes in residential care and nursing homes would need to categorize facilities according to characteristics relevant to outcomes, such as staffing levels and the provision of nursing services and oversight.
| TABLE 1-3. States with Regulations that Include an Assisted Living Philosophy | |||
|---|---|---|---|
| Alaska Arizona Arkansas District of Columbia Florida Hawaii Idaho Illinois |
Iowa Kansas Louisiana Maine Maryland Massachusetts Montana Nebraska |
Nevada New Jersey New Mexico New York North Dakota Oklahoma Oregon Rhode Island |
South
Carolina Texas Vermont Washington Wisconsin Wyoming |
Twenty-nine states and the District of Columbia reported that they include provisions regarding assisted living concepts such as privacy, autonomy and decision making in their residential care regulations or Medicaid standards. (See Table 1-3.) Some states regulations are more detailed in these matters, others are less so. For example, regulations may state the importance of privacy, but only 11 states with a statement of the philosophy of assisted living require private apartment units;9 five states have mixed requirements, allowing bedrooms in some settings and individual apartments in new construction; and 14 states allow sharing (apartments or bedrooms) only by resident choice. (See section on Occupancy Requirements and Privacy for additional information.) Examples of state provisions that reference assisted living principles follow.
Florida’s statute describes the purpose of assisted living as “to promote availability of appropriate services for elderly and disabled persons in the least restrictive and most home-like environment, to encourage the development of facilities which promote the dignity, privacy and decision making ability” of residents. The Florida law also states that facilities should be operated and regulated as residential environments and not as medical or nursing facilities. Regulations require that facilities develop policies to maximize independence, dignity, choice, and decision making.
Illinois’ statute defines assisted living, in part, as a model that: (1) assumes that residents are able to direct their services and will designate a representative to direct them if they are unable to do so; and (2) supports the principle that there is an acceptable balance between consumer protection and resident willingness to accept risk and that most consumers are competent to make their own judgments about the services they are obtaining. The statute states that assisted living establishments and shared housing establishments “shall be operated in a manner that provides the least restrictive and most home-like environment and that promotes independence, autonomy, individuality, privacy, dignity, and the right to negotiated risk in residential surroundings.”
New Jersey requires facilities to coordinate services “in a manner which promotes and encourages assisted living values. These values are concerned with the organization, development, and implementation of services and other facility or program features so as to promote and encourage each resident’s choice, dignity, independence, individuality, and privacy in a home-like environment,” as well as “aging-in-place and shared responsibility.”
Texas’ authorizing statute specifies that rules must be developed to promote policies that maximize the dignity, autonomy, privacy, and independence of each resident; and that service delivery should be driven by a philosophy that emphasizes personal dignity, autonomy, independence, and privacy and should enhance a person’s ability to age in place.
Oregon, the first state to adopt a specific philosophy for assisted living, states that: “Assisted living … is a program that promotes resident self-direction and participation in decisions that emphasize choice, dignity, privacy, individuality, independence and home-like surroundings.”
Washington requires that the basic training curriculum for staff in residential care settings includes instruction on how to perform tasks while incorporating resident preferences; how to maintain residents’ privacy and dignity; and how to create opportunities that encourage resident independence.
Unless states operationalize assisted living concepts as specific regulatory requirements -- for example, assuring privacy by requiring private rooms or apartments -- the choices that facilities make in their physical and organizational structures and their service and training policies will generally determine whether the state’s intent is realized. In the absence of specific regulatory requirements, it may be difficult to determine whether a facility is carrying out the regulations’ philosophy.
Consumer advocates have questioned whether staff that inspect or survey nursing facilities should also inspect residential care facilities operating under an assisted living philosophy and related rules, without having specific training about this philosophy. Some states provide this training (e.g., Texas requires training for state inspectors on how assisted living differs from nursing homes). The National Academy of State Health Policy 2002 survey of state licensing agencies found that 24 states use different staff to survey residential care facilities than they use for nursing facilities; survey staff in the remaining states inspect both.
As illustrated in the examples above, ensuring resident autonomy is a central concept in the assisted living philosophy. Fifteen states and the District of Columbia have regulations referencing a process or approach for negotiating disagreements about residents’ autonomy and risk taking and providers’ concerns about risk (Alaska, Arkansas, Delaware, Florida, Hawaii, Illinois, Iowa, Kansas, New Jersey, Ohio, Oklahoma, Oregon, Vermont, Washington, and Wisconsin.) States use different terms to describe the process -- negotiated risk, managed risk, shared responsibility, compliance agreement, and negotiated plan of care.
Despite differences in the term, most of the regulations share common features, such as requiring that the agreement be written and signed by the resident and the appropriate facility administrator. State regulations typically require that the agreement describe the possible consequences of the resident’s actions, the specific concerns of the facility, and options that will both minimize the risk and respect the resident’s choices. They also generally require documentation of the negotiation process, and agreement or lack thereof, and the decision reached by the resident after consideration of the facility’s concerns. Several states allow surrogates or sponsors to negotiate risk agreements.
Examples of states’ specific provisions follow.
The District of Columbia defines a shared responsibility agreement as a “tool to recognize a resident’s right to autonomy by respecting his or her right to make individual decisions regarding lifestyle, personal behavior, safety and individual service plans.
New Jersey defines managed risk as the process of balancing residents’ choice and independence with the health and safety needs of the resident and other persons in the facility or program. If a resident’s preference or decision places the resident or others at risk or is likely to lead to adverse consequences, the facility may discuss such risks or consequences with the resident (and their representative if the resident wants). The facility can then negotiate with the resident a formal plan to avoid or reduce negative or adverse outcomes.
Oregon’s rules do not allow managed risk plans “with or on behalf of a resident who is unable to recognize the consequences of his/her behavior or choices.”
Vermont’s rules require that the facility notify the resident that the state Long-Term Care Ombudsman is available to assist in the negotiated risk process.
Wisconsin’s rules state that risk agreements do not mitigate or waive any tenant’s rights.
State licensing officials in states that allow negotiated risk agreements indicated that they are not widely used.
Historically, the physical character of a substantial portion of residential care was quite institutional -- as permitted by state regulation -- with 2-4 persons sharing a bedroom, and as many as 8-10 residents sharing toilet and bathing facilities. The new assisted living model of residential care became popular with older people in large part because it offers what traditional board and care facilities generally do not: privacy and the concomitant opportunity to have greater control over daily activities such as bathing, eating, and sleeping. Another reason for its popularity is that ALFs built in the 1990s have more attractive and comfortable physical environments than do board and care facilities, many of which were built in the 1960s and 1970s.
Consequently, single occupancy apartments or rooms dominate the assisted living private-pay market. A survey of non-profit facilities conducted in 1997 by the Association of Homes and Services for the Aging found that 76 percent of the units in free-standing facilities and 89 percent of units in multi-level facilities were private (studio, one, or two-bedroom units).10 A similar survey by the Assisted Living Federation of America found that 87.4 percent of units in its member facilities were studio, one, or two-bedroom units and only 12.6 percent were semi-private (shared by two unrelated persons).11 In a national survey of ALFs in the late 1990s, Hawes, et al. found that 73 percent of the units were private, 25 percent of the units were semi-private, and 2 percent were “ward-type” rooms that housed three or more unrelated persons.12
A 1998 survey of ALFs by the National Investment Conference (NIC) found that 17 percent of the residents shared a unit. Of these, 52 percent said that they shared their unit for economic reasons, 30.4 percent for companionship, and 14.9 percent because a private unit was not available. Just under 65 percent of those who shared a unit were satisfied with the arrangement and 35.7 percent preferred a single unit.13
Nationally, consumer demand, the availability of subsidized units, and the extent of competition are more likely than regulatory policy to determine whether studio or apartment-style living units are available for private-pay residents. However, for Medicaid eligible residents, state regulatory policy and Medicaid policy determine the types of units available. For example, Medicaid contracting requirements in Washington require participating facilities to provide private apartments shared only by choice.
Due to the popularity of assisted living, many providers of all types of residential care settings market themselves as assisted living, whether or not they give private rooms to all residents. Some board and care homes that want to be licensed as assisted living may have an interest in opposing rules requiring apartment-style units and single occupancy. On the other hand, advocates of assisted living as a unique model of care oppose the use of the term assisted living by facilities that do not offer private rooms or units to all residents. Consequently, occupancy requirements have become a contentious issue.
States have taken a number of approaches to setting occupancy requirements. Some states have simply amended their statutes to rename board and care homes as assisted living and continue to permit dual occupancy. Others have allowed dual occupancy standards in grandfathered buildings but require new buildings to offer single occupancy units. Some states maintain separate licensing categories, allowing dual occupancy in some settings and requiring single occupancy in others. Several states have multiple licensing categories and the two-person limit may apply to only one of the categories.
Thirty-five states have rules that allow two unrelated people to share a unit or bedroom. Ten states have licensing categories that allow four people to share a room; three states allow three people to share units. A few states to do not specify how many people may share a bedroom.
States that have developed a multiple-setting assisted living model vary the requirements by the setting. For example, New York allows sharing for board and care facilities participating in the Medicaid program but requires apartments in the “enriched housing category,” which includes purpose-built residences and subsidized housing. Additional examples of states’ requirements follow.
Florida licenses two types of assisted living, one which allows up to four people to share a bedroom, and extended congregate care (ECC), which requires private apartments or private rooms shared only by a resident’s choice.
New Mexico’s assisted living waiver provides services in two types of adult residential facilities offering “home-like” environments, which offer both units with 220 square feet of living and kitchen space (plus bathroom), and single or semi-private rooms in adult residential care facilities. Rooms and units may be shared only by choice.
Texas covers assisted living services through Medicaid to residents in three settings: assisted living apartments (single occupancy); residential care apartments (double occupancy allowed); and residential care non-apartments (double occupancy rooms).
Four people may share a room under what would have been described prior to the use of the term “assisted living” as board and care licensing rules in Delaware, Georgia, Indiana, Iowa, Michigan, Mississippi, Missouri, Nebraska, Pennsylvania, Rhode Island, South Carolina, and Virginia. Shared toilet facilities and bathing facilities are the rule among states with board and care regulations. State rules that allow bedrooms to be shared by 2-4 residents require bathrooms and lavatories for every 6-10 residents.
While a state’s policy sets the parameters for what may be offered and provided, the actual practice may be narrower. Shared units may be allowed, but the market may produce very few or no facilities that offer shared units. Further, facilities constructed prior to the development of the assisted living model may offer shared units while most, if not all, newly constructed buildings have predominantly or solely private units.
A GAO study of ALFs in four states concluded that while most facilities provide information about the services available, they do not routinely provide information about discharge criteria, staff training and qualifications, services not available from the facility, grievance procedures, and medication policies. The GAO report concluded that the provision of adequate information to prospective and current residents is a major issue that requires additional oversight.14
With few exceptions, states that license residential care require facilities to include specific information in residency agreements. Connecticut and Minnesota do not use residency agreements per se because they only license the service provider and the housing provider executes a lease agreement with tenants. Table 1-4 lists the type of information that states may provide in resident agreements and the number of states that require the provision of this information.
| TABLE 1-4. Residency Agreement Provisions | |||
|---|---|---|---|
| Topics Covered | States Requiring |
Topics Covered | States Requiring |
| Services included in basic rate | 49 | Grievance procedures | 21 |
| Cost of service package | 44 | Termination (admission/discharge) | 20 |
| Rate changes | 30 | Terms of occupancy | 13 |
| Refund policy | 30 | Advance payments | 13 |
| Cost of additional services | 28 | Temporary absences | 12 |
| Admission/discharge | 28 | Period covered | 11 |
| Service beyond basic rate | 27 | Accommodations | 10 |
| Payment/billing | 21 | Services not available | 7 |
| Residents rights | 21 | Other | 35 |
As can be seen, a majority of the states provide information about services, but only about half or less provide information about most of the other topics. Few states require information about medication policy and staffing.
Examples of “other” requirements follow:
Colorado requires facilities to disclose whether they have an automatic sprinkler system.
Kansas requires facilities to give prospective residents information on advance medical directives, resident rights, and the facility’s grievance procedure, before an agreement is signed.
Maine does not allow the resident agreement to contain any provision for discharge that is inconsistent with state rules or law or which implies a lesser standard of care than is required by rule or law. Agreements in Maine must also include information about grievance procedures, tenant obligations, resident rights, and the facility’s admissions policy.
Maryland requires disclosure in the agreement of the LOC that the facility is licensed to provide and the LOC needed by the resident at the time of admission. The state also requires facilities to disclose policies concerning shared occupancy and procedures that will be followed when a resident’s accommodations are changed due to relocation, change in roommate assignment, or an adjustment in the number of residents sharing a unit.
New Hampshire issued regulations in 2003 requiring disclosure of information to allow residents to compare ALRs, independent retirement communities, and elder housing, in order to make an informed choice about where to live. The state requires facilities to disclose whether they are licensed; the basic rate; the personal care and other services included in the rate; meals provided; transportation services; recreation and leisure activities; amenities in the living unit; policies regarding deposits/advance payment requirements and refundability; and services not included in the basic rate and their cost. Facilities must also provide information about their staffing, including whether staff are available 24-hours a day, and the availability of licensed nurses, personal care attendants, nursing assistants, and maintenance staff.
Wisconsin requires that the qualifications of staff who will provide services be included in the agreement as well as whether services are provided directly by the facility’s staff or under contract by an outside entity.
