|
|
|
|
|
"Imported" Malaria in the United StatesRecent immigrants and refugees make up on average about 10% of the approximately 1,500 malaria cases brought into the United States each year. In addition to the threat the illness poses to the people themselves, imported cases make it possible for malaria to start circulating once again in the United States (malaria was eliminated by the early 1950s). Anopheline mosquitoes that are capable of transmitting malaria are found in the 48 contiguous states and US territories. 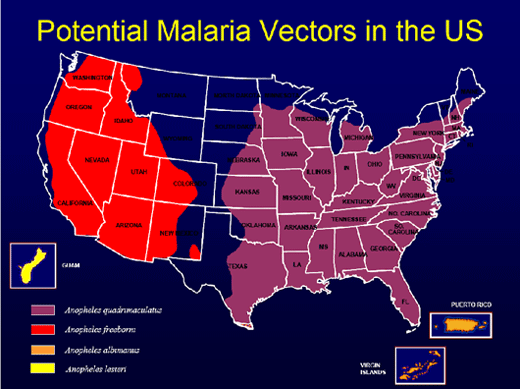 Malaria in Burundian RefugeesA recently released report in CDC’s August 15 MMWR describes three cases of Plasmodium falciparum malaria and two cases of Plasmodium ovale malaria during June 27, 2007–October 15, 2007 in King County, Washington, in Burundian refugees who recently arrived in the United States from two refugee camps in Tanzania, where they had been living after fleeing in 1972 from ethnic violence in their homeland. Some of the refugees had been displaced many times; most had always lived in exile. Among 1,805 Burundian refugees from Tanzania who resettled to 34 states from May 4 to July 7, 2007, 29 malaria cases were identified in 12 states, including Washington. Of the 29 persons with malaria, most (82%) were hospitalized; no one died. Up to 70,000 refugees are resettled to the United States annually, often from areas with endemic malaria. Refugees' Care Prior to Departure and Once in the United StatesCDC recommends that refugees from sub-Saharan Africa be given presumptive treatment for malaria (with an artemisinin-containing combination treatment), as well as other illnesses, before departure or during domestic refugee medical screening after arrival.1 Many U.S. health-care providers may not be familiar with recommended malaria treatment regimens. For example, one of the five patients described in the report did not receive adequate treatment for severe infection with P. falciparum. Instead, she received oral atovaquone-proguanil, which would have been appropriate for uncomplicated malaria. The recommended regimens for severe infection with P. falciparum include either intravenous quinidine or artesunate. Health-care providers in the United States caring for refugee populations resettling from malarial regions should remain aware of the possibility of malaria in these groups regardless of prior treatment. CDC Resources for Health-Care ProvidersFor health-care providers needing assistance with diagnosis or management of suspected cases of malaria,
Page last modified : August 15, 2008 Content source: Division of Parasitic Diseases National Center for Zoonotic, Vector-Borne, and Enteric Diseases (ZVED)
|
|
|||||||||||||||||||||||||||

| Home | Policies and Regulations | Disclaimer | e-Government | FOIA | Contact Us | ||||||
|