|
|
|
FDA Home Page | Search
FDA Site | FDA A-Z Index | Contact
FDA
![]()
|
FDA Consumer
magazine |
This article originally appeared in the January-February 2003 FDA Consumer and contains revisions made in November 2003. |
|
Email
this Page To a Friend |
|
By Linda Bren
Her entire lifetime may span only a few weeks, but the female Culex pipiens mosquito makes the most of it. Feeding on the blood of humans and animals gives this common carrier of West Nile virus the protein she needs to produce several hundred eggs every few days--eggs that evolve into biting adult mosquitoes seeking blood meals of their own. And with each bite, an infected mosquito may transmit West Nile virus (WNV).
Most people who become infected with WNV have no symptoms, according to the Centers for Disease Control and Prevention (CDC). About 20 percent develop West Nile fever with its mild, flu-like symptoms: fever, headache, body aches, and sometimes a rash and swollen lymph glands. In a small number of people with symptoms--about 1 in 150--the virus causes life-threatening inflammation of the brain (encephalitis) or inflammation of the membrane surrounding the brain and spinal cord (meningitis).
There is no evidence to suggest that WNV can be spread through casual contact such as touching or kissing a person with the virus or by handling an animal with the virus, says the CDC. But public health officials are concerned that WNV may spread from person to person by other means.
"Based on investigations of cases previously reported, we believe that West Nile virus can be transmitted by both organ transplantation and blood transfusion," says Jesse Goodman, M.D., M.P.H., director of the Food and Drug Administration's Center for Biologics Evaluation and Research. It is not yet clear how commonly this occurs. In addition, there is limited evidence suggesting the virus may also be transmitted from mother to infant through breast milk.
No licensed tests exist yet for the large-scale screening of donor blood for WNV, nor are there any FDA-approved drugs to treat the virus or vaccines to prevent it. But the health and scientific communities, including federal agencies, public health departments, research facilities, and blood banks, are actively pursuing these medical advances.
|
|
WNV is one of a group of disease-causing viruses called flaviviruses, which are spread by insects, usually mosquitoes. Other flaviviruses include yellow fever, dengue, and St. Louis encephalitis viruses.
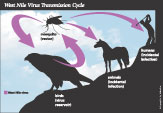
WNV primarily circulates between infected birds and mosquitoes that bite them. Only female mosquitoes bite and feed on blood; males feed on nectar. The infected mosquitoes can transmit the virus when they bite other animals or people. (See graphic at right.)
More than 130 species of birds have been reported to be infected with WNV, according to the CDC. The virus also can infect horses and some other animals. (See "Protecting Your Pet Against West Nile Virus.")
Even in areas where WNV is circulating, not all mosquitoes become infected with it, and human infection does not occur in all individuals exposed to mosquitoes. A study done in 1999 among residents at the height of WNV activity in New York City showed that only 2.6 percent had been infected, says the CDC. People who do get West Nile fever typically develop symptoms within three to 14 days after being bitten by an infected mosquito. Symptoms in people whose disease is limited to West Nile fever often go away without treatment in three to six days and do not seem to cause any long-term health effects.
The risk of getting the more severe West Nile encephalitis from an infected mosquito is higher for people 50 years of age and older. Many recent cases in transplant and transfusion recipients have been severe and, although unproven, it is likely that people with compromised immune systems are at increased risk for the more severe symptoms of WNV infection.
In 2002, the CDC, in collaboration with the FDA, state health departments, and blood organizations, concluded that 23 cases of WNV infection occurred from the transfusion of infected blood. In addition, WNV was identified in transplanted organs in at least four people who received organs from a single donor. That donor's blood was later confirmed to contain the virus at the time of organ transplantation.
The FDA and other organizations have taken precautions to reduce the risk of WNV transmission through blood transfusion and organ transplantation. One of these precautions has been to allow donor blood to be screened using rapidly developed experimental tests.
"This is a new challenge to blood safety," says Goodman. "There is a risk, and we have been taking it very seriously." The FDA has been working closely with diagnostics manufacturers, the blood industry and CDC to address the risk, says Goodman. "What is remarkable is that in only eight months since we recognized the new risk, tremendous progress has been made in protecting the blood supply from the threat of WNV, including the development and implementation of new screening tests to help keep blood safe."
In August 2002, the FDA alerted blood banks to be vigilant in excluding individuals from donating blood who may have early symptoms of WNV infection.
