|
 |

|
Print  Download Reader
Download Reader 
|
|
|
Print Download Reader
Testimony
Wednesday, February 8, 2006 Introduction New Medicare Prescription Drug Benefit Delivers Drugs and Savings to Millions According to CMS� Office of the Actuary, Medicare�s drug coverage will have significantly lower premiums and lower costs to federal taxpayers and states, as a result of stronger than expected competition in the prescription drug market. Moreover, beneficiary premiums are now expected to average $25 a month � down from the $37 projected in last July�s budget estimates. The Federal government is now projected to spend about 20 percent less per person in 2006 and, over the next five years, payments are projected to be more than ten percent lower than first estimated, so taxpayers will see significant savings. And state contributions for a portion of Medicare drug costs for beneficiaries who are in both Medicaid and Medicare will be about 25 percent lower over the next decade. All these savings result from lower expected costs per beneficiary; projected enrollment in the drug benefit has not changed significantly. Since the new prescription drug benefit began January 1, 2006, enrollment is off to a strong start. As of mid-January, nearly 24 million people with Medicare now have prescription drug coverage and tens of thousands are enrolling every day. Pharmacists across the nation are filling a million prescriptions each day for people with Medicare. Nationwide, pharmacists are processing more than 40,000 Medicare prescriptions an hour during peak hours as hundreds of thousands of people with Medicare are now getting help with their drug costs each day. In the first 10 days, over three million prescriptions were dispensed to Medicare beneficiaries in nursing homes. And pharmacists across the country are reporting to CMS that people who did not have good coverage previously are now no longer struggling with their drug costs. For example, one pharmacist told us how, for the first time, he didn�t have to advise his Medicaid patients about which prescription he couldn�t fill completely because of Medicaid coverage limits. Pharmacies have, though, had difficulty filling prescriptions for certain beneficiaries eligible for both Medicare and Medicaid (dual eligibles), and some states have turned their state billing systems back on to help cover medications needed in these situations. We have put in place a demonstration project to reimburse states for the direct and administrative costs they have incurred since the initiation of the drug benefit, in temporarily filling this coverage gap for dual eligibles transitioning from Medicaid to Medicare drug coverage and are working with them to fully resolve this issue. As part of this demonstration, CMS will reconcile with the drug plans to ensure that they pay for covered drugs. Many reports from people who are getting their drugs under the new prescription drug benefit, however, are very positive. One man wrote, �My drug bill went from $154.28 per month to $34 for the same drugs. That is a 78 percent savings! I chose a program that had no deductible so I would not have to wait to spend $250. After paying the monthly fee of $39.50, my savings per month is 52.7 percent. Tell me I didn't get a good dea...� Enrollment Status Update
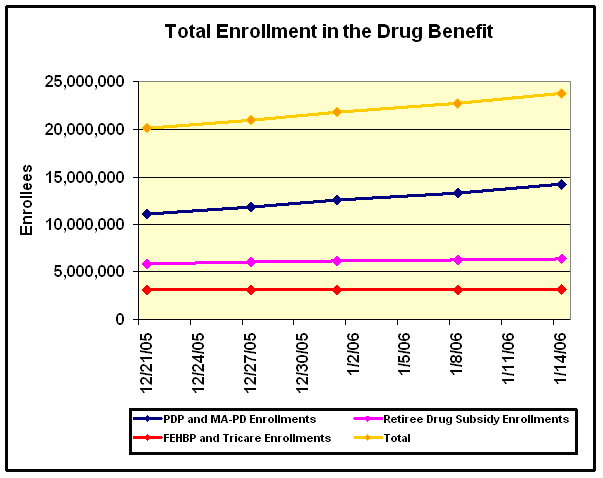
Between mid-December and mid-January, more than 2.6 million people have signed up for the new stand-alone prescription drug coverage. This number is on top of the 1 million who enrolled in stand-alone plans in the first 30 days of the initial enrollment period. An additional 4.5 million individuals, including 600,000 full benefit dual eligible individuals are enrolled in a Medicare Advantage plan. Overall, about 6.2 million full benefit dual eligible individuals, including those enrolled in a Medicare Advantage plan, have transitioned to Medicare prescription drug coverage. In addition, Medicare�s retiree drug subsidy will reimburse a portion of drug costs incurred by at least 6.4 million retirees for 2006. Also, an estimated 1 million retirees are in employer- or union-sponsored coverage that incorporates or supplements Medicare�s coverage. Another estimated 500,000 retirees are continuing in other employer or union coverage. An additional 3.1 million Medicare eligible retirees are receiving their coverage through TRICARE for Life or a Federal Employee Health Benefit Plan. Tens of thousands of beneficiaries continue to enroll every day. CMS Works to Resolve Start-up Challenges
CMS recognizes the enormity of this transition and has been working intensively for many months with partners in and out of government, including States, plans, pharmacists, advocates, and other key partners to ensure the transition process is as smooth as possible for people with Medicare and all of our partners. Since the beginning of the year CMS has taken the following key actions to address our implementation challenges.