Some states require facilities to provide some of the information listed in Table 1-4 in a residents’ rights statement rather than a residency agreement, particularly information about grievance procedures.
The GAO study cited unmet consumer expectations for aging-in-place and forced moves as a major resident complaint. Twenty-eight states require agreements to include information about the facility’s criteria for admission, discharge, or transfer. Other states cover discharge criteria under provisions regarding termination.
Finally, several states have rules regarding the format of resident agreements. Kansas requires that agreements be written in clear and unambiguous language in 12-point type. Maryland requires agreements to use accurate, precise, easily understood, legible, readable, “plain” English. Wisconsin requires that agreement formats make it easy to readily identify the type, amount, frequency, and cost of services. Some states require information about provisions that allow staff to inspect living quarters, with the resident’s permission.
Most states do not have rules for revising or updating resident agreements. However, Alabama, Illinois, Mississippi, and Oregon require that agreements include the period covered by the agreement. Wisconsin requires that the agreement be reviewed and updated when there is a change in the resident’s condition or at the facility’s or resident’s request. Updates are otherwise made as mutually agreed to by the resident and the provider.
States regulations pertaining to admission and retention typically consider applicants’ or residents’ general condition, physical and cognitive function, behavioral problems, and health-related needs including the need for nursing care.
Only a few states (e.g., North Carolina and Illinois) do not allow individuals who meet the state’s minimum nursing home LOC criteria to be served in residential care settings. However, no states allow persons who need a skilled level of nursing home care to be served in residential care settings (e.g., individuals who require 24-hour-a-day skilled nursing oversight or daily skilled nursing services).
State approaches for setting admission and retention policies can be grouped into three categories:
These approaches are not mutually exclusive and states may use more than one approach. States may also grant facilities waivers that allow them to serve residents whose needs exceed the limits stated in statutes or regulations.
States using a full continuum approach have broad criteria that allow facilities to serve residents with a wide range of needs, in theory permitting residents to age in place. However, providers are not required to serve everyone who meet these criteria and can establish their own admission and discharge standards within state parameters. For example, Massachusetts allows providers to meet personal care needs and at a minimum must provide assistance with bathing, dressing, and ambulation. However, they are not required to offer assistance with other ADLs such as toileting and eating. Most other states allow, but do not require, residences to serve people with ADL needs. Facilities are often required to inform prospective residents about the type of conditions that would trigger discharge. Giving providers a great deal of discretion regarding discharge criteria can limit residents’ ability to age in place.
States using the full continuum approach include Hawaii, Kansas, Maine, Minnesota, Nebraska, New Jersey, and Oregon, and those with the most flexible rules include Arizona, Hawaii, Kansas, Maine, Maryland, Minnesota, New Jersey, Oklahoma, and Oregon. Examples of this approach follow.
Oregon generally does not limit whom facilities may serve. The rules contain “move out” criteria that allow residents to choose to remain in their living environment despite functional decline as long as the facility can meet the resident’s needs. However, facilities are not required to serve all residents whose needs increase. Providers may ask residents to move if: (1) their needs exceed the level of ADL services available; (2) the resident exhibits behaviors or actions that repeatedly interfere with the rights or well-being of others; (3) the resident, due to cognitive decline, is not able to respond to verbal instructions, recognize danger, make basic care decisions, express need, or summon assistance; (4) the resident has a complex, unstable, or unpredictable medical condition; or (5) the resident has failed to make payment for charges.
Hawaii’s rules do not specify who may be admitted and retained. Rather, each facility may use its professional judgment and the capacity and expertise of the staff to determine who it will serve. Facilities are required to develop their own admission and discharge policies and procedures. Discharge with 14 days notice is allowed based on behavior, needs that exceed the facility’s ability to meet them, or a resident’s established pattern of non-compliance.
Washington allows facilities to accept and retain residents if: (1) they can meet the individual’s needs, and provide required specialized training to resident care staff; (2) the individual’s health condition is stable and predictable, as determined jointly by the “boarding home” and the resident or the resident’s representative if appropriate; and (3) the individual is ambulatory, unless the boarding home is approved by the Washington State director of fire protection to care for semi-ambulatory or non-ambulatory residents. Individuals must also meet all of the boarding home’s established acceptance criteria.
Maine allows facilities to determine whom they will admit and the type of services they will provide. They may discharge residents who pose a direct threat to the health and safety of others, damage property, or whose continued occupancy would require modification of the essential nature of the program. Rules regarding the provision of nursing care vary by setting. Residential care facilities may provide nursing services with their own staff only to residents who do not meet the state’s nursing home LOC criteria. Residents who meet the LOC criteria can be served, but nursing services must be provided by a licensed home health agency. Congregate housing programs may receive a license to provide nursing and medication administration services by registered nurses (RNs) employed by the program.
New Jersey’s rules state that assisted living is not appropriate for people who are incapable of responding to their environment, expressing volition, interacting, or demonstrating independent activity. The rules allow facilities to provide a very high LOC, but they are not required to do so. The rules specifically state that facilities may choose to serve residents who:
Facilities may not serve residents who require a respirator or mechanical ventilator or people with severe behavior management problems, such as combative, aggressive, or disruptive behaviors.
States use discharge triggers to regulate the types of medical treatments that can and can not be provided by specific facilities and to determine when a resident can no longer reside in a facility. Most prohibited treatments require performance by skilled nursing personnel. States that use these triggers include: California, Delaware, Florida, Idaho, Illinois, Maryland, Mississippi, Nevada, New Mexico, South Carolina, Tennessee, Virginia, and West Virginia. State rules may overlap as Idaho, Maryland, and Mississippi also license by LOC, and New Jersey allows a full continuum of care. Examples of this approach follows.
Tennessee requires facilities to discharge individuals who require intravenous (IV) or daily intramuscular injections; gastronomy feedings; insertion, sterile irrigation, and replacement of catheters; sterile wound care; or treatment of extensive Stage III or IV decubitus ulcers or exfoliative dermatitis; or who require four or more skilled nursing visits per week for any other condition. Facilities may retain current residents who develop these needs for up to 21 days but may not admit individuals with these needs.
Virginia does not allow residential care facilities to serve people who are ventilator dependent; have Stage III or IV dermal ulcers (unless a Stage III ulcer is healing); need IV therapy or injections directly into the vein except for intermittent care under specified conditions; have an airborne infectious disease in a communicable state; need psychotropic medications but do not have an appropriate diagnosis and treatment plan; or have nasogastric tubes and gastric tubes (except when individuals are capable of independently feeding themselves and caring for the tube.)
Several states -- Arizona, Arkansas, Florida, Maine, Maryland, Mississippi, Missouri, Utah and Vermont -- have two or more levels of licensure based on the needs of residents or the services that may be provided. Idaho dropped licensing by levels of care in 2006. Examples of this approach follow.
Arizona licenses three levels of care: supervisory care, personal care, and directed care. Residential care facilities providing supervisory care may serve residents who need health or health-related services if these services are provided by a licensed home health or hospice agency. Those with a personal care service license may not accept or retain any resident who is unable to direct self-care; requires continuous nursing services unless the nursing services are provided by a licensed hospice agency or a private duty nurse; has a Stage III or IV pressure sore; or is bed bound due to a short illness unless the primary care physician approves, the resident signs a statement and the resident is under the care of a nurse, a licensed home health agency, or a licensed hospice agency. Facilities licensed to provide directed care may serve residents who are bed bound, need continuous nursing services, or have a Stage III or IV pressure sore.
Arkansas licenses two levels of facilities. Level I ALFs cannot serve nursing home eligible residents or residents who need 24-hour nursing services; are bedridden; have transfer assistance needs that the facility cannot meet; present a danger to self or others; or require medication administration performed by the facility.
Level II ALFs can serve nursing home eligible residents and participate in a Medicaid HCBS waiver, but cannot serve residents who need 24-hour nursing services; are bedridden; have a temporary (no more than 14 consecutive days) or terminal condition unless a physician or advance practice nurse certifies the resident’s needs may be safely met; have transfer assistance needs, including but not limited to assistance to evacuate the facility in case of emergency, that the facility cannot meet with current staffing; present a danger to self or others; or engage in criminal activities. Facilities may be licensed for both levels of care in distinct parts or separate wings.
Florida licenses four types of facilities: basic ALFs, limited nursing services (LNS), limited mental health services, and ECC which is the highest LOC. ECC facilities serve residents with higher needs and provide more services than the other levels including total help with bathing; nursing assessment more frequently than monthly; measurement and recording of basic vital functions; dietary management; supervision of residents with dementia; health education and counseling; assistance with self-administration and administration of medications; provide or arrange rehabilitative services; and escort services to health appointments.
Utah licenses two levels of facilities. Level I facilities serve residents who are ambulatory, have stable health conditions, require limited assistance with ADLs and need regular or intermittent care or treatment from facility staff. Level II facilities serve residents who need substantial assistance with ADLs, offer separate living units, and enable residents to age in place as much as possible. Level II residents may not need in-patient or 24-hour continual nursing care for more than 15 days, or a two-person assist to evacuate the building. Both types of facilities may assist with or administer medications under supervision of a licensed nurse.
States typically have two or more levels of nursing home care and not all persons served in nursing homes may be served in residential care. States distinguish among levels of care primarily for payment purposes. As noted in the discussion of admission and retention policies, above, states typically do not allow facilities to serve persons who require a skilled level of nursing care (as opposed to discrete skilled services, which many states allow in residential care on a limited basis).
Generally, individuals who meet a state’s minimum LOC criteria can be and are served in residential care settings. Only a few states do not allow residential care facilities to serve persons who meet the minimum or threshold nursing home LOC criteria (e.g., North Carolina). Because states’ minimum nursing home criteria vary markedly, individuals who meet the nursing home criteria in one state may not meet the criteria in another state. Thus, the statement that most states permit residential care settings to serve individuals who are “nursing home eligible” obscures sometimes significant differences in the type and LOC provided in these settings in different states.
States fall on a continuum from low to high thresholds for nursing home admission. Some states require a person to need assistance with only two ADLs, while others may require that a person be totally dependent in three or more ADLs. Some states require individuals to have a combination of medical conditions/needs and functional limitations; others require only certain medical needs. Of the 45 states whose criteria were reviewed for the 2004 Compendium, two used medical criteria only; 13 used medical and functional needs; eight used an assessment score based on a combination of medical and functional needs; and 22 used ADL thresholds. Section 3 provides information about each state’s nursing home LOC criteria.15 A few examples of states’ criteria follow.
Medical. Alabama requires an individual to need daily nursing or medical services that as a practical matter can only be provided in a nursing facility on an in-patient basis.
Medical and/or functional. Maine requires individuals to need skilled care on a daily basis (nursing or rehabilitation therapies); or extensive assistance with three of the following ADLs (bed mobility, transfer, locomotion, eating, and toileting); or one of several specifiedcombinations of nursing and functional needs.
ADL Threshold. New Hampshire requires individuals to either need assistance with two or more ADLs, or to need 24-hour care for at least one of the following: medical monitoring and nursing care; restorative nursing or rehabilitative care; or medication administration.
Combination of Factors. Illinois requires individuals to have a specific score on a standardized assessment. The score is derived from a score on the Mini-Mental State Examination (MMSE), and impairments in six ADLs and nine instrumental activities of daily living (IADLs) (including ability to perform routine health and special health tasks and ability to recognize and respond to danger when left alone).
Because Centers for Medicare and Medicaid Services (CMS) gives states considerable flexibility in setting minimum nursing home LOC criteria, states may choose to make the criteria more stringent in response to budget deficits. In states that cover Medicaid waiver services in residential care settings, if individuals become ineligible for nursing home care due to increases in the threshold LOC criteria -- for example, requiring three out of five ADL impairments rather than two out of five -- they will also be ineligible for waiver services in residential care settings.
If a state markedly increases the stringency of its minimum nursing home LOC criteria to control nursing home admissions, it would need to ensure that admission and retention criteria for residential care settings allow these settings to continue serving Medicaid waiver clients with the higher level of need required for Medicaid nursing home admission.
One of the attractive philosophical tenets of assisted living is that it allows aging-in-place -- meaning that as individuals age and become more disabled, additional services can be provided so that they will not have to move to another residential care setting or to a nursing home.
States seeking to facilitate aging-in-place and to offer consumers a full range of long-term care options allow more extensive services to be provided in residential care facilities, just as they can be provided in an individual’s home through home health agencies and in-home service programs.
However, facilities vary in the extent to which aging-in-place is possible, because states generally specify the range of allowable services and a minimum that must be provided, but do not require facilities to provide the full range of allowable services. Facilities are usually authorized to determine which services they will provide within state parameters. Facilities may offer very limited, moderate, or extensive services. Thus, both state regulations and facility policy govern the type, amount, frequency and duration of services provided, and, hence, the ability to age in place.
Thus, although state regulations frequently state their support for aging-in-place, they may also allow facilities to discharge individuals with higher levels of need. A key determinant of the ability to age in place is the extent to which states permit residential care facilities to address residents’ nursing and health-related needs.
Some experts contend that residential care settings cannot and should not be expected to meet the needs of persons with a high level of disability and/or medically complex conditions. Others agree, believing that residential care should be a social care model and that having nurses on staff is not only unnecessary but undesirable. However, other regulators, particularly in states that allow nurses to delegate specified nursing tasks, believe that residential care settings, like a person’s own home or apartment, are appropriate settings for people with severe disabilities and/or health needs. But some observers have expressed concern about direct care staff’s ability to recognize and address health problems in medically fragile residents when they are not trained nursing assistants. Many states do allow residential care facilities to provide skilled nursing care, as indicated in the following examples.