To further reduce the risk of transmitting WNV infection through transfusions, the FDA issued guidance to the blood industry in October 2002. The agency updated the guidance in May 2003 based on its experience with the 2002 outbreak. The guidance provides detailed information to help blood centers determine which potential donors should be excluded from giving blood, when to report donor illnesses that suggest WNV infection, and when to withdraw or quarantine blood products from these donors. Blood banks are not to take donations from people who have had a fever and headache in the week before they donate blood. In addition, donors are encouraged to report any illness suggestive of WNV infection that they contract within two weeks after donating blood.
The CDC has asked physicians to notify public health authorities of any patients who develop WNV infection within four weeks of receiving a blood transfusion or organ transplantation.
There is no risk that donors will acquire WNV by giving blood, and the FDA continues to encourage blood donations, as well as blood transfusions and organ transplants for those who need them.
Unlike other viruses, such as HIV and hepatitis B and C (which can be lifelong infections), WNV does not stay in the blood for a long period of time. "The available evidence supports the idea that most infected persons develop antibodies against the virus within one to two weeks," says Goodman. "These antibodies help clear the virus from the blood and likely protect the person against re-infection, but it's possible that immunity decreases in later years."
Although the virus disappears, the antibodies may remain in a person's blood for years, resulting in a positive blood antibody test. But there is no indication that such a person is chronically infected, says Goodman. "Current evidence supports the concept that such individuals who have recovered from West Nile virus can still be considered safe blood donors."
In July 2003, the FDA cleared the first commercially available test that will help physicians diagnose cases of potentially deadly WNV earlier than current methods allow. The test, called the IgM Capture ELISA, detects the levels in the blood of a particular type of antibody (IgM) to WNV. The test is for use in people who have symptoms of viral encephalitis or meningitis (headache, high fever, neck stiffness, stupor, disorientation, coma, tremors, convulsions, muscle weakness, and paralysis). Results from the IgM Capture ELISA must be confirmed with other lab tests as part of a complete evaluation. Diagnostic testing, based on CDC methods, is also available through state health departments.
Although such tests can detect antibodies to WNV in the blood, the IgM Capture ELISA is not adequate for screening donated blood to prevent the spread of WNV through transfusion. WNV is usually only present in the blood before symptoms and antibodies develop and can be detected, according to Goodman. Blood-screening tests are required to identify the virus itself, and the most sensitive methods work by detecting its genetic material.
The FDA has been working with the blood and medical diagnostics industry to speed development of sensitive blood-screening tests for WNV. Several screening tests have been developed that can detect very small amounts of genetic material. The FDA is evaluating the sensitivity and clinical use of these nucleic acid tests (NAT) and has encouraged blood banks to use them to help protect the safety of the blood supply. As a result, while the tests are being studied, the nation's blood supply is also currently being screened for WNV. Over 800 potentially infective WNV-positive units of blood have already been removed before they could be transfused, undoubtedly greatly reducing the risk of transmission of WNV by transfusion and protecting the safety of the blood supply.
Pathogen inactivation is another promising area of technology under development that is being explored to help make donated blood safe from WNV and other infectious agents. This type of technology uses chemical treatments, often combined with other methods such as ultraviolet energy, to kill the virus in the blood. The FDA is evaluating several inactivation methods for their effectiveness and safety, says Goodman, who stresses the importance of studying the effects of these treatments, both on possible infectious agents and on the quality and safety of the blood products themselves. "If one treats large numbers of units of blood to eliminate an infection from a rare unit, one has to be very sure that the effects of the treatment on those other units are not potentially harmful or don't potentially affect the quality of blood for the majority of patients who are receiving it."
Based on a case in Michigan in September 2002, it appears that WNV may be transmitted through breast milk. A new mother, unaware that she had been infected with the virus, possibly from a blood transfusion received shortly after giving birth, breast-fed her baby for 17 days. After the mother reported symptoms of nausea, malaise, and fever, she and her baby were tested for WNV. Laboratory tests confirmed that they both had WNV antibodies, indicating they both had been infected. The virus also appeared in the mother's breast milk.
Although the infant's exposure to the virus from a mosquito bite cannot be ruled out, it is unlikely, since the baby was outside only when transported from the hospital to the home, says Matthew Boulton, M.D., M.P.H., chief epidemiologist at Michigan's Department of Community Health. "We think the baby was exposed through the oral route from the breast milk," says Boulton, who adds that the infant showed no symptoms of illness from the virus and remains healthy.