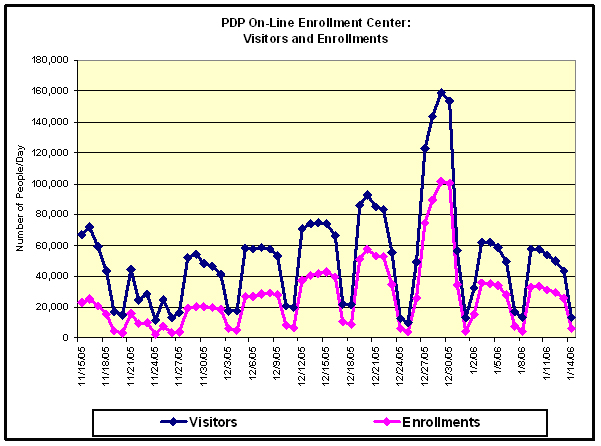
As a result of these and other efforts, which we describe in more detail below, we are not seeing nearly the extent of start of the month issues as we did in January. We are seeing improvements on a daily basis as more people with Medicare receive their enrollment confirmations and their personal information is available in CMS� databases, which allows easy payment for their prescriptions. However, despite these efforts, we are very concerned that some people with Medicare have had difficulty accessing their drug coverage for the first time, in particular certain dual eligible beneficiaries with Medicare and Medicaid. These problems generally do not occur for people who completed their enrollment well in advance of the beginning of the month and received their drug benefit card before filling any prescriptions. Additionally, many of these initial problems have been relatively straightforward to resolve. For example, one woman stated on January 10, 2006 that she did not immediately receive her plan card although her husband received his from the same plan after enrolling at the same time. When she contacted the plan, the problem was quickly resolved. After getting her prescriptions filled, she reported, �I normally spend $538 for a three-month supply of my drugs. But this time it cost only $278. And these weren't even generic drugs.� After people use the system once, these initial problems that some beneficiaries have faced do not recur. We have been most concerned about helping dual eligible individuals use the new Medicare benefit. While the vast majority of the more than 6 million full benefit dual eligible individuals have already begun to use Medicare drug coverage, certain of these full benefit dual eligible individuals have had initial difficulties. In particular, the small number of full benefit dual eligible beneficiaries who switched plans towards the end of 2005 after their initial auto-enrollment did not have complete information available on their new plan�s coverage in early January. In addition, information transfers among states, CMS, and plans did not occur perfectly for all beneficiaries who changed plans. CMS is committed to ensuring that all beneficiaries receive their needed prescription drugs, and as outlined below, is taking steps, in conjunction with States to assure this happens. CMS worked with numerous partners leading up to the start of the drug benefit to educate beneficiaries and their caregivers about the Medicare prescription drug benefit. We, along with the plans, pharmacists, States, and hundreds of other partners, helped people understand how to make decisions about their prescription drug coverage based on cost, coverage and convenience. As a result of our successful outreach efforts, we experienced a substantial surge in enrollment at the end of the year and many full benefit dual eligible individuals elected to change plans close to December 31, 2005. As shown in Figure 2, both visitors to the prescription drug plan on-line enrollment center and enrollments rose steadily throughout December and peaked at the end of the month with over 100,000 enrollments on both December 29 and 30, 2005. CMS continues to see tens of thousands of new enrollments daily.