Illinois allows health services such as medication administration, dressing changes, catheter care, and therapies, if provided on an intermittent basis.
Florida allows the provision of nursing services under two types of licensure: LNS and ECC. A license for LNS allows facilities to provide nursing services including medication administration and supervision of self-administration, heat and ice cap application, passive range of motion exercises, urine tests, routine dressing changes that do not require packing or irrigation, and intermittent nursing services (e.g., change of colostomy bag and related care, catheter care, administration of oxygen, routine care of an amputation or fracture, prophylactic, and palliative skin care). A license for ECC permits a facility to provide nursing services in addition to those provided under the LNS license.
However, the state also specifies certain nursing services that may not be provided under either type of license, including oral or nasopharyngeal suctioning, assistance with tube feeding, monitoring of blood gasses, intensive rehabilitation services for a stroke or fracture or treatment of surgical incisions that are not clean and infection-free, and any treatment requiring 24-hour nursing supervision.
Washington’s regulations specify which skilled services may and may not be delivered by licensed nurses and unlicensed staff in residential care settings. RNs or licensed practical nurses (LPNs) may insert catheters, provide nursing assessments, and glucometer readings. Unlicensed staff under the supervision of a licensed nurse may provide Stage I skin care, routine ostomy care, enemas, catheter care, and wound care. Statutory changes in the Nurse Practice Act that would allow greater delegation are pending in the legislature.
New Jersey allows residential care facilities to provide skilled nursing procedures that are specifically barred in many states, for example, care of Stage III or IV pressure sores, ostomy care, and 24-hour nursing supervision.
Missouri allows residential care facilities to provide certain nursing procedures that they call “advanced personal care services.” They include catheter and ostomy care, bowel or bladder routines, range of motion exercises, assistance applying prescriptions or ointments and other tasks requiring a highly trained aide.
Maine allows residential care facilities and congregate housing programs to provide skilled nursing services.
Several states limit the provision of skilled nursing services in residential care settings by restricting their frequency and duration. Others prohibit facilities from providing these services directly, but allow them -- and/or residents -- to arrange for their provision through a home health agency. Some states use a combination of approaches, all of which are illustrated in the following examples.
Massachusetts -- like many states -- does not allow residential care facilities to serve residents who need nursing services available 24-hours-a-day. Skilled services may only be provided by a certified home health agency on a part-time or intermittent basis to persons whose medical conditions require services periodically on a scheduled basis.
In addition, the state allows residents to “engage or contract with any licensed health care professional and providers to obtain necessary health care services...to the same extent available to persons residing in private homes.” Because the Massachusetts statute allows skilled nursing services to be provided only by a certified home health agency, RNs hired by an ALF are not allowed to deliver skilled care. An initial draft of new state regulations did not allow the provision of skilled services for more than 90 days in a 1-year period. When the state attorney general’s office determined that such limits may conflict with fair housing rules, the state removed the 90-day limit.
Ohio limits the provision of skilled services in residential care facilities to 120 days in a 12-month period with exceptions for special diets, dressing changes, and medication administration.
Iowa allows facilities to provide health-related care (i.e., services provided by a RN, a LPN, or home care aide), and services provided by other licensed professionals as defined in regulations. Health-related and personal care services can be provided on an intermittent and part-time basis, which is defined as up to 35 hours a week on a less than daily basis, or up to eight hours provided seven days a week for temporary periods not exceeding 21 days.
Kentucky allows residents to arrange for additional services under direct contract or arrangement with an outside agent, professional, provider, or other individual designated by the client if permitted by facility policy.
In 2003 and 2004, hearings held by the U.S. Senate Special Committee on Aging, reports by GAO, and newspaper articles all raised concerns about the quality of care in residential care settings and the challenges providers and state oversight agencies face in assuring quality. In April 2004, the GAO issued a report on quality assurance initiatives in Florida, Georgia, Massachusetts, Texas, and Washington.16
The report stated that ALFs are more likely to meet and maintain licensing standards if they can obtain help in interpreting those standards and in determining what concrete changes they need to make to satisfy them. It described an initiative in Washington that established a staff of quality consultants to provide such training and advice to assisted living providers on a voluntary basis. Evaluations at six months and two years after implementation documented improvements in provider compliance as well as resident health and safety. However, a statewide budget crisis required the state to end funding for the program in order to maintain traditional licensing enforcement functions.
Wisconsin and Kansas have recently initiated activities to better ensure quality. The Wisconsin Bureau of Quality Assurance created an Assisted Living Forum for stakeholders to discuss current issues, interpretation of regulations, best practices, quality improvement (QI), staffing issues, national and state trends, and other public policy issues.
Wisconsin has also revised its survey process for residential care apartment complexes (RCACs), its apartment model of assisted living, which is not licensed but has to be either registered or certified to serve Medicaid clients. The new process includes a technical assistance component to interpret requirements; provide guidance to staff on consumer quality of life and care; review provider systems, processes and policies; and explain new or innovative programs. The revised survey strategy includes seven types of surveys: initial, standard, abbreviated, complaint, verification, monitoring, and self-report. The state determines which type of survey to conduct for each facility based on a range of factors, including its citation history. Abbreviated surveys are performed for facilities without any enforcement actions over the past three years and no substantial complaints or deficiency citations.
Kansas has adopted a collaborative oversight approach. Facility staff accompany the surveyor during the review. Observations are discussed during the process and, when necessary, problem areas are reviewed in the context of the regulatory requirements. Deficiency statements focus on consumer outcomes. The Director of licensing also conducts a full day training course several times a year on the role of licensed nursing in ALFs for nurses, operators and owners. The training covers use of the assessment, developing a service plan, managing medications and the Nurse Practice Act. The state believes that the combination of regular visits, consistent application of the regulations, and a more collaborative oversight process and training have resulted in better compliance with the regulations and fewer complaints.
Several states reported organizing periodic trainings for facility staff or including articles in a newsletter about specific problems that surveyors find are occurring in a number of facilities. One state indicated that facilities are responsible for resolving quality problems and the state provides consultants to assist them to do so. Other states clarify rules or statutes with facility staff during the survey or during exit interviews after the survey is completed. If the facility is able to correct the problem during the survey, no deficiency citation is issued. Utahallows new administrators to request assistance, and has procedures for the licensing agency to review survey forms with administrators, as well as previous reports and deficiencies. Pennsylvania provides guidance by disseminating information about best practices.
A few states indicated that they could not provide consultation and technical assistance due to staff shortages and the need to complete facility surveys.
States mentioned other quality assurance strategies including, providing technical assistance and follow-up; acting within ten days on complaints; having clear lines of communication and definition of duties for survey staff; developing clear enforcement procedures that are well understood by state staff meeting with providers to discuss issues; providing training; conducting follow-up visits; and maintaining a consumer perspective that focuses on improving care, not just punishing past failures. States described a number of quality initiatives underway including:
Other strategies focused on conducting regulatory reviews to bring provisions up to national standards and tightening standards for assessment, training, and LOC, including:
As facilities are allowed to serve residents with greater needs, regulators have cited medication administration and assistance with self-medication as a major concern. A study cited in a literature review on medication use in assisted living found that residents were prescribed an average of 4.6 medications per month; 37 percent took four to seven medications a month; and 11 percent took eight or more.17 Comparing prescriptions to the “Beers List,” the study found that 25 percent of the residents had inappropriate medication orders.18 Another study cited found that 11 percent of residents were taking two or more psychotropic medications and 70 percent were taking psychotropic agents without receiving mental health services. The literature review found that there was substantial use of medications considered inappropriate for use by elderly persons; widespread use of psychotropic medications; under-treatment of depression; and use of medications with undocumented diagnosis or reason for use.
Several states noted that its licensing agency is paying more attention to medication issues as the acuity level increases and more residents are taking increasing numbers of medications. States that did not previously track the prevalence of medication issues are now doing so.
Interviews with state contacts for the 2002 Compendium asked whether states allowed trained aides to administer medications or to assist with self-administration of medications. Of the responding states, 98 percent allow trained aides to assist with self-administration, and 63 percent allow aides who have completed and passed a training program to administer medications. Thirteen percent of responding states require facilities to have a consulting pharmacist. Several states require record reviews of medications by a RN.
States are addressing problems with medication administration by offering additional training, enacting changes to nurse delegation provisions, and tracking medication issues on survey reports. A few states indicated that problems with medication administration are consistently among the top eight or ten deficiencies and a few reported it was the most frequently cited deficiency. On the other hand, states reported that deficiencies and problems decreased after the licensing agency offered more training on medication administration to administrators, supervisory and direct care staff.
Staff training requirements are a key component of quality assurance. A national study found that the types of required staff training and orientation varied across facilities, but for the most part, relatively little training was required.19 Three-quarters of unlicensed personnel were required to attend some type of pre-service training or orientation, most commonly lasting between 1 and 16 hours. Only 11 percent of the staff who received required training completed it prior to the start of work; the remainder received on-the-job training or a combination of pre-service and on-the-job training. In contrast, nursing homes aides are required to have a minimum of 75 hours of training (ten days) and to pass an exam before they can work on a unit providing direct resident care.
Staff reported receiving training on -- or an orientation to -- the philosophy of assisted living and how that philosophy differs from traditional nursing home care and other residential care settings. However, the study found the staff were not well informed about normal aging and care for persons with dementia.
States’ regulations specify initial and on-going training requirements for staff and administrators but the level of specificity in the training requirements varies considerably. Some states specify only general requirements, while others specify topics to be covered, the number of training hours required, the completion of approved courses, or some combination thereof.
Forty-five states have specific regulatory provisions for facilities serving people with Alzheimer’s disease and other dementias an increase from 44 in 2004, 36 in 2002 and 28 in 2000. Examples of state regulations for facilities serving residents with dementia follow.
Rhode Island requires a license for dementia care when one or more residents’ dementia symptoms affect their ability to function as demonstrated by behaviors that adversely impact the rights of others; elopement; or an inability to self preserve. Facilities that advertise or represent special dementia services or that segregate residents with dementia also need a license for dementia care. In addition to basic license requirements, dementia care licenses require staff training specific to dementia care; a RN on staff and available for consultation at all times; and a secure environment appropriate for the resident population.
Pennsylvania’s rules contain provisions for securing units and providing adequate indoor and outdoor wandering space. They also specify competency-based training requirements for administrators and staff covering mandated topics such as the definition and diagnosis of dementia; differences between dementia, delirium, and depression; managing behavioral symptoms; and working with family members.
Montana has a licensure category for facilities that serve residents who are not capable of expressing their needs or making basic decisions. Requirements apply to staffing provisions; general staff education, training, and experience requirements; dementia specific annual continuing education requirement, including the teaching of skills necessary to care for, intervene and direct residents who are unable to perform ADLs; and techniques for minimizing challenging behavior. Other requirements apply to locked units or distinct parts of facilities.
Washington’s regulations require staff with experience and training in dementia care to coordinate outside services, offer monthly educational and family support meetings, and advocate for residents. Staff training requirements include a minimum of 30 hours on care for residents with dementia; the nature, stages, and treatment of the disease; therapeutic interventions; communication techniques; medication management; therapeutic environmental modifications; assessment and care planning; the role of family and their need for support; staff burn-out prevention; and abuse prevention. Eight hours of continuing training is required annually.
Staffing must be sufficient to provide 2.25 hours of direct care per resident per day. At least two staff must be present for units serving more than five residents. An RN must be available if residents require nursing procedures. The rules describe special requirements for the physical environment with security measures, including secured outdoor spaces.
Licensed facilities that do not market themselves as SCUs but serve residents with early symptoms of dementia must provide staff training on dementia care, including strategies to help residents manage their behaviors.
Twenty-eight states have disclosure requirements for facilities that advertise themselves as operating special care facilities or units or caring for people with Alzheimer’s disease or other dementias. These facilities are required to describe in writing how they are different from other facilities. The regulations may require a description of the philosophy of care, admission/discharge criteria, the process for arranging a discharge, services covered and the cost of care, special activities that are available, and specific features of the environment that address the needs of persons with dementia. See Table 1-5 for an overview of disclosure requirements. Specific examples of regulations regarding disclosure requirements follow.
Illinois’ standard Alzheimer’s Special Care disclosure form, which all providers must use, addresses the form of care or treatment; philosophy; admission and retention policies; assessment care planning and implementation guidelines; staffing ratios; physical environment; activities; family members’ roles, and the cost of care.
Minnesota requires facilities to provide information about the form of care or treatment; the treatment philosophy; unique features for screening, admission and discharge; assessment and care planning; staffing patterns; the physical environment; security features; type and frequency of activities; opportunities for family involvement; and the costs of care.
Texas requires a disclosure statement that describes the nature of the care or treatment provided; the pre-admission and admission processes; discharge and transfer policies; the planning and implementation of care; policies related to changes in residents’ condition; staff training on dementia care; the physical environment; and staffing.
Thirty-six states have requirements for dementia specific training and staffing for facilities serving people with Alzheimer’s disease and other dementias. Examples follow.
In Alabama, staff in specialty care facilities must complete a training program developed by the Department of Mental Health and Mental Retardation and receive six hours of on-going training a year on topics specified in the regulations.
Arizona requires staffing ratios of one staff per six residents during the morning and evening, and one per 12 residents at night.