These findings do not suggest a change in breast-feeding recommendations, according to the CDC. "The benefits of breast-feeding by far outweigh any potential risks of breast-feeding, including the risk of WNV transmission," says Lyle Petersen, M.D., deputy director of the CDC's Division of Vector-Borne Infectious Diseases. There is no evidence that WNV can be transmitted from mother to child during pregnancy or birth, he adds.
The only way to control the spread of WNV in people today is by controlling the mosquitoes that carry the virus and taking precautions to avoid getting bitten. (See "Protecting Yourself Against West Nile Virus.") But medical researchers are also working on drugs to treat WNV and a vaccine to prevent it.
More than 550 drugs have been screened to treat the disease, and about 3 percent have shown potential for additional testing in animals, according to the National Institute of Allergy and Infectious Diseases (NIAID).
NIAID is supporting the development of several vaccine approaches, including a live vaccine made by mixing WNV with the already existing yellow fever vaccine. Scientists are exploring additional approaches to developing effective WNV vaccines and the FDA is committed to helping to get these products developed and evaluated as quickly as possible.
Despite the risk of getting WNV through blood products, organs, and breast milk, these forms of transmission appear to be rare, according to the CDC. Bites from mosquitoes carrying WNV remain, by far, the most common means of transmission.
"While striving to keep blood as safe as possible, it is also important to keep a risk, even a poorly understood risk, in perspective," says Goodman, who emphasizes that only a few dozen cases of possible WNV transmission by blood transfusions are under investigation, out of the more than 4 million people who receive blood each year.
"Blood products and organ transplantation are often lifesaving, or life-enhancing," adds Goodman. "For people who need a transfusion or transplant, our current knowledge suggests that the potential benefits will outweigh the risks, including the risk of West Nile virus infection. The FDA, along with other components of the Department of Health and Human Services, will continue to do everything possible to determine the degree of this risk, and will find and take all available steps to reduce it."
The West Nile virus (WNV), first found in Africa in 1937, was identified in the Western Hemisphere for the first time in 1999 in the New York City area. Since then, it has spread quickly throughout most of the United States. From January 2003 to the end of October 2003, 44 states and the District of Columbia reported more than 7,700 human cases of WNV infection, resulting in 166 deaths.
There are about 200 different species of mosquitoes in the United States, and the WNV has been found in 36 of them, says Emi Saito, V.M.D., M.S.P.H., West Nile surveillance coordinator at the U.S. Geological Survey's National Wildlife Health Center. "No one really knows how it got into this country," says Saito. "It could have been brought in by a migrating bird, an imported bird, a mosquito hitching a ride on a plane or boat, or another host that we don't know about."
No matter what the route, scientists believe WNV is here to stay. The virus needs its natural host, the birds, to multiply, says Saito. "The only way to truly eliminate the virus in the U.S. is to kill every bird and every mosquito." Even if this approach were feasible, the virus could potentially re-enter the country by a migrating bird or by other means, adds Saito.
For people living in areas where West Nile virus is active, the Centers for Disease Control and Prevention recommends the following:
Humans aren't the only ones who can get West Nile virus (WNV). The virus is a threat to some animals, too, especially to wild birds and horses. About 40 percent of the horses that developed encephalitis (brain inflammation) from WNV died during the 1999 outbreak that originated in the New York City area. A USDA-licensed equine vaccine for WNV is now available through veterinarians.
WNV has been shown to infect dogs, cats, bats, chipmunks, skunks, squirrels, and domestic birds and rabbits. The virus has rarely caused illnesses in these animals.
Pet owners should not use human repellents that contain DEET on animals. Some animals are more sensitive than people to direct application of DEET products, making their use potentially harmful. Check with your veterinarian for the appropriate products to protect your pet. Also contact your veterinarian if your pet shows signs of WNV infection, such as fever, depression, lack of coordination, muscle weakness or spasms, or seizures or paralysis.
Adapted from the American Veterinary Medical Association and the ASPCA Animal Poison Control Center. For more detailed information, visit www.avma.org or www.apcc.aspca.org.
FDA Web site: www.fda.gov/oc/opacom/hottopics/westnile.html
CDC Web site: www.cdc.gov/ncidod/dvbid/westnile/
Or call the CDC hotline: 1-888-246-2675 Español: 1-888-246-2857 TTY: 1-866-874-2646
For information on West Nile virus in your local area, visit www.cdc.gov/ncidod/dvbid/westnile/city_states.htm
![]()