CMS Plans for Implementation of Drug Coverage on January 1, 2006 for Individuals Eligible for Both Medicare and Medicaid CMS Worked With States CMS also has worked with States through various workgroups to assure that States report and CMS knows of every dual eligible beneficiary in the country undergoing this transition from Medicaid to Medicare drug coverage. In addition the CMS and State workgroups collaborated to
In addition to the ongoing efforts of the State Issues Workgroup, CMS engaged the States in a series of summits, conference calls, and workshops to discuss and address implementation issues associated with the MMA. These gatherings include monthly all-State conference calls; State Pharmacy Assistance Program (SPAP) Workgroup conference calls; and conferences hosted by organizations representing the States including the National Governors Association, National Conference of State Legislatures, and Council of State Governments. In addition, CMS provided States with:
Finally, CMS has worked diligently with States to appropriately identify their full benefit dual eligible individuals. CMS validated the information that States reported to minimize reporting errors, mistakes, and omissions that may affect the identification of the States� full benefit dual eligible residents. These validation data matches achieved rates of over 99 percent for all States, according to an independent evaluation completed in the fall of 2005. CMS Automatically Enrolled Full Benefit Dual Eligible Individuals into Plans Also, while other individuals generally have the opportunity to change plans only at the end of the calendar year, dual eligible individuals have the opportunity to change plans at any time. This flexibility ensures continuity of care when Medicaid prescription drug coverage ends, while also allowing them to select a plan that best meets their needs. CMS also has worked with States to identify and auto-enroll individuals who are about to become full-benefit dual eligible prior to the end of their Medicaid drug coverage to work toward a seamless transition on an on-going basis. This includes those Medicaid individuals who will age into Medicare or who will reach the end of the 24-month Medicare disability waiting period. CMS Developed New and Enhanced Information Technology Systems for the Prescription Drug Benefit Staff created and modified a variety of complex, integrated systems that currently interact with the private and public sectors to implement the new benefits. These IT systems support the key critical business processes that CMS uses to manage the Medicare Advantage and prescription drug benefit programs. The integrated system provides CMS with the ability, among other things, to enroll people with Medicare into prescription drug plans, make payments to plans, and ensure that beneficiaries receive their drug coverage. The integrated information technology system also allows CMS to pay the Retiree Drug Subsidy to approved plan sponsors and track True-Out-of-Pocket Expenses (TrOOP � costs borne by the enrollee) for people with Medicare. In addition, the updated systems ensure the correct premium amount is either paid directly to the plan or provided to the Social Security Administration to withhold from a beneficiary�s Social Security check. Through contracts with telecommunications clearinghouses that currently service the majority of retail pharmacies, the pharmacies will be able to perform real-time eligibility determinations and will be able to route claims to primary, and if applicable, secondary plans for proper adjudication to accurately coordinate benefits. The new and modified systems also were designed to ensure only authorized individuals have access to Medicare information. CMS worked closely with industry experts to implement nine system modules. Implementation included application development and integration efforts, system engineering activities, and validation and testing. In order to meet the deadlines, CMS worked creatively and collaboratively to compress what would ordinarily be an 18 to 24-month systems development process. CMS ensured that the necessary computer and network capacity and capabilities were in place as the CMS IT applications came online. These enhancements included