Indiana requires six hours of training for direct service workers within six months of employment and three hours annually.
Rhode Island requires new direct service workers to receive at least 12 hours of orientation and training about dementia, communicating effectively with dementia residents, and managing problem behaviors. The state also requires that a RN be available to residents on site as needed, and available for consultation at all times.
| TABLE 1-5. Disclosure Requirements for Facilities Serving Residents with Dementia | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Topics Required | AR | CA | CO | DE | FL | GA | ID | IL | KY | MD | ME | MI | MN | MO |
| Philosophy | X | X | X | X | X | X | X | X | X | X | ||||
| Services | X | X | X | X | X | X | ||||||||
| Cost | X | X | X | X | X | |||||||||
| Population served | X | X | X | X | ||||||||||
| Admission and discharge process | X | X | X | X | X | X | X | X | X | X | ||||
| Assessment and care planning process | X | X | X | X | X | X | X | X | ||||||
| Staffing | X | X | X | X | X | X | X | X | X | X | X | |||
| Training | X | X | X | X | X | X | X | X | X | X | ||||
| Physical environment | X | X | X | X | X | X | X | X | X | |||||
| Resident activities | X | X | X | X | X | X | X | |||||||
| Family role | X | X | X | X | X | X | X | |||||||
| Psycho-social services | X | |||||||||||||
| Nutrition | X | |||||||||||||
| Form of care | X | X | ||||||||||||
| Security features | X | X | ||||||||||||
| Other | X | X | ||||||||||||
| Topics Required | MT | NE | NH | NC | OH | OK | OR | PA | RI | SC | TX | VT | WA | WV |
| Philosophy | X | X | X | X | X | X | X | X | X | |||||
| Services | X | X | X | X | ||||||||||
| Cost | X | X | X | X | X | X | X | X | X | X | ||||
| Population served | X | |||||||||||||
| Admission and discharge process | X | X | X | X | X | X | X | X | X | X | ||||
| Assessment and care planning process | X | X | X | X | X | X | X | X | X | X | X | |||
| Staffing | X | X | X | X | X | X | X | X | X | |||||
| Training | X | X | X | X | X | X | X | X | X | X | ||||
| Physical environment | X | X | X | X | X | X | X | X | X | |||||
| Resident activities | X | X | X | X | X | X | X | X | X | |||||
| Family role | X | X | X | X | X | X | X | X | ||||||
| Psycho-social services | X | |||||||||||||
| Nutrition | ||||||||||||||
| Form of care | X | X | X | X | X | |||||||||
| Security features | ||||||||||||||
| Other | X | X | X | X | X | |||||||||
Medicaid is a significant payer of long-term care services. Medicaid expenditures on long-term care comprise 33.2 percent of Medicaid spending (see Table 1-6). States are steadily shifting the balance of long-term care spending from institutional to home and community settings. Medicaid spending for institutional care in nursing homes and ICFs-MR rose from $41.5 billion in 1996 to $60.2 billion in 2006.20 During the same period, spending for home and community services (state plan personal care, home health, and HCBS waivers) grew from $11.2 billion to $38.5 billion.21 Consequently, Medicaid spending for institutional care dropped from 79 percent of all Medicaid long-term care spending in 1996 to 61 percent in 2006 for all populations. The percentage of Medicaid long-term care spending on home and community services was higher for individuals with development disabilities (60.7 percent) than for adults with physical disabilities and elders (28.6 percent.)
| TABLE 1-6. Medicaid Long-Term Care Spending (in billions) | ||||
|---|---|---|---|---|
| Service | 1996 | 2006 | ||
| Spending | Percent | Spending | Percent | |
| Home Health | $2.1 | 1.4% | $3.6 | 1.2% |
| Personal Care State Plan | $2.9 | 1.9% | $9.3 | 3.1% |
| HCBS Waiver | $6.2 | 4.0% | $25.6 | 8.6% |
| ICF-MR | $9.7 | 6.3% | $12.5 | 4.2% |
| Nursing Home | $31.8 | 20.6% | $47.7 | 16.0% |
| Total Long-Term Care | $51.8 | 33.6% | $99.3 | 33.2% |
| Total Medicaid | $154.2 | $298.7 | ||
Much of the growth in HCBS spending has been for services for persons with MR/DD, which account for 75 percent of all spending.
The expansion of home care programs, home health services, and residential care options has afforded persons with long-term care needs a number of alternatives to nursing homes. People with fewer ADL impairments are less likely to enter a nursing home.22 Thus, while the absolute number of nursing home beds increased from 1.8 million in 1985 to 1.9 million in 1999, the rate per thousand persons over age 75 declined from 141 beds to 117 beds, and nursing home occupancy rates dropped from 92.3 percent in 1987 to 87.0 percent in 1996,23 and further declined to 85.6 percent in December 2003.24 See Table 1-7 for occupancy rates in each state.
Declining nursing home occupancy rates create some concerns for states. First, as higher income individuals choose assisted living, the proportion of nursing home residents who are Medicaid beneficiaries increases. Increased reliance on Medicaid creates pressure to raise payment rates to replace revenue formerly received from private-pay residents. Second, excess capacity creates a greater likelihood that Medicaid nursing home expenditures will rise if Medicaid beneficiaries do not have access to sufficient home and community services and must rely on nursing homes at greater expense to the states.
State officials thus have an interest in ensuring that the supply of nursing facilities declines as the supply of home and community services expand. The 1999 U.S. Supreme Court Olmstead decision gives further impetus for shifting spending from institutions to home and community settings. That decision, and guidance to states from CMS, requires that states have plans for serving people with disabilities in the most integrated setting. Additionally, the ruling states that if states have a waiting list for services, the list must move at a “reasonable pace.”
| TABLE 1-7. Nursing Home Supply and Occupancy Rates and Residential Care Supply, 2003 | |||||||
|---|---|---|---|---|---|---|---|
| State | NF Supply/ 1000 65+ |
Occupancy Rate |
Residential Care Supply/ 1000 65+ |
State | NF Supply/ 1000 65+ |
Occupancy Rate |
Residential Care Supply/ 1000 65+ |
| US | 50.0 | 85.6 | US | 50.0 | 85.6 | ||
| AL | 44.8 | 90.0 | 16.8 | MT | 60.9 | 77.0 | 30.4 |
| AK | 20.6 | 83.9 | 12.3 | NE | 70.5 | 86.7 | 39.4 |
| AZ | 23.4 | 82.7 | 34.9 | NV | 21.6 | 83.6 | 16.7 |
| AR | 78.6 | 73.3 | 21.3 | NH | 51.0 | 92.4 | 26.3 |
| CA | 35.8 | 85.5 | 41.7 | NJ | 45.1 | 87.8 | 14.3 |
| CO | 46.3 | 81.9 | 31.7 | NM | 33.6 | 85.4 | n.a. |
| CT | 66.1 | 93.4 | 7.9 | NY | 49.6 | 92.7 | 17.6 |
| DC | 45.4 | 91.8 | 2.7 | NC | 43.1 | 89.0 | 17.6 |
| DE | 44.4 | 91.0 | 16.5 | ND | 69.4 | 93.5 | 30.3 |
| FL | 28.9 | 88.0 | 26.2 | OH | 79.3 | 86.0 | 27.7 |
| GA | 49.1 | 90.9 | 31.3 | OK | 71.1 | 67.3 | 21.0 |
| HI | 22.4 | 95.0 | 23.3 | OR | 28.8 | 67.8 | 47.5 |
| IA | 93.2 | 83.2 | 12.1 | PA | 47.6 | 89.9 | 40.0 |
| ID | 41.4 | 76.0 | 40.8 | TN | 52.8 | 92.0 | 19.3 |
| IL | 71.0 | 80.1 | 9.7 | SC | 36.4 | 91.8 | 33.1 |
| IN | 72.9 | 83.2 | 15.5 | SD | 68.0 | 92.4 | 31.0 |
| KS | 76.2 | 85.7 | 22.4 | TN | 52.8 | 89.3 | 19.3 |
| KY | 50.3 | 91.1 | 14.5 | TX | 56.4 | 77.5 | 19.6 |
| LA | 73.1 | 77.2 | 9.6 | UT | 37.4 | 72.7 | 22.5 |
| MA | 60.2 | 91.2 | 12.3 | VA | 38.5 | 89.9 | 42.3 |
| MD | 47.7 | 86.1 | 27.8 | VT | 44.5 | 92.4 | 30.4 |
| ME | 40.8 | 93.0 | 48.4 | WA | 35.0 | 85.7 | 36.2 |
| MI | 39.9 | 87.2 | 38.6 | WI | 60.2 | 86.6 | 38.9 |
| MN | 65.2 | 92.5 | n.a. | WV | 40.7 | 89.9 | 11.9 |
| MO | 71.9 | 75.7 | 28.8 | WY | 51.7 | 80.8 | 21.7 |
| MS | 52.4 | 88.6 | 14.2 | ||||
| SOURCES: Population Division, U.S. Census Bureau. Annual Estimates of the Resident Population by Selected Age Groups for the United States and States: July 1, 2003. American Health Care Association: December 2003. The supply of residential care settings was calculated by NASHP using Census data and data reported by state licensing agencies. (n.a. -- not available). | |||||||
While some areas of the country, particularly rural areas, have an inadequate supply of residential care facilities, in other areas, developers have over-built facilities. In over-built areas, nursing homes compete with ALFs for market share and residential care facilities compete among themselves for residents. Low occupancy rates in ALFs may lead to greater interest in serving Medicaid beneficiaries, thereby increasing the availability of this service option for low income individuals.
States have several options for using Medicaid to fund services in residential care settings (see Table 1-8): the Medicaid state plan, HCBS waivers (also called 1915(c) waivers), and Section 1115 demonstration programs. States most often use the HCBS waiver. See Table 1-9 for the sources of funding each state uses to pay for services in residential care settings. There has been no increase in the total number of states actually using Medicaid to cover service in residential care settings since 2004. States that did not implement approved waivers were dropped from Table 1-9.
| TABLE 1-8. States Using Medicaid to Cover Services in Residential Care Facilities | |||
|---|---|---|---|
| Waiver Only (29) | State Plan Only (7) | Waiver & State Plan (6) | |
| Alaska Arizona California Colorado Connecticut Delaware Georgia Hawaii Illinois Indiana Iowa Kansas Maryland Mississippi |
Montana Nebraska Nevada New Hampshire New Jersey New Mexico North Dakota Ohio Oregon Rhode Island South Dakota Texas Utah Washington Wyoming |
Maine Massachusetts Michigan Missouri New York North Carolina South Carolina |
Arkansas Florida Idaho Minnesota Vermont Wisconsin |
Congress authorized HCBS waivers in 1981 under Section 1915(c) of the Social Security Act. Under this provision, states may apply to HHS for a waiver of certain federal requirements to allow states to provide home and community services to individuals who would otherwise require services in an institution.
Under the HCBS waiver authority, states can provide services that are not covered by a state’s Medicaid program, such as personal care not covered by the state plan, home delivered meals, ADC, personal emergency response systems, respite care, environmental accessibility adaptations, and other services that are required to keep a person from being institutionalized. The waiver authority also allows states to provide waiver participants a greater amount, duration, and scope of services than are provided under the state plan.
Additionally, the waiver authority allows states to limit services to specific counties or regions of a state and to target services to certain groups -- strategies that are not normally allowed under Medicaid. State Medicaid agencies must ensure that waiver programs have provisions to ensure the health and welfare of participants. In addition, states must establish in advance how many people they will serve during the course of a year. Thus, in contrast to the regular Medicaid program, states may establish waiting lists for waiver programs.
| TABLE 1-9. Sources of Public Funding for Services in Residential Care Settings | |||||||
|---|---|---|---|---|---|---|---|
| State | Source of Funding | State | Source of Funding | ||||
| Medicaid Waiver |
Medicaid State Plan |
State Funds |
Medicaid Waiver |
Medicaid State Plan |
State Funds |
||
| Alabama | a | Missouri | Planned | X | |||
| Alaska | 1915 (c) | Montana | 1915 (c) | ||||
| Arizona | 1115 | Nebraska | 1915 (c) | ||||
| Arkansas | 1915 (c) | X | Nevada | 1915 (c) | |||
| California | 1915 (c)b | New Hampshire | 1915 (c) | ||||
| Colorado | 1915 (c) | X | New Jersey | 1915 (c) | |||
| Connecticut | 1915 (c) | X | New Mexico | 1915 (c) | |||
| Delaware | 1915 (c) | New York | X | ||||
| DC | d | North Carolina | X | ||||
| Florida | 1915 (c) | X | North Dakota | 1915 (c) | |||
| Georgia | 1915 (c) | Ohio | 1915 (c) | ||||
| Hawaii | 1915 (c) | Oregon | 1915 (c) | ||||
| Idaho | 1915 (c) | X | X | Pennsylvania | d | ||
| Illinois | 1915 (c) | Rhode Island | 1915 (c) | ||||
| Indiana | 1915 (c) | X | South Carolina | X | |||
| Iowa | 1915 (c) | South Dakota | 1915 (c) | X | |||
| Kansas | 1915 (c) | Texas | 1915 (c) | ||||
| Maine | X | Utah | 1915 (c) | ||||
| Maryland | 1915 (c) | X | Vermont | 1915 (c) | X | ||
| Massachusetts | X | Virginia | X | ||||
| Michigan | c | X | Washington | 1915 (c) | |||
| Minnesota | 1915 (c) | X | West Virginia | ||||
| Mississippi | 1915 (c) | Wisconsin | 1915 (c) | X | |||
| Wyoming | 1915 (c) | ||||||
| Total | 35 | 13 | 7 | ||||
|
|||||||
Finally, average expenditures for waiver beneficiaries must be the same or less than they would have been without the waiver (no more than average Medicaid nursing home costs).25 Importantly, while Medicaid may cover services in residential care facilities, it will not cover room and board. Medicaid can cover room and board only in institutions, such as nursing homes, ICFs-MR, and hospitals.
