|
Adapted from the NCI Cancer Bulletin, vol. 5/no. 7, April 1, 2008 (see the current issue).
Unlike most cancers, colorectal cancer is considered preventable in many cases: prevailing opinion states that many malignancies found in the colon or rectum began years earlier as adenomas - noncancerous tumors that form in the linings, or mucosa, of these organs. Early detection and removal of these adenomas is the basis of screening for colorectal neoplasms.
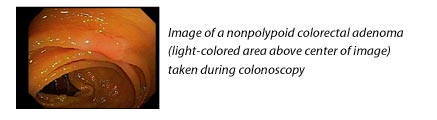
Traditionally, doctors have focused on finding and removing polypoid adenomas - growths that protrude from the mucosa - during screening colonoscopy. But newer evidence suggests that flat (having a height less than half of the diameter) or depressed adenomas may be even more likely to harbor precancer or cancer, and may be more common than previously realized.
In a recent study published in the Journal of the American Medical Association (JAMA), investigators examined 1,819 patients undergoing colonoscopy for screening, surveillance, or symptoms of colorectal neoplasms. Although just over 9 percent of adenomas found were flat or depressed (known as nonpolypoid), these growths accounted for about 15 percent of identified neoplasms and 54 percent of high-grade dysplasia and submucosal invasive carcinoma in this series of patients.
Advanced cancers that arise from nonpolypoid adenomas are indistinguishable from those that arise from polyps. "If we had not intervened, if we had missed [the nonpolypoid adenomas], some of them would have become invasive cancers, and by that time we wouldn't know where they had come from, because they would have gone through the transformation to become bulky and invasive," says Dr. Roy Soetikno from the Veterans Affairs Palo Alto Health Care System and Stanford University, lead author of the JAMA study.
The overall prevalence of nonpolypoid colorectal neoplasms (NP-CRN) in the general population remains unclear, and scientists do not know if these types of adenomas grow or recur faster than the more common polypoid lesions. In an editorial accompanying the paper in JAMA, Dr. David Lieberman from Oregon Health and Science University writes that polypoid and nonpolypoid neoplasms missed during screening "may represent the most common explanation for interval cancers," that is, cancers that arise in between scheduled colonoscopies or other screening tests.
However, explains Dr. Barry Kramer, associate director for disease prevention at the National Institutes of Health, "we really don't know, because we really can't be confident about the natural history of these lesions. All we have at this point are cross-sectional studies; that is, what appears in the colon at the time of colonoscopy or sigmoidoscopy. If we're aware of polyps or flat adenomas [during screening], we take them out. And so we lose our ability to learn, at least with precision, what the natural history is.
"That's a gap in our knowledge at this point," he continues. "It will also be useful to know if there are differences in the molecular fingerprints between these lesions and the usual [polypoid] adenomas. If there are, that might help us predict the behavior of a given lesion, and that's an important area for research."
Two traits of NP-CRN agreed on by investigators are that they are more difficult to detect and more difficult to remove. Unlike polyps, which can be cut away from the intestinal wall fairly easily, removing NP-CRN involves a multi-step procedure called mucosal resection.
By training with Japanese endoscopists and studying videos of NP-CRN cases, Dr. Soetikno's team learned to look for the characteristic features of NP-CRN, which include a slightly red appearance, altered or absent vascular network, friability, and wall deformity. He believes that any interested physician can learn to recognize the lesions. "You need to have an imprinting of the shapes, of the color, in your mind…if people are willing to spend the time and look at [training] movies and really imprint them in their minds, I think people can learn."
His research group plans to make their training materials freely available to interested endoscopists through the American Society for Gastrointestinal Endoscopy. "The technique of mucosal resection also needs to be disseminated, so the benefit of finding these flat lesions can be maintained," he adds.
Another screening test called virtual colonoscopy - also known as CT colonography - which uses computed tomography (CT) to visualize the GI tract noninvasively, has been tested recently in clinical trials.
While researchers are debating how to optimize CT colonography to better detect truly flat or depressed lesions, Dr. Perry Pickhardt, associate professor of radiology at the University of Wisconsin Medical School, believes that most "lesions the JAMA paper describes are things that we see routinely, and with current techniques we really don't have much problem finding those lesions. I think awareness is the main thing, and that's a very important message: be aware of these."
"We're still developing techniques to optimize both colonoscopy and CT colonography…as there's increasing awareness that [nonpolypoid lesions] exist and are relatively common," says Dr. Kramer.
"The future of screening for colorectal neoplasms is to detect and remove all neoplastic lesions: polypoid and nonpolypoid. By having data to show the existence and importance of the flat and depressed lesions in the United States, we can alert all endoscopists," said Dr. Soetikno. "Our patients, referring physicians, and insurers expect that when we give a patient a clean bill of health, we do not leave any neoplasms behind."
Back to Top |