CMS implemented backup and parallel support systems to minimize any vulnerabilities, and also oversaw the implementation of a secure, Internet-based computing environment in the CMS data center. If these systems had not come online on schedule, CMS would not be able to enroll beneficiaries or pay the health plans that are administering the new benefit. CMS set new standards for documenting requirements, program management, managing change, testing systems, and documenting and ensuring that system development life cycle reviews were undertaken. Extensive Plan Formulary Requirements Provide Access to Needed Prescription Drugs In addition, each Medicare prescription drug plan�s formulary was developed and reviewed by the plan�s pharmacy and therapeutics committee. Each formulary must be consistent with widely used industry best practices. Furthermore, CMS compared the prescription drug plans� use of benefit management tools to the way these tools are used in existing drug plans to ensure they are being applied in a clinically appropriate fashion. Prescription drug plan formularies typically include upwards of 80 percent of the 100 most commonly used drugs. CMS has developed exceptions procedures designed to ensure that enrollees receive prompt decisions regarding whether medications are medically necessary. For example, if the enrollee is requesting coverage of a non-formulary drug, the drug may be covered if the prescribing physician determines that all of the drugs on the formulary would not be as effective as the non-formulary drug or would have adverse effects for the enrollee, or both. The plan would have to review the physician�s determination and must make its decision as expeditiously as the enrollee�s health condition requires after it receives the request, but no later than 24 hours for an expedited coverage determination or 72 hours for a standard coverage determination. CMS Required Plans to Have a Transition Process for All Individuals CMS Worked Toward Achieving a Smooth Transition in Long Term Care Facilities There are 1.6 million people with Medicare who are residents in 15,800 nursing homes throughout the nation. A majority of individuals in long term care facilities are Medicare beneficiaries, many of them are dual eligible. Individuals in LTC facilities represent a unique and vulnerable population because they have cognitive and/or functional impairments. This population typically has multiple co-morbidities, the highest utilization of drugs, with an average of nine medications per day, and the highest spending for prescription drugs compared to other people with Medicare. In March 2005, CMS issued guidance for the implementation of CMS requirements regarding pharmacies that provide products and services to individuals in LTC facilities. This guidance addressed pharmacy performance and service criteria, convenient access standards, formulary considerations, and other beneficiary protections that prescription drug plans should consider as they develop their prescription drug benefit offerings for people with Medicare in LTC facilities. Auto-enrollment of Individuals in LTC Performance and Service Criteria for Pharmacies Providing LTC Service
For example, network LTC pharmacies (NLTCPs) must have the capacity to provide specific drugs in unit of use packaging, bingo cards, cassettes, unit dose or other special packaging commonly required by LTC facilities. NLTCPs must have access to or arrangements with a vendor to furnish supplies and equipment including but not limited to labels, auxiliary labels, and packing machines for furnishing drugs in such special packaging required by the LTC setting. Additionally, NLTCPs must provide on-call, 24 hour a day, 7 day a week service with a qualified pharmacist available for handling calls after hours and must have medication dispensing capability available for emergencies, holidays and after hours of normal operations. Prescription Drug Plan Formularies for LTC residents CMS recommended nursing homes include a 90 to 180 day transition period to accommodate the needs of Medicare beneficiaries residing in long-term care facilities. The vast majority of plans are providing 90 day transition periods with many offering the option of extending to180 days. However, the LTC emergency first fill policy is unique to this setting and continues throughout the entire year for any off-formulary prescription written. In addition, plans are required to cover drugs as written during the 7 to 14 days allowed for initial exceptions and appeals process. CMS Provides Education Regarding LTC Pharmacy Requirements CMS also provided and continues to provide instruction through trade association newsletters, fiscal intermediary newsletters and conferences. In addition, CMS developed electronic messages that are shown to facilities each time they enter data on the Minimum Data Set (MDS) - part of the federally mandated process that provides a comprehensive clinical assessment of all residents in Medicare and Medicaid certified nursing homes. Education efforts included, for example, a three pronged approach for ensuring that nursing home residents who are in the process of spending down their assets to qualify for Medicaid, simultaneously apply for Medicaid and the low income subsidy and enroll in a PDP to maximize their prescription drug benefits. This outreach also included numerous Open Door Forums, in which all stakeholders were invited to participate so CMS could share the outcomes of critical policy and procedural decisions and to solicit feedback on areas of concern. CMS Educated and Coordinated Outreach Efforts for Pharmacies Direct Communications: CMS made extensive