From the inception of the waiver program, states have used waivers to pay for services in residential care settings as an alternative to ICFs-MR. In 1981, Oregon became the first state to use the waiver program to fund services in residential care settings for elderly persons, but few states followed suit until the 1990s.
In the revised HCBS waiver application (version 3.4), assisted living is no longer listed as a separate service.States may list assisted living or services in assisted living and other residential settings under “other.” The guidelines CMS uses to review waiver applications ask the following questions about services in larger residential settings: “Is a home-like character maintained in larger settings (i.e., the facility is community-based) provides an environment that is like a home, provides full access to typical facilities in a home such as a kitchen with cooking facilities, small dining areas, provides for privacy and easy access to resources and activities in the community?” States may also choose to provide waiver services in congregate housing even if the waiver does not specifically cover a service category called “assisted living.”
Differences Between State Plan and Waiver Services
HCBS waivers and state plan services differ in several important ways. First, waiver services are available only to beneficiaries who meet the state’s nursing home LOC criteria; that is, they would be eligible for Medicaid payments in a nursing home if they applied. Nursing home eligibility is not required for beneficiaries using state plan services.
Second, states may set limits on the number of beneficiaries that can be served through waiver programs. The limits are defined as expenditure caps that are part of the cost neutrality formula required for CMS approval. Waivers are only approved if the state demonstrates that Medicaid long-term care expenditures under the waiver will not exceed expenditures that would have been made in the absence of the waiver. States do not receive federal reimbursements for any waiver expenditures that exceed the amount stated in the cost neutrality calculation. In contrast, state plan services are an entitlement, meaning that all beneficiaries who meet the eligibility criteria must be served. Federal funding matches state expenditures without any cap.
Perhaps the most significant difference between the two options is the ability under HCBS waivers to use more generous income-eligibility standards. To be eligible for personal care under the state plan, individuals must meet Medicaid’s community-based eligibility standards, which (depending on the state) are: (1) the Supplemental Security Income (SSI) level of income ($623 per month in 2007), (2) an amount above the SSI standard up to 100 percent of the federal poverty level, or (3) the state’s medically needy income standard.26
For nursing home and HCBS waiver applicants, states may use the special income standard (SIS), an optional eligibility category that allows individuals with income up to 300 percent of the federal SSI benefit ($1,869 in 2007) to be eligible. However, states can only offer this option in HCBS waivers if they offer it to nursing home applicants. Offering the higher income-eligibility standard in the waiver program “levels the playing field” between institutional and non-institutional services.
Table 1-10 summarizes the major differences between waiver services and state plan services.
Although the majority of states use Medicaid to cover services in residential care settings, the number of Medicaid beneficiaries who receive such services is considerably lower than might be expected because many states limit the number of people served under waivers. States using personal care under the state plan to cover services have higher participation rates than states using the waiver because state plan services cannot be capped.
| TABLE 1-10. Differences Between State Plan and Waiver Services | ||
|---|---|---|
| State Plan Service | 1915(c) Waiver Services | |
| Entitlement | States must provide services to all beneficiaries who qualify for Medicaid | States may limit the number of individuals served and restrict services to specific groups (e.g., age 65 or older, persons with MR/DD) |
| Scope | Must be available in the same amount, scope, and duration to all beneficiaries across the state | May limit amount, scope and duration to specific geographic areas or beneficiary groups |
| Duplication between HCBS and the State Plan | Services provided in accordance with state plan | May not duplicate services available in the state plan; may have different limits, definitions, or providers than state plan services |
| Service Criteria | Must meet state plan requirements for services | Must meet the state’s nursing home LOC criteria |
| Income | Must be SSI eligible or meet the state’s community-based income-eligibility standard | State may set eligibility up to 300 percent ($1,869) of the monthly federal SSI payment standard ($623) if also used for nursing home eligibility |
| Approval Period | Continuous unless amended by the appropriate state agency | Initial waivers approved for three years; renewals for five years |
For example, roughly 37,000 Medicaid beneficiaries living in residential settings are served under the state plan in North Carolina (20,442), Michigan (10,300), and Missouri (6,000). Waiver participation is highest in Wisconsin (8,542), Washington (6,193), Oregon (5,983), and Arizona (4,034). Florida serves 3,623 beneficiaries in its waiver program and 11,389 through the state plan.
States do not report the number of Medicaid beneficiaries in residential care settings by age or type of disability. The vast majority of the individuals served are age 65 and older but some may be under age 65. Some may have serious mental illness, acquired brain injuries, or MR/DD. Whatever their age or diagnosis, to be eligible for Medicaid coverage they must meet either the state’s nursing home LOC criteria for waiver services or the state’s service criteria for Medicaid state plan personal care services.
Participation figures are under-reported since a few states do not track and report the number of Medicaid beneficiaries by home or community settings. A few states reported the annual unduplicated number of Medicaid beneficiaries served in residential care settings, but most reported the number of people for a given month. Based on available data, participation is estimated to be just over 115,000 in 2007, down from 121,282 in 2004.
Limitations of Using Waiver Programs to Cover Services in Residential Care and How States Have Addressed Them
A major challenge facing policymakers who support a comprehensive range of home and community services is finding the resources to expand their availability. Waiver services are not an entitlement and most waiver programs operate with a specific appropriation based on a number of budgeted “slots.” Although states may cover services in residential care settings through a waiver program, limited slots may lead to a waiting list for services. On the other hand, nursing home care is an entitlement, and its budget is likely to rise each year through rate increases. In the event of a budget deficit, non-entitlement services are the most vulnerable to budget cuts. States are addressing this issue in several ways.
Colorado, Oregon, Vermont and Washington have shifted resources from institutions to home and community services by creating a single appropriation for long-term care services, sometimes called a global budget.
Arizona, Florida, Massachusetts, Minnesota, New York, Texas, Wisconsin and states with PACE programs have capitated funding for long-term care services, which gives contracting organizations the flexibility to approve the most appropriate service for beneficiaries.
Kansas, Maryland, Texas, and Wisconsin have implemented a Money Follows the Person (MFP) policy, which allows funding appropriated for nursing homes to be spent on home and community services for individuals who relocate from a nursing home.
Illinois uses funds from its nursing home appropriation in a waiver program that provides services for residents of SLFs. The program was built on the premise that about 10 percent of nursing home residents could be served in residential care settings with access to supportive services 24-hours-a-day. Because the program is funded from the nursing home budget rather than the waiver budget, the state is able to fund all approved SLF slots and there is no waiting list.
All of these financing strategies give states a mechanism to ensure that people who can be served in the community are not required to stay in nursing homes because of a waiting list for waiver services. To create incentives for states to support nursing home residents wanting to relocate to the community, the Deficit Reduction Act of 2005 authorized a MFP Demonstration. Thirty-one states received awards from CMS to carry out the demonstration. However, to be eligible for an enhanced federal match for HCBS, individuals can not relocate to a licensed residential setting that serves more than four individuals. This restriction may limit relocation for nursing home residents who cannot live alone and do not have family members to live with. For example, since Texas began its MFP policy in 2001, 25-30 percent of the individuals who relocated moved to a residential care setting.
Enabling Medicaid Beneficiaries to Pay for Room and Board
Medicaid beneficiaries with limited income may not be able to pay residential care facilities’ room and board rates. As noted earlier, Medicaid pays for room and board only in institutions, except in limited circumstances such as for the provision of respite care and for meals served as part of a day care program. For Medicaid purposes, room and board comprises real estate costs (debt service, maintenance, utilities, and taxes) and food.The costs of preparing, serving and cleaning up after meals can be covered as a waiver service.
Although Medicaid beneficiaries are responsible for room and board costs, states have a range of options to make them affordable.
Each of these options is discussed below.
Limiting the Amount Facilities Can Charge for Room and Board
States can limit the amount that can be charged for room and board by setting a combined “rate” for Medicaid beneficiaries that includes service costs and room and board costs, but the state only pays for services. This approach essentially caps the room and board rate that Medicaid beneficiaries pay. Other states simply limit by policy the amount that facilities can charge Medicaid beneficiaries for room and board. See Table 1-11 for a list of states that limit room and board charges. Medicaid programs that specify how much facilities may charge Medicaid beneficiaries for room and board usually limit the charges to the state’s SSI payment for a single elderly beneficiary living in the community, plus a state supplement, if any. This approach guarantees that Medicaid beneficiaries can afford room and board costs in facilities that accept Medicaid. If providers feel that the room and board rate is too low to cover costs, they may decide not to admit Medicaid beneficiaries. Only New Jersey has passed a law requiring that facilities licensed after September 2001 set aside 10 percent of their units to serve Medicaid residents within three years after licensing.
| TABLE 1-11. States That Limit Room and Board Charges | ||
|---|---|---|
| Arizona Colorado Delaware District of Columbia Georgia Hawaii Idaho* Illinois Indiana |
Maryland Minnesota Mississippi Montana Nebraska New Jersey New Mexico North Carolina North Dakota |
Ohio Oregon Pennsylvania South Carolina South Dakota Texas Vermont Washington Wisconsin |
| * The limit is “suggested.” | ||
Persons in residential care settings who qualify for SSI receive a basic federal SSI payment ($623 per month in 2007). In settings that do not have housing subsidies, they retain a PNA, typically $30 or higher as determined by the state, and the remaining income is paid to the facility for room and board. If the resident lives in a HUD 202 subsidized unit in which the tenant’s share of the costs for rent and utilities is limited to 30 percent of the resident’s income, the resident may have additional income that could be used to pay for services. If a person is SSI eligible and received $623 a month, they will pay 30 percent of this amount for rent ($186.90), and have $436.10 left over to pay for services or other costs depending on the state’s cost sharing provisions.
Impact in Subsidized Housing
HUD’s housing subsidy rules do not allow residential care settings to impose an additional charge for rent and utilities, but they can charge the resident for board (i.e., meal costs), or for services that are not covered by the Medicaid state plan or waiver program in a residential care setting. The amount of the permitted meal charge depends on the scope of the Medicaid service payment (i.e., whether it includes the cost of meal preparation). In all cases, Medicaid may not pay for food.27
Under HCBS waivers, the cost of preparing and serving food may be covered under the service payment. If preparing and serving meals is covered, the meal cost charged to tenants would be lower. If not, charges for a meal program would include the food, its preparation, serving, and cleaning up after meals. States covering personal care in residential care settings under the state plan may also allow payment for the preparation and serving of meals but not for the cost of food.
Medicaid beneficiaries with incomes over the SSI level must contribute income above the amount of room and board (minus a small PNA) to pay for services. Medicaid then pays the difference between the resident’s payment and the maximum service rate. Because beneficiaries in this category have more income than SSI beneficiaries, when they live in subsidized units, they will pay a higher rent, because the rent is calculated as a percentage of income. They also may have more income available to pay for services after the rental payment is made.
Providing State Supplements to the SSI Payment
To increase access for SSI beneficiaries in areas with high development costs, states can create a special SSI state supplement for persons in residential care facilities and limit what providers may charge to the amount of the federal payment plus the state supplement.28 Many states have such State Supplemental Payment (SSP) programs to supplement the federal SSI payment, which in 2007 is $623 a month; the payment is adjusted each January based on the cost of living. Individual states may use a specific term to refer to their supplement and some use the term SSI to refer to both the federal payment and any state supplement.
State supplements are totally state-determined and vary widely.29 States may pay different supplements based on a person’s living arrangement. A few states have developed a supplemental payment rate specifically for SSI recipients in residential care settings to provide them with sufficient income to pay for room and board.
Some policymakers might question the fiscal benefit of providing 100 percent state funding to enable residents to pay for room and board. However, it is important to consider the net state cost of services in a residential care setting compared to a nursing home. If the program diverts people from entering a nursing home or allows individuals to move from a nursing home to the community, states may fund a fairly substantial supplement to the federal SSI payment and still reduce their net cost. For example, the net cost for a state with an average nursing home payment of $3,000 a month and a 50 percent federal match is $1,500. A state could use a portion of the state match that would normally pay for nursing home care to raise the payment standard for residential care settings. Policymakers would have to determine how many people would be covered if the supplement were increased in order to calculate whether the change is “budget neutral” (or better) relative to the amount of the supplement.
Providing Housing Subsidies for Low Income Persons
Many states are exploring ways to combine Medicaid funding and subsidized housing to develop residential care options for low income persons. Housing subsidies can reduce housing costs for Medicaid beneficiaries and other low income persons, and are available through a number of programs:
Some federal housing programs either provide direct grants to public housing agencies and to developers or they reduce the debt incurred by the owner and, therefore, the revenue that needs to be raised through tenant rental fees. Others provide rental assistance directly to low income tenants who would otherwise be unable to afford even reduced rents.
The HUD Section 8 Housing Choice program contains some provisions that states can use to subsidize housing costs for waiver clients in residential care settings. Housing Choice offers two broad voucher programs: Fair Share and Special Purpose.
