
Studies Make Case for Finasteride to Prevent Prostate Cancer
The initial results from the largest completed prostate cancer prevention trial appear to have underestimated the benefits and overestimated the potential risks of finasteride, according to three new analyses of data from the trial. These results bolster the case for finasteride as a preventive agent against prostate cancer, say the studies' leaders.
Results from two of the analyses were presented on May 18 at the American Urology Association annual meeting in Orlando, FL, and all three appeared online May 18 in Cancer Prevention Research.
Initial results from that trial, the nearly 19,000-participant Prostate Cancer Prevention Trial (PCPT), were published in 2003 and showed that men who took 5 mg of finasteride daily for 7 years had a 25 percent reduced risk of developing prostate cancer compared with men taking a placebo.
However, finasteride treatment was also associated with a small but statistically significant increased risk for developing high-grade prostate cancers, those with Gleason scores of 7 to 10. And because the preventive benefit was the result of a reduction of non-high grade cancers, those with a Gleason score of 6 or less, some prostate cancer researchers argued that finasteride only prevents indolent cancers that would never require treatment, explains Dr. Ian Thompson, chair of the Department of Urology at the University of Texas Health Science Center at San Antonio and a senior author on two of the new analyses.
Neither conclusion, he says, now appears to be accurate.
"We've now shown that the cancers prevented by finasteride are often clinically significant, the same kind of cancers that lead to surgery," Dr. Thompson says. "In addition, we showed a 28 percent reduction of high-grade cancer with finasteride."
In a related editorial in Cancer Prevention Research, Drs. Christopher Logothetis and Paul Schellhammer, from University of Texas M.D. Anderson Cancer Center and Eastern Virginia Medical School, respectively, lauded the analyses, arguing that the results demonstrate that "the promise of prostate cancer prevention is a reality."
Two of the analyses were conducted independently, using 500 prostatectomy samples from the more than 2,000 patients diagnosed with cancer in the PCPT, to estimate the "true rate" of high-grade disease in the two study arms (finasteride and placebo). The analyses, one led by Dr. Mary Redman from Fred Hutchinson Cancer Research Center and the other by NCI's Dr. Paul Pinsky, used statistical modeling to extrapolate the Gleason scores at prostatectomy to the larger study population. Prostatectomy is the gold-standard for determining Gleason scores. Both analyses adjusted for the fact that, as recent studies have shown, finasteride increases the sensitivity of both prostate-specific antigen (PSA) testing and needle biopsy for detecting high-grade cancer.
No overall increase in high-grade disease associated with finasteride was found by either analysis, Dr. Thompson stresses. Instead, they found that finasteride had a modest protective effect, driven by the reduction in tumors scored as Gleason 7. Because of the limited number of cancers scored as Gleason 8 to 10, says Dr. Howard Parnes from NCI's Division of Cancer Prevention, it's not possible to draw firm conclusions about finasteride's affect on such tumors.
The third analysis, conducted by Dr. Scott Lucia from the University of Colorado Denver and colleagues, addressed whether finasteride prevents "clinically significant" prostate cancer by examining the extent of cancer present in the PCPT biopsy specimens of Gleason score 6 cancers - again, the cancers that finasteride was shown to inhibit in the PCPT. They assessed biopsy samples according to two different sets of criteria that can be used to guide treatment decisions. Sixty percent of tumors given a Gleason score of 6 or less were clinically significant by these criteria.
More than 90 percent of men whose prostate biopsies have Gleason scores of 6 opt to receive immediate treatment, explains Dr. Parnes, a co-author on two of the analyses. So, regardless of whether they would be considered clinically significant by these biopsy criteria, he says, "We shouldn't overlook the importance of preventing the so-called 'clinically insignificant' tumors."
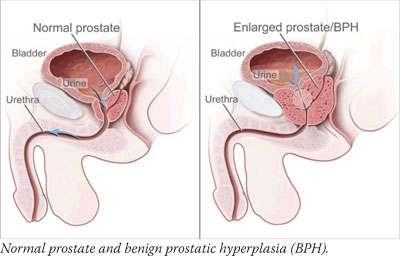
Finasteride is not yet approved by the Food and Drug Administration (FDA) for prostate cancer prevention, Dr. Parnes cautions. "However, men committed to regular screening and those with benign prostatic hyperplasia (BPH) may want to discuss this option with their physicians," he adds. Finasteride is FDA-approved for treating BPH symptoms and, at a lower dose, for reducing hair loss.
FDA approval aside, there are other factors holding finasteride back, says Dr. Brantley Thrasher, chair of Urology at the University of Kansas Medical Center.
Urologists have become "acclimated" to the idea that finasteride increases the risk of high-grade disease, he says. And it's more than that. "Nobody has worked out which patients we should be recommending finasteride to," Dr. Thrasher adds. "I think it will be an uphill battle to get wider adoption."
The AUA and American Society of Clinical Oncology are in the process of developing guidance on finasteride use for prostate cancer prevention, Dr. Parnes says.
—Carmen Phillips
|