efforts to directly reach pharmacists in preparation for January 1, 2006. CMS created the Medicare Rx Update as a periodic update to pharmacists to ensure they are well informed about the details of the Medicare prescription drug benefit implementation. CMS distributed the Rx Updates through the internet to directly reach practicing pharmacists with highlights and clarifications about implementation issues. Since its inception in May 2005, CMS has sent 25 Rx Updates to the pharmacy community addressing topics including the pharmacists� role with the low income subsidy, marketing guidelines, the prescription drug plan compare tool, and the true-out-of-pocket (TrOOP) facilitator. With thousands of subscribers and because State and national organizations distribute the Update as well, these bulletins have gone a long way toward educating the pharmacy community about the procedures related to the new benefit. CMS also created and maintains a website (http://www.cms.hhs.gov/Pharmacy/) specifically for pharmacists. In addition to the Medicare Rx Updates, the pharmacist website contains informative prescription drug benefit guidance, links to training materials, information for special practice pharmacies, and more. CMS� pharmacist outreach team, which includes our regional pharmacists, has conducted the most targeted personal outreach. CMS' central office pharmacy team, which includes 21 pharmacists, as well as the pharmacists and staff from CMS' 10 regional offices, have traveled the country educating pharmacists in all practice settings about the new benefit. The pharmacists have presented at hundreds of events and gatherings reaching tens of thousands of pharmacists. Furthermore, CMS created a forum known as the Pharmacy Information Exchange, a periodic open phone town hall style meeting. Hundreds of pharmacists attended calls hosted by CMS' pharmacists. These calls have enabled CMS to present on relevant topics, answer many questions and identify new issues from the community. Finally, CMS has developed two pharmacist-specific continuing education programs that were distributed through the on-line arm of Drug Topics, the magazine dedicated to the profession of pharmacy, and through Kansas University, respectively. Plans to Address Pharmacy Operational Issues: Finally, as January 1, 2006 approached, CMS finalized a comprehensive plan for further pharmacist training, including materials targeted to explain technical details of the TrOOP facilitation process, Medicare Part B versus Part D coverage, out-of-network policies for Hurricane Katrina evacuees, the point-of-sale facilitated enrollment process for full benefit dual eligible individuals, and more. CMS is working directly with a wide range of pharmacy organizations, identifying operational questions for pharmacists and developing dynamic action plans on how to anticipate problems and, to the extent that we can, address them in advance. In preparation for the first days of the benefit, CMS engaged the pharmacy community on a daily basis so that the Agency could work directly with the industry to provide direct assistance for any issues that arose in the early days of implementation. CMS Worked With Physicians Point-of-Sale System Facilitates Enrollment Beneficiaries, who present at a pharmacy with evidence of both Medicaid and Medicare eligibility, but without current enrollment in a prescription drug plan, can leave the pharmacy with a filled prescription and the claim for their medication submitted to a single account for payment. A CMS contractor will immediately follow up to validate eligibility and facilitate enrollment of the full-benefit dual eligible individual into a prescription drug plan. CMS has provided information on the WellPoint system to pharmacy associations, plans, and individual pharmacies. This information describes how the process of POS-facilitated enrollment starts at the pharmacy with the pharmacist verifying dual eligibility and billing a special WellPoint account in order to ensure that the individual with Medicare receives the prescription. CMS Takes Action to Ensure Timely Receipt of Prescription Drugs after Start of Benefit CMS Works to Ensure Emergency Fills for Dual Eligible Individuals CMS Educates People with Medicare About the Timing of Selecting a Plan Generally, if an individual newly enrolls in a plan, or switches to a different plan by the 15th of the month, their information should be available at the pharmacy by the beginning of the next month. So we have begun encouraging people with Medicare to enroll at least a few weeks before they expect to need drug coverage, and to be prepared to wait several weeks to be fully entered into the system and our data show that message is getting through. In the last half of December, hundreds of thousands of individuals who were auto-enrolled elected a different plan, compared to about 24,000 during the last week of January. We are developing model language for plans to use to inform their enrollees of these facts, and will also provide those who enroll through our 1-800-MEDICARE call centers and our internet-based Plan Finder tool with a similar notice. Enrollees will also be informed that while waiting for the data systems to be appropriately modified, they may, if need be, use the acknowledgement letter sent to them by the plan when they go to the pharmacy to fill their prescriptions. CMS Supports Ongoing Success of IT Systems