Fair share vouchers are allocated to serve people on waiting lists for Section 8 assistance. They are awarded through a competitive process and an additional 15 points are given to proposals that set aside 15 percent of the vouchers for people with disabilities. In addition, proposals qualify for five points if they demonstrate collaboration with Medicaid waiver programs and set aside 3 percent of the vouchers for waiver participants. Special purpose programs offer mainstream vouchers to help people with disabilities find affordable private housing, which can include residential care settings.
Typically, multiple public programs are needed to provide an adequate housing subsidy. For example, one affordable assisted living development in Vermont was financed by a combination of funds from HUD’s Section 202 Assisted Living Conversion Program, the Vermont Housing and Conservation Board, the Community Development Block Grant and City Trust, HUD Special Purpose Funding, and tax exempt bond financing through the Vermont Housing Agency. However, because housing subsidy programs and Medicaid operate under different requirements, including those related to eligibility, extensive planning and collaboration is needed to enable multiple programs to work together.
Using the 300 Percent of SSI Standard and Providing an Adequate Personal Maintenance Allowance
States have the option to use more liberal income-eligibility criteria for the waiver program -- up to 300 percent of the federal SSI payment -- ($1,869 per month in 2007). This option is attractive for waiver programs that cover services in residential care settings, because it expands the program to include beneficiaries who are better able to afford room and board costs. To make this option effective, however, states must allow eligible persons to retain enough of their income to cover “maintenance needs” including the room and board charges in residential care settings. Setting a higher maintenance allowance may allow more beneficiaries to be served in residential care settings; however, it will increase Medicaid’s service payment since it reduces the “excess income” that is applied to the cost of services.
Under Medicaid’s post-eligibility treatment of income rules for HCBS waivers, states are allowed to use “reasonable standards” to establish the maintenance allowance, and may vary the allowance based on the beneficiary’s circumstances. For example, states can permit Medicaid beneficiaries to keep sufficient income to pay for the needs of a dependent, health care costs not covered by Medicaid, and other necessary expenses.
Beneficiaries living in residential care settings may have different income needs depending on the type of facility: private market-rate facility or subsidized housing facility. The “rent” component of the monthly fee charged by facilities built with low income housing tax credits will be lower than the rent charged by privately financed facilities. Through tax credits, rents in assisted living can be reduced to around $400 a month. Setting the maintenance allowance based on the area’s average monthly charge for room and board may be overly generous when applied to residents in subsidized units. On the other hand, setting the maintenance allowance based on the amount paid by residents in subsidized units may be too low for private market facilities and create access barriers. If a state wants to improve access to both private and subsidized ALFs, it can set a separate maintenance allowance for each setting.
Interaction with housing subsidies. Under HCBS waivers using the 300 percent of SSI income-eligibility option, treatment of the additional income retained by residents because of rent subsidies depends upon the threshold set by the state for the maintenance allowance. If the state sets the maintenance allowance at the SSI level, all income above that amount is applied to the cost of Medicaid services. If the person has income between SSI and 300 percent of SSI ($1,869 in 2007), residents receiving housing subsidies may have additional income that is protected. For example, a person with $1,000 a month in social security and other income would have a maintenance allowance of $623 (the SSI monthly benefit in 2007) and apply the excess income ($377) to the cost of services. However, instead of paying $623 (less the PNA) for rent and utilities, if the resident is living in HUD Section 202 subsidized housing, the resident pays 30 percent of his or her income ($333.33) and keeps $103 for other expenses.
If the maintenance allowance is higher than $103, the resident can retain the higher amount and use it to pay for other expenses. For example, if the resident is allowed to keep the entire $1,000 a month, the resident’s portion of the rent and utility charge would be $333.33 a month and the resident keeps $667.67.
Separate maintenance allowance. States typically set a single maintenance allowance for all waiver participants. However, Medicaid rules allow states to set different maintenance allowances for each individual, or for groups of individuals, if they believe that different amounts are justified by the needs of the individuals or groups. For example, states can set a lower allowance for beneficiaries whose rent is subsidized. A lower maintenance amount for individuals with rent subsidies means more income is available to share the cost of services.
States face many challenges in their efforts to expand the supply of affordable assisted living by combining subsidized housing and Medicaid funding. Housing subsidies may not be available in a particular area or, as is often true with waiver services, waiting lists may exist for rent vouchers. To be effective, a rent subsidy voucher must be available when a waiver participant applies and at the same time that a facility is available that will accept the voucher as well as Medicaid payment. From application to implementation, close collaboration is needed between public housing agencies, waiver programs, and service providers. These challenges require knowledgeable housing operators and local housing authorities and state policymakers who are able to identify and address the barriers.
Family Supplementation
Family members may be able and willing to help with room and board costs when the beneficiary is unable to pay them. States set their own rules governing family supplementation.
As presented in Table 1-12, 25 states reported that they allow family supplementation, 12 states do not allow supplementation, and eight states have no policy. The remaining states either do not cover services in residential care settings or did not report whether they have a policy on supplementation.
Since Medicaid does not pay for room and board in residential care settings, rules regarding supplementation in nursing facilities do not apply (i.e., families of nursing home residents may not supplement Medicaid payments, which cover room and board and services). Several states indicated that they permit supplementation to enable beneficiaries to upgrade to a private unit.
In states that allow supplementation, family members need to understand that the amount of the supplement is considered in determining financial eligibility for SSI. Federal SSI regulations contain provisions for treating unearned income during the eligibility determination process. Because a family contribution paid directly to an SSI beneficiary is counted as unearned income, supplementation can lead to a reduction in the SSI payment or the loss of SSI altogether, and with it, potentially Medicaid as well.
| TABLE 1-12. Family Supplementation Policy | |||
|---|---|---|---|
| Allow Supplementation | No Policy | Prohibit Supplementation | |
| Arizona Colorado Connecticut Florida Georgia Kansas Idaho Illinois Iowa Maine Michigan Minnesota Missouri |
Montana Nevada New Hampshire New Jersey New Mexico New York North Carolina North Dakota Texas Utah Washington Wisconsin |
Alaska District of Columbia Hawaii Illinois Indiana Massachusetts Mississippi Wyoming |
Delaware Indiana Maryland Michigan Nebraska Ohio Oregon Pennsylvania Rhode Island South Carolina South Dakota Vermont |
If, however, the family contribution is paid directly to a RCF on the beneficiary’s behalf, it is treated differently, as an “in-kind” payment, and reduces the monthly SSI benefit by one-third or, if documented, by the actual amount of support provided if it is lower than one-third of the federal benefit. The maximum reduction is one-third even if the payment exceeds one-third of the SSI payment.
For example, a facility may have a room and board rate of $800, and because the SSI payment is not high enough to cover the charge, family members agree to help pay the cost. If the payment is made to the resident, it is considered unearned income and the federal SSI payment is reduced $1 for every $1 in unearned income, after a $20 per month exclusion. If the payment is made directly to the facility, the amount of the payment is considered “in-kind,” and the one-third reduction rule applies, that is, the federal benefit is reduced by one-third (or less if documented).
If the room and board rate is $800, the difference between that rate and the SSI benefit of $623 (in 2007) is $177. If the family pays $177 directly to the facility, then the individual’s SSI benefit is reduced by one-third of the SSI payment (i.e., $207). The family would then have to pay the facility an additional $207. The consequence of the reduction rule for in-kind payments, then, is that the family must increase its supplementation from $177 to $384.
Because the federal rule states that the SSI payment will be reduced by up to one-third, there is no limit on the amount of money that can be paid to a facility on behalf of an SSI beneficiary. If a family chooses, they could pay for room and board in a more expensive facility without jeopardizing an individual’s eligibility for SSI.
Family supplementation also has implications for Medicaid eligibility. Since Medicaid income and resource rules follow SSI rules, payment to a residential care setting would be considered in-kind income to the beneficiary. If the individual still receives SSI, and therefore remains a Medicaid beneficiary, there is no impact.31 Beneficiaries who are eligible through spend-down or the 300 percent of SSI special income level might be affected if the supplementation raises their income above the medically needy standard or 300 percent of SSI.
To prevent beneficiaries from losing Medicaid eligibility, states could amend their state plan, with approval from CMS, to exempt in-kind income that supports a person’s accommodations or services not covered by the Medicaid payment in residential care settings. Section 1902(r)(2) of the Social Security Act allows states to use less restrictive income and resource methodologies in determining eligibility for most Medicaid eligibility groups than are used by SSI. States can elect to disregard different kinds or greater amounts of income and/or resources than SSI, giving states more flexibility to design and operate their Medicaid programs.
Food Stamps
The use of food stamps to pay for meals subsidizes the board component of the room and board cost, making it more affordable for Medicaid beneficiaries and others with low incomes. USDA regulations allow meals provided in certain group living arrangements to elderly, blind, or disabled residents to be supported by food stamps (7 CFR §271.2). Group living arrangements are defined as a public or non-profit residential care setting that serves no more than 16 residents. Facilities that can participate as food stamp vendors receive stamps from beneficiaries, which are used as payment toward meal costs.
Wisconsin officials are working with USDA to allow RCACs to become approved food stamp vendors for eligible residents. SLFs in Illinois and Community-Based Residential Care Facilities in Wisconsin have been approved as food stamp vendors. Supportive Living Facilities in Illinois that participate in the program receive about $97 a month for eligible beneficiaries.
One final approach states can use to make room and board costs more affordable is to examine the facility’s monthly room and board charges to identify any coverable services -- such as laundry assistance, light housekeeping, or food preparation -- that Medicaid can reimburse for beneficiaries who require assistance with these IADLs. Including all coverable services in the state’s assisted living service payment reduces the beneficiary’s monthly payment solely to room and board and any other charges that Medicaid does not cover.
Effect of Medically Needy Rules on the Ability to Pay for Room and Board32
States have the option of covering medically needy beneficiaries under their Medicaid programs. The medically needy are persons who, except for income, would qualify in one of the other Medicaid eligibility categories (such as being over age 65 or meeting SSI disability criteria). Medicaid payments can begin for this group once they have “spent down” -- that is, incurred expenses for medical care in an amount at least equal to the amount by which their income exceeds the medically needy income level. Any family supplementation is considered part of the excess income that must be spent down.
The medically needy eligibility option can allow people who have income greater than 300 percent of SSI to become eligible for Medicaid services. But federal law imposes two significant constraints on the use of this option:
The state must cover medically needy children and pregnant women before it can elect to cover any other medically needy group. Additionally, the state may not place limits on who is eligible for Medicaid by using such characteristics as diagnosis or place of residence. Thus, it cannot use medically needy policies to extend Medicaid services only to HCBS waiver beneficiaries in residential care settings.
The maximum income-eligibility limit that a state medically needy program may use is based upon its welfare program for families -- levels that are typically lower than SSI. The income level must be the same for all medically needy groups in the state (i.e., states are not permitted to establish higher income-eligibility levels for selected subsets of the medically needy, such as beneficiaries in residential care settings).
These rules have several implications that states need to consider when trying to make the medically needy eligibility option work for higher income individuals in residential care settings. First, these individuals may find it more difficult to incur sufficient medical expenses to meet the spend-down requirements while living in the community than they would in a nursing home. The higher their “excess” income, the higher the amount of their spend-down -- which means only beneficiaries with extremely high medical expenses may qualify. Second, community providers are less willing to deliver services during the spend-down period, since payment cannot be guaranteed and collection may be difficult. Third, spend-down rules combined with low medically needy income-eligibility levels mean that individuals may not have enough total income to pay both the bills they incur under the spend-down provision and room and board.
In summary, room and board costs may present a barrier to residential care living for Medicaid beneficiaries unless states take specific steps to make them affordable. Several observers have suggested that the Medicaid program be allowed to pay for room and board in residential care settings as it does in nursing homes, which would require Congressional approval.
Reliability of Medicaid Funding Options
State plan services are an entitlement and all beneficiaries who meet the service requirements must be served. Personal care is the most common service covered in residential care settings under the state plan. States that do not already cover personal care through their state plan have been reluctant to add it because it is an entitlement and services must be provided statewide. However, CMS has allowed states to limit the provision of personal care provided under the state plan to specific providers, which may address state concerns about adding an open-ended entitlement to personal care under its state plan. South Carolina, for example, allows only licensed community residential care facilities (CRCFs) to provide personal care under the state plan.
On the other hand, services provided under Medicaid waivers are not entitlements and states may limit their provision to particular geographic areas, target groups, and care settings. Additionally, states may limit the number of waiver participants and further reduce this number during state budget cutbacks. States can also use solely state-funded long-term care programs to pay for services in assisted living. However, because they also are not entitlements, these programs are also vulnerable during state budget cutbacks.
Types of Waivers
As discussed earlier, states can cover services in residential care settings through a waiver program that provides services in the full range of home and community settings, or through a waiver that covers services only in residential care settings. The type of waiver can affect the pattern of referrals. States that include assisted living as one of a menu of home and community services must always offer beneficiaries a choice of services and cannot guarantee that applicants will choose assisted living. Single service waivers are better able to assure referrals as long as the number of providers contracting with Medicaid does not exceed the capacity of the waiver.
Waiting Lists
Some states have long waiting lists for waiver services, which can present a significant obstacle to serving Medicaid beneficiaries in assisted living. If waiver slots are not available, Medicaid eligible persons who cannot be served at home will need to enter a nursing home (if they meet the state’s nursing home LOC criteria) and the ALF will have to look elsewhere for new residents. Recognizing this as a potential problem, lenders may require that facilities establish a reserve to cover low occupancy in the event that Medicaid funds are not as available as projected.
States that fund waiver services and nursing homes from a global budget (Oregon and Washington) or who allow funding to “follow the person” who transfers from a nursing home to community settings (Indiana, Maryland, Texas, and Vermont) have more flexibility.33 States with MFP policies allow persons transitioning from nursing homes to bypass the waiting list. States that have nursing home transition programs help nursing home residents re-locate to community settings and have staff that will generate referrals to ALFs.
State Policy Regarding Room and Board Payments
About half of the states limit the amount that facilities can charge Medicaid beneficiaries for room and board -- usually to an amount equal to the federal SSI payment plus a state supplement (if offered). Others do not restrict the amount that can be charged, but providers need to understand their states’ income-eligibility rules and cost sharing requirements to determine how much Medicaid beneficiaries can afford. Persons eligible for Medicaid because they are receiving SSI have no income other than the federal payment and a state supplement (if any). Forty-four states provide supplements, which vary considerably. However, most are less than $100 a month. Some states pay different supplements depending on living arrangement. Even in states that use the 300 percent of SSI income-eligibility standard for its HCBS waiver program ($1,869 a month in 2007), beneficiary cost sharing requirements can reduce the amount of income available to pay for room and board.
Time Frame for Determining Medicaid Eligibility
Some states may not determine eligibility for services until financial eligibility has been determined, a process that can take up to 45 days or longer if further documentation of income or assets is needed. An extended time frame for determining Medicaid eligibility can be a major deterrent to participation in the Medicaid program, because providers will generally not want to admit someone if they are unsure about payment. If Medicaid eligibility cannot be determined quickly, beneficiaries in the midst of a transition, such as discharge from a hospital, may be more likely to enter a nursing home.
Some states expedite the determination of Medicaid eligibility or allow case managers or eligibility workers to “presume eligibility” based on preliminary information. However, if the eligibility presumption is later found to be incorrect, states do not receive federal reimbursement for expenditures made while the determination was pending and must pay providers solely with state funds. Nebraska, Ohio, and Washington have provisions for allowing presumptive eligibility, and Michigan allows Area Agencies on Aging (AAAs), which administer HCBS programs, to make presumptive eligibility determinations as well. Georgia and Pennsylvania have developed initiatives to expedite the application process.
The extent to which low income older people have access to residential care settings as an alternative to nursing homes depends in large part on the extent to which states use Medicaid to cover services in these settings, and providers’ views on the adequacy of Medicaid’s service reimbursement rates. In addition to the amount of the payment, the reimbursement approach can also serve as an incentives or disincentives for providers.
Data from the 2004 report suggested that states increased their payments over the prior four years, although they are still quite low relative to private-pay rates, and may not fully cover services to meet residents’ needs. However, key informants suggested that providers’ willingness to accept Medicaid rates is increasingly driven by an over-supply of facilities and difficulty finding private-pay residents.
States face a number of major challenges in developing Medicaid payment methodologies for residential care services, including: (1) defining and distinguishing between types of services, (2) collecting data on which to base payments while avoiding complex and burdensome new data collection requirements, (3) developing rates that support quality care and aging-in-place, and (4) providing reimbursement that is sufficient to ensure provider participation within state budget constraints.
States use five primary approaches to set rates for Medicaid services provided in residential care settings:
Table 1-13 lists the states that use Medicaid to cover services in residential care settings according to their rate-setting approach. Descriptions of each state’s reimbursement approach and rates can be found in Section 3 under the heading public financing.
| TABLE 1-13. State Rate-Setting Approaches | ||||
|---|---|---|---|---|
| Flat Rates | Tiered Rates | Case-Mix | Modified Case-Mix | Cost-Based and Fee-for-Service |
| Colorado Florida Georgia Illinoisa Massachusetts Mississippi Nebraska New Hampshire New Jerseyb New Mexico Rhode Island South Dakota |
Alaska Arizona Arkansasf California Delaware Indiana Maryland Nevada Ohio Oregon Texasc Vermont |
Minnesotad New York |
Mainee North Carolinae Washington |
Arkansasf Idaho Iowa Kansas Mainee Michigan Missouri Montana North Dakota Wisconsin |
|
||||
Flat Rates
Under a flat rate system, providers receive the same monthly payment regardless of the amount of services and staff assistance a resident requires. As in the health care system, flat rates for residential care create incentives for facilities to admit residents with lighter care needs, rather than those with multiple impairments in ADLs, cognitive impairments, or health needs. Twelve states use flat rate reimbursements, examples of which are described below.
Florida pays facilities $32.20 a day for services provided through the waiver program and $9.28 a day for personal care services provided through the Medicaid state plan.
Massachusetts uses Group Adult Foster Care (GAFC) -- a Medicaid state plan service -- to cover services in residential care settings. Using the state plan to cover services allows Medicaid to serve people who are frail but are not eligible to enter a nursing home following a tightening of the LOC criteria. The state pays a flat daily service rate of $37.75 for Medicaid beneficiaries.
Colorado’s Medicaid monthly rate for services is $1474.98 a month ($47.58 a day). The rate covers oversight, personal care, homemaker, chore, and laundry services. The state limits room and board charges for Medicaid beneficiaries to $571 a month.
Georgia pays a flat rate of $35.04 a day for waiver services provided to residents of group homes serving 7-24 people. The state limits room and board charges for Medicaid beneficiaries to $528 for a combined monthly rate of $1,569.
Illinois has different daily service rates for each of its seven regions, ranging from $50.76 to $66.92.Rates are set at 60 percent of the weighted average nursing facility rate for the region and are adjusted annually to reflect changes in the rates paid to nursing homes.
Flat Rates that Vary by Setting
States may vary its flat rates for different types of residential care settings. Texas pays a higher rate for apartment and other private occupancy settings, reflecting the state’s preference for these settings. Varying rates by setting may reflect differences in the average level of resident service needs in each setting. For example, a state may reimburse for services in both traditional elderly housing buildings and purpose-built ALFs. Generally, tenants in elderly housing sites are less impaired than those in purpose-built ALFs. Unlike purpose-built ALFs, elderly housing sites typically do not have 24-hour staffing and the capacity to meet the unscheduled needs of tenants. Consequently, elderly housing facilities receive a lower rate than purpose-built ALFs with 24-hour staffing.
New Jersey licenses assisted living services, which are provided in a range of settings. The state developed rates for each of three settings regardless of the level of services needed (see Table 1-14). Newly constructed ALRs receive $70 a day to cover waiver services, and comprehensive personal care homes (CPCHs) receive $60 a day. ALPs (services provided in subsidized housing) receive $50 a day. The state limits room and board charges in both settings to $680.55. Residents in subsidized housing pay a percentage of their income for rent; the housing subsidy pays the difference between this amount and the actual rent.
| TABLE 1-14. New Jersey Rate Schedule | |||
|---|---|---|---|
| Assisted Living Residences | Personal Care Homes | Assisted Living Programs | |
| Room and Board | $680.55 | $680.55 | n.a. |
| Medicaid waiver services | $70 per
day $2,100 per month |
$60 per
day $1,800.00 per month |
$50 per
day $1,500.00 |
| Total | $2,780.55 per month | $2,480.55 | $1,500 |
Tiered Rates
Tiered rates have been developed to more accurately and fairly reimburse providers for services provided to frailer residents. Tiered systems usually include 3-5 tiers based on the type, number, and severity of ADL limitations and/or cognitive or behavioral impairments, and create incentives for providers to serve residents with higher service needs. Eight states use tiered rates, examples of which are described below.
Arizona’s Long-Term Care System has three rate levels based on resident needs. The rate levels vary by type of setting; assisted living homes that serve ten or fewer residents and assisted living centers that serve 11 or more residents. The service payments are negotiated and vary by program contractor (county). Daily rates for Level 1 range from $41.23 to $70.11; for Level 2 from $55.00 to $91.91; and for Level 3 from $51.00 to $143.75.
Delaware has three levels of waiver service monthly payments, which were developed based on an analysis of spending for HCBS waiver clients living in their own homes and in AFC. Level I is $1,034; Level II is $1,271; and Level III is $1,544. Facilities receive an additional ten percent for residents with cognitive impairments. The state limits the room and board payment for SSI beneficiaries to $598 in 2007. The maximum payments rates for each level range from $1,632 to $2,142.
Oregon has five payment levels based on the type and degree of residents’ impairments. ADLs assessed include eating/nutrition, dressing/grooming, bathing/personal hygiene, mobility, bowel and bladder control, and behavior. Table 1-15 lists the impairments needed for each level, and the payments per level. The state limits the room and board payment for Medicaid beneficiaries to $483.70, which is less than the full SSI payment because of the PNA retained by the beneficiary.
Texas uses a tiered payment system for HCBS waiver services derived from their nursing home case-mix system. Payments, which vary by level and by setting, are listed in Table 1-16. The state limits the room and board payment for Medicaid beneficiaries to $479 a month.
| TABLE 1-15. Oregon Service Priority Categories and Monthly Payment Rates: Assisted Living (January 1, 2007) | ||||
|---|---|---|---|---|
| Impairment Level |
Service Priority | Service | R&B | Total Rate |
| Level 5 | Dependent in 3-6 ADLs OR dependent in behavior and 1-2 other ADLs | $2,010 | $483.70* | $2,493.70 |
| Level 4 | Dependent in 1-2 ADLs OR assistance in 4-6 ADLs plus assistance in behavior | $1,628 | $483.70 | $2,111.70 |
| Level 3 | Assistance in 4-6 ADLs OR assistance in toileting, eating, and behavior | $1,245 | $483.70 | $1,728.70 |
| Level 2 | Assistance in toileting, eating and behavior or behavior AND eating or toileting | $942 | $483.70 | $1,425.70 |
| Level 1 | Assistance in 2 critical ADLs or assistance in any 3 ADLs or assistance in 1 critical ADL and 1 other ADL | $712 | $483.70 | $1,195.70 |
| * The room and board payment is less than the SSI payment to allow the beneficiary to retain a PNA. | ||||
| TABLE 1-16. Texas Daily Reimbursement Rates Effective September 1, 2007 | |||
|---|---|---|---|
| Assisted
Living Apartment |
Double
Occupancy Apartment |
Residential
Care Non-Apartment |
|
| AL 1 | $67.76 | $60.76 | $42.21 |
| AL 2 | $62.80 | $55.81 | $37.25 |
| AL 3 | $56.04 | $49.05 | $30.50 |
| AL 4 | $58.63 | $51.64 | $33.08 |
| AL 5 | $52.40 | $45.42 | $26.86 |
| AL 6 | $50.68 | $43.69 | $25.13 |
Rates Based on Case-Mix Systems
Several states have adopted payment systems based on their nursing home case-mix methodology. Like tiered rate approaches, the case-mix approach creates incentives to serve more impaired residents by linking reimbursement to the LOC needed. Case-mix approaches typically have more categories that tiered rates. The case-mix approach requires the collection of extensive functional and health data for residents.
Both tiered rates and case-mix rates are subject to “category creep” or “gaming,” a tendency for facilities to interpret assessment data to support payment of the next higher rate or to request an adjustment because the resident has become more impaired and requires more staff support than upon admission. To address “gaming,” states may use an assessment by an independent case management agency to determine the original payment level. Subsequent requests to adjust the payment level can be reviewed by either a case management agency or the state agency before being approved. Five states use case-mix rates, examples of which are described below.
Washington uses a 12-payment level rate structure for waiver services provided in homes and residential care settings. A case manager conducts a comprehensive assessment to measure level of need and the appropriate rate tier. Three sections of the assessment are used to set the payment level based on a combined score based on points for: health status, psychological/social/ cognitive status, and functional abilities and supports. Individuals must have substantial or total impairments in an ADL for it to receive points. Points are also assigned for impairments in speech, sight, and hearing, the number of medications, disorientation, memory impairment, impaired judgment, wandering, and disruptive behavior. The total score determines the payment level.
New York modeled its reimbursement rates on its case-mix system for paying nursing homes. The service reimbursement is set at 50 percent of the Resource Utilization Group (RUG) rate for nursing home residents. The state has created RUG rates for 16 geographic areas of the state. The reimbursement category is determined through a joint assessment by the ALP and the designated home health agency or long-term home health care program. The Department of Social Services’ district office reviews the assessment and the RUG category. In 2007, the combined SSI and state supplement payment was $1,264. Beneficiaries retain a PNA of $200 and the balance is paid to the facility for room and board.
North Carolina covers personal care in adult care homes as a Medicaid state plan service and uses a modified case-mix payment system. The payment includes a flat rate for basic personal care with add-ons for residents with specific ADL impairments. Residents with extensive or total impairments in eating, toileting, or both eating and toileting qualify for a higher rate. In 2007, the basic payment is $17.33 for facilities with 30 or fewer beds and $18.98 for facilities with more than 30 beds. The additional daily rate for residents with extensive or total impairments in eating is $10.69, toileting $3.82, and impairments in both eating and toileting are reimbursed at $14.51. An additional payment for residents needing assistance with ambulation/locomotion is $2.73 a day. These payment levels are in addition to the basic rate. Eligibility for the additional payment is based on an assessment by the adult care home, which is verified by a county case manager. The state SSI and state supplement payment combined is $1,148 for room and board. The resident keeps $65 a month for personal needs and pays the remaining $1,083 to the facilities for room and board.
Cost-based reimbursement pays the facility for aggregate costs incurred by Medicaid eligible residents for allowable services.
Fee-for-service rates are determined by the number of hours of service identified in a care plan or a point system based on an assessment. For example, Kansas treats ALFs as providers of home care services, and reimburses for the services delivered. This approach may be cumbersome for some facilities to implement because they are used to receiving a regular monthly payment and providing resident services as needed pursuant to a plan of care. If services are reimbursed on a fee-for-service basis, facilities must track service delivery and prepare and submit bills to the payment agency. Depending on the pricing structure, ALFs may not be set up to prepare and submit itemized bills for each increment of service delivered to each resident.
Service delivery in ALFs also differs significantly from in-home service programs. Participants in home care programs typically receive services in block authorizations (e.g., two hours of care, five days a week). Assisted living residents typically receive services in 15-minute increments at various times seven days a week including nights. Home care programs typically do not cover services at night, and, of course, cannot meet unscheduled needs.
Tracking, aggregating, and billing can become cumbersome and time consuming, especially for facilities used to charging a single all-inclusive service fee. However, the pricing structure of many facilities includes a basic package of services with additional charges based on the increments of service used by residents. Facilities with this policy for private-pay residents may be better able to participate in Medicaid programs that reimburse using a fee-for-service approach.
Eleven states use fee-for-service rates, examples of which are described below.
Arkansas allows personal care services to be provided through the state plan in a person’s home “or other setting” such as a RCF. RCFs can be reimbursed for up to 64 hours of personal care per month at a rate of $13.84 an hour.
In Missouri, personal care and advanced personal care services are reimbursed as a Medicaid state plan service in RCFs. Facilities receive a unit rate (15 minutes) for services that are authorized in the care plan. The unit rate is $4.02 for personal care aides (PCAs), $5.03 for advanced PCA services, and $39.97 for nursing visits. The maximum payment is $2,379 a month, which is equal to the state’s Medicaid cost for nursing home care. No more than one nursing visit a week can be authorized. Very few residents receive advanced personal care and nursing visits.
The state limits the room and board rate for Medicaid beneficiaries to the federal SSI payment plus the state supplement, also called a “cash grant,” which varies depending on the type of facility. Type I facilities provide room and board, supervision, and protective oversight and receive a monthly payment of $754, comprising the SSI payment and a state supplement. Type II facilities provide personal care, dietary supervision, and health care in addition to Type I services, and receive a combined monthly payment of $850 a month. Residents can retain $25 a month for their personal needs.
Montana uses a payment system that has elements of a tiered system but lacks the structure and limited number of payment levels of tiered approaches. The payment amount varies widely based on the number and type of impairments, a structure more like a fee-for-service reimbursement approach. Montana’s payment is based on a point system. Agency field staff determine the number of points based on an assessment of impairments, and the provider receives $33 a month per point.
Monthly waiver reimbursement rates for personal care facilities vary depending on the residents’ LOC needs. Additional payments are calculated based on ADL and other impairments. The points determine the actual payment within a range. The state limits monthly room and board payments for Medicaid beneficiaries to $495. The maximum monthly payment for services is $63.34 per day or $1,900.20 for a 30 day month.
Adequacy of Rates
At first glance, it appears that states are paying markedly different rates for services, suggesting that some states may not be paying rates that are adequate to meet residents’ service needs. However, it is not possible to compare service rates across states due to significant differences in their admission and retention criteria for residential care settings. Most notably, rates for providers who do not serve nursing home eligible residents are not comparable to rates for providers who do serve this population.
States have no models on which to build reimbursement methodologies for residential care settings. Nursing home payment methods include both room, board and service costs and must address the needs of higher acuity residents than are generally served in residential care settings, even those that serve individuals who meet a nursing home LOC. Historically, board and care homes have provided room, board and very limited services, and payment rates typically have been set at SSI plus state supplement levels. The trend is for residential care settings to provide a LOC somewhere between traditional board and care and nursing homes.
A potential source of comparable cost data for developing reimbursement rates is in-home services provided under HCBS waiver programs. However, significant differences exist between services provided in-home and in residential care settings. First, in-home service utilization may be constrained by the times during which it is available, state funding limits, or the lack of in-home workers. Second, in-home utilization may overstate the amount of services an individual needs because services are reimbursed in blocks of time such as two hour increments. In contrast, because residential care staff are on-site at all times, this setting is able to offer more intermittent services in smaller time increments. On the other hand, in-home utilization may understate services received because it does not include the sometimes considerable amount of unpaid care provided by family and friends, particularly during the evening, at night, and on weekends, when in-home services are generally not available.
These differences in utilization patterns may or may not offset one another in the aggregate. Consequently, states may need to collect data on service provision in residential care settings in order to develop adequate service rates. Washington and Maine have both conducted studies to determine the amount of time direct care staff spend with residents.
Both federal and state governments recognize that, in order to reduce costly institutionalization, a range of supportive housing and service options is needed. An increasing number of persons 65 and older who can no longer live independently view assisted living as a preferred alternative to nursing home care, or as a means to forestall admission to a nursing home. But market-rate assisted living that provides private rooms and a high level of services is generally far beyond the means of most low income elderly persons.
There are several sources of funding available to finance the development or renovation of housing to create affordable assisted living. The Federal Government’s main vehicle for creating affordable housing is the low income housing tax credit program. Other sources of funding are programs in the U.S. Department of Housing and Urban Development (HUD) and USDA, and state programs. These departments provide funds to both finance new housing units and provide rental assistance in existing housing. However, not all programs that create and/or support affordable housing can be used for affordable assisted living.
Developing affordable assisted living is a complex undertaking. Different statutory authorities and administrative structures, and a lack of communication among those who manage housing and service programs, present major difficulties. A major issue for some housing subsidy programs is that the lenders and investors they depend on require evidence of a stable revenue source over the life of their commitment to protect their investment -- typically 15-30 years. But state service programs may be unable to provide a stable revenue source because they are subject to annual appropriations that depend on the state’s budget.
Additionally, despite targeting the same or similar populations, housing and service programs have different and often conflicting income, age, and functional eligibility rules that make it difficult to create the supportive housing plus services arrangements that frail elderly persons need. Medicaid program requirements can also pose barriers to the receipt of services in residential care settings (e.g., Medicaid’s rules regarding financial eligibility and post-eligibility treatment of income may limit an individual’s ability to pay for room and board).
Housing programs also have conflicting requirements. Yet, successful projects often need to combine funding from multiple housing finance programs (e.g., low income housing tax credits, HUD’s HOME program, the Federal Home Loan Bank’s Affordable Housing Program, conventional debt, and Housing Choice Vouchers), with two or more service subsidy programs (e.g., Medicaid state plan or waiver programs, state supplements to the SSI program, state-funded service programs).34
At the state level, some agencies that manage Medicaid waiver programs have begun working with state and local housing agencies and non-profit housing organizations to explore ways to combine housing subsidies with Medicaid services. At the federal level, HUD and HHS are currently looking at ways in which the agencies can work together to expand housing and service choices for people with disabilities.
The growth of assisted living has sparked interest in developing or expanding assisted living for elderly persons with low incomes. However, facilities may be reluctant to participate in the Medicaid program if they are not sure that they will have a reliable source of potential residents and payments. Housing providers and lenders need to project revenues to determine the feasibility of each project. Public agencies that provide subsidies to developers to build affordable assisted living need assurances that there will be a stable source of funding for residents’ service needs. Consequently, in addition to being knowledgeable about the Medicaid program generally, assisted living investors, developers, owners, and operators need to be aware of several Medicaid policy and program issues.
Donna Folkemer, Allen Jensen, Linda Lipson, Molly Stauffer and Wendy Fox Grage. Adult Foster Care for the Elderly: A Review of State Regulatory and Funding Strategies. AARP. Washington, DC. March 1996.
The data were obtained from state agency websites, when available, or reported by state licensing agencies. Partial information was reported for some categories in Delaware, Kentucky, Minnesota, New Jersey, New York, New Mexico and West Virginia. (See Table 2-1 in Section 2 for each state’s information.) While these numbers do not include facilities licensed by state MR/DD agencies, some individuals with MR/DD may be living in facilities licensed as residential care/assisted living.
The number of residents receiving Medicaid in residential care settings is slightly underreported because it does not include data from Kansas. Kansas’ reporting system does not differentiate between waiver clients served in their own homes and those served in residential care settings.
Please note that websites change over time and the links listed may not be current when you try to access the site.
The six states were Florida, Minnesota, Oregon, North Carolina, Texas, and Wisconsin. Oregon is the only state of the six that requires assisted living providers to offer private apartments. (See Janet O’Keeffe, Christine O’Keeffe, and Shula Bernard. Using Medicaid to Cover Services for Elderly Persons in Residential Care Settings: State Policy Maker and Stakeholder Views in Six States. Report prepared for the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy.) Available at: http://aspe.hhs.gov/daltcp/reports/04alcom.htm.
42 U.S.C. 1396r.
Wendy Fearnside, Program and Planning Analyst, Bureau of Aging and Long-Term Care Resources, Wisconsin Department of Health and Family Services.
Catherine Hawes, Ph.D. and Charles D. Phillips, Ph.D., M.P.H. A National Study of Assisted Living for the Frail Elderly: Final Summary Report. Texas A&M University System Health Science Center. US DHHS, Assistant Secretary for Planning and Evaluation, contract number HHS-100-94-0024 and HHS-100-98-0013. November 2000. [http://aspe.hhs.gov/daltcp/reports/finales.htm]
Oregon defines a “unit” as an individual living space constructed as a completely private apartment, including living and sleeping space, kitchen area, bathroom and adequate storage areas.
Ruth Gulyas. The Not-for-Profit Assisted Living Industry: 1997 Profile. American Association of Homes and Services for the Aging. Washington, DC. 1997. Also, 2000 Overview of the Assisted Living Industry. The Assisted Living Federation of America and Coopers and Lybrand. Washington, DC. 2000.
Ronald K. Tinsely, Robert G. Kramer, et al. Overview of the Assisted Living Industry. Assisted Living Federation of America. Fairfax, VA. 2000.
Hawes et al., op. cit.
National Survey of Assisted Living Residents: Who Is The Customer? NIC and the Assisted Living Federation of America. Washington, DC. 1998.
Assisted Living: Quality of Care and Consumer Protection Issues. GAO. T-HEHS-99-111. April 26, 1999.
Some state summaries do not include this information because it was not readily available.
Assisted Living: Examples of State Efforts to Implement Consumer Protections. GAO. GAO-04-684. Washington, DC. April 2004.
Thomas Clark, Director of Professional Affairs for the American Society of Consulting Pharmacists Medication Use and Pharmacist Impact in Assisted Living Facilities, located at http://www.ascp.com/public/pr/assisted/2003/rximpact.pdf.
The Beer’s List identifies medications to avoid or use within specified dose and duration ranges for elderly persons, as well as medications to avoid in elderly persons with specific diseases.
Catherine Hawes, Ph.D., et al. op.cit.
Data provided by Brian Burwell, Steve Eiken, et. al. The MedStat Group. Memorandum, 2006.
Medicaid spending for services delivered in residential care settings is not reported separately.
Jones, A. “The National Nursing Home Survey: 1999.” National Center for Health Statistics. Vital Statistics 13(15) 2002.
Rhoades, Jeffrey A. and Krauss, Nancy A. Nursing Home Trends, 1987-1996. Rockville, MD: Agency for Health Care Policy and Research; 1999. MEPS Chartbook No. 3. AHCPR Pub. No. 99-0032.
American Health Care Association. Based on CMS-OSCAR form 671:F41-F43. 2003.
States can use either a fixed per capita amount for each beneficiary or they can average expenditures across waiver beneficiaries. The latter method provides more flexibility because it allows some beneficiaries to exceed the nursing facility cost as long as costs for others in the program are lower and the average waiver cost does not exceed the average nursing facility cost. States have the option of setting a cap on waiver services at a percentage of nursing home costs (e.g., 80 percent).
Except in 209(b) states which have a Medicaid income-eligibility threshold that is lower than the federal SSI payment.
Capitated programs have more flexibility to pay for room and board costs than is allowed under standard Medicaid rules).
Many states have a state supplement for residential care settings that may be too low to cover more intense services needs and higher capital costs in some residential care settings.
For further information, see: “A Technical Assistance Guide for Housing Resources and Strategies,” prepared by the Technical Assistance Collaborative Inc. for the Rutgers Center for State Health Policy Community Living Exchange Collaborative, funded by CMS to assist Real Choice Systems Change Grantees. http://www.nashp.org/Files/Final_Regional_Forum_guide.pdf. Also, Ruth A. Gulyas. How States Have Created Affordable Assisted Living: What Advocates and Policymakers Need to Know. AARP. Washington, DC.
Payments in 209(b) states might affect Medicaid eligibility since it is not linked to SSI eligibility.
Some of the information in this section is taken directly from Smith, O’Keeffe, et al., Understanding Medicaid Home and Community Based Services: A Primer. HHS, Office of Disability, Aging and Long-Term Care Policy. Washington, DC. October 2000. Available at: http://aspe.hhs.gov/daltcp/reports/primer.htm.
Wisconsin has a special waiver to assure community placement for individuals who want to transfer when their nursing home closes.
Robert Jenkens, Deputy Director, Coming Home Program, Vice President, NCB Development Corporation. Personal communication, June 2004.
| REPORT FILES AVAILABLE: |