Based on these evaluations, CMS has identified, in priority order, key performance and operations issues. The resolution and implementation of the solutions is underway. CMS has taken steps to ensure plans have the means to cross-check CMS data with plan data for improved accuracy and completeness to ensure that dual eligible individuals can be appropriately identified when they present at the pharmacy counter. On January 13, 2006 and again on January 18, 2006, CMS sent files to each plan with information about its dual eligible enrollees along with instructions on how to process these files. As these data are processed by plans, this process is substantially reducing the workload of the pharmacists and assisting the vast majority of dual eligible individuals in getting their drugs. Providing this information enables pharmacists to identify plans in which dual eligible individuals are enrolled and ensure that correct and appropriate co-payments are charged to the individual with Medicare. Furthermore, on January 30, 2006, CMS sent an additional file of low income subsidy eligible individuals, this time using an enrollment effective date of February 1, 2006. This file should provide an additional source of information for many of the plan changes that have taken place in the past couple of weeks and help plans prepare for enrollments that are effective beginning in February. CMS also has been working with specific plans to resolve their unique issues surrounding sending and receiving data files from CMS. As a result of these efforts, dual eligible beneficiaries who had been having difficulty with correct co-payments and eligibility are now getting their prescriptions filled correctly. To ensure CMS� performance evaluation system and corrective actions are effective, CMS contracted with Electronic Data Systems (EDS) as an independent reviewer to help resolve specific data translation issues with the plans, States, and pharmacies. CMS Improves 1-800 MEDICARE Call Center to Reduce Wait Times
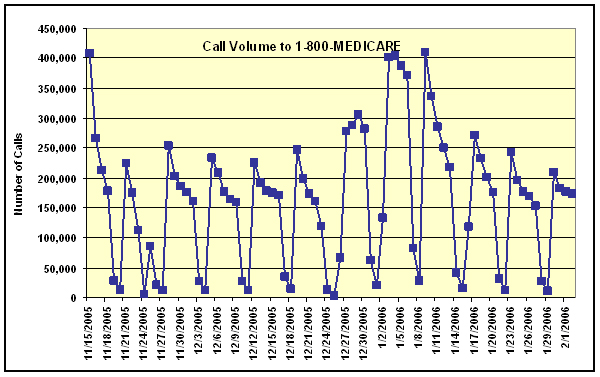
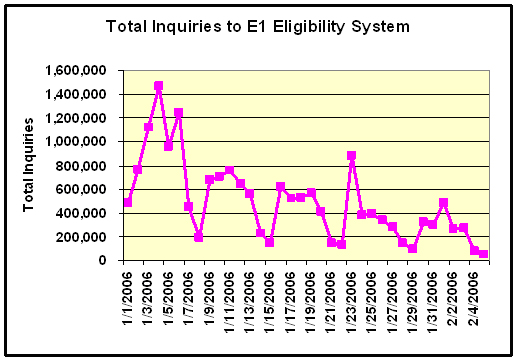
On average, callers have experienced wait times of less than two minutes from mid-November to mid-January, with longer waits sometimes occurring during peak call periods. CMS has increased the number of CSRs from 3,000 in June of 2004 to as many as 7,800 to handle beneficiary calls. We have also acquired additional infrastructure including telephone lines, workstations, and seats at call center sites. We have upgraded our CSR scripts by reducing redundant information, indexing scripts for quick access, and including probing questions to help the CSRs better identify the caller�s concerns. CMS has implemented a major enhancement through the use of Smart Scripts, which provide the CSRs with an easily followed path of responses to the most frequently asked questions. Smart Scripts are a new type of script that has hyperlinks built into the body of the text that when activated will take the CSR directly to related information about that subject. In addition, we have CSRs participate in the content workgroups for the actual development of scripts and job aides. CMS also has implemented a CSR feedback system and streamlined our approval process for updating the scripts in a timely manner to respond to the changing needs of our customers or to incorporate policy updates. CMS hired and trained additional staff to exclusively use the Prescription Drug Plan Finder (PDP) tool to handle only PDP calls. All CSRs receive one week of classroom training followed by two or three additional days of practice calls, simulation, quality monitoring and follow-up coaching to ensure peak performance. CSR certification with a written examination and test calls is required prior to taking live calls. Calls are being handled on an in-bound basis and steps CMS has taken to strengthen the call centers� capabilities and reduce wait times have made it possible to address beneficiaries� concerns as they arise. CMS customer satisfaction surveys indicate that the bulk of callers who interact with our CSRs, 84 percent, are satisfied with their experience. They are particularly pleased with how courteous and patient the CSRs are (rated at 97 and 95 percent, respectively). These responses came not only from people with Medicare, but also friends or relatives calling on their behalf, who made up 48 percent of callers during December, 2005. CMS� Medicare website, www.medicare.gov, has also been a source of useful information for people with Medicare. Since the first of the year, our frequently asked questions have been accessed more than 530,000 times. CMS has also responded to over 5,300 e-mails received through the site, with 93 percent of them being resolved satisfactorily in the first response. CMS Works with Plans to Improve Their Customer Service We have also informed plans that they must comply with their transition policies so that enrollees who require a specific medications are able to obtain coverage for a one-time supply of those drugs, while they work with their physician and plan to select a new drug in the same therapeutic class, or appeal for coverage of their existing prescription. CMS also required plans to inform their CSRs about their transition policies and empower them to permit a pharmacy to dispense these drugs. Most recently, we have notified plans, letting them know that the 30 day transitional coverage period would be extended another 60 days, to provide enough medications to their enrollees while implementation challenges are resolved. CMS Takes Steps to Identify Areas of Concern CMS began development of the CTM in the fall of 2005 and refined the system in response to input from various stakeholders. The design of CTM format and content were driven from previous experience with the Drug Card, intra-agency components, and insights from the Pharmacy Benefit Management (PBM) Industry. CMS launched the CTM into production on October 3, 2005. Since this time, the CTM has been fully tested to accept large numbers of daily transactions simultaneously from many users across the Agency. CMS began tracking complaints in January and although this process is still in the early stages, we have seen a general decline in complaints. CMS Provides Caseworkers for One-on-One Counseling CMS has established a system to help resolve urgent issues on a case-by-case basis. CMS has hundreds of trained caseworkers who are working as rapidly as possible with individuals with Medicare and plans to resolve urgent issues to help ensure that people with Medicare get their prescriptions filled. CMS urges people with Medicare or their family members who are having difficulties to call 1-800-MEDICARE, and if necessary, their case will be forwarded to our caseworkers. Urgent cases have high priority for rapid resolution. While the number of individual cases is small in comparison to the millions of prescriptions and individuals who are successfully receiving their prescriptions, CMS is committed to ensuring that every individual receives their needed medicines, are properly identified, and are charged the appropriate co-pays in the future. CMS Provides Dedicated Support to Pharmacists CMS has significantly increased the capacity of the toll-free pharmacy support phone lines to help resolve issues pharmacists encounter in dispensing medications to those newly enrolled in the Medicare prescription drug plans. CMS has increased its call handling capacity at the pharmacist help line 30 fold and the line is now available 24 hours a day. We have increased the CSR staffing to support this initiative from 150 CSRs to about 4,500. The increased capacity has reduced the wait time to less than a minute for pharmacists who want to use this mode of communication for eligibility and enrollment determination. CMS Responds to Early Technical Problems with the Eligibility and Enrollment Query System for Pharmacists During the first week of the Medicare prescription drug program, CMS experienced some delays in response time with the new computer tool provided to pharmacists for real time enrollment and eligibility look-up. Working with our contractor, CMS has improved response time to less than one second with no delays. CMS continues to load data into this system from information obtained on individuals� recent enrollment or plan switching activity, which will help pharmacists obtain complete enrollment and billing information on more individuals when they use the E1 system at the pharmacy counter. As shown in Figure 4, CMS is seeing an overall decline in the number of times pharmacists must utilize the E1 system from a high of 1.47 million to about a half million in recent days. This reflects a more efficient and effective use of the system after CMS issued a tip sheet in early January on how best to use the system. In addition, more individuals have received appropriate plan identification information, so the need for the E1 system has declined.
In addition, pharmacists are reporting that they are experiencing improvements in their ability to query and obtain information from the E1 eligibility transaction system. One pharmacist noted on January 11, 2006, �I wanted to take the opportunity to tell you that our 434 pharmacies have found the (E1) system very helpful and we have seen the system's �integrity� improve significantly from January 2, 2006 to today.� CMS Addresses Issues Between Plans and Pharmacies Typically, under Medicaid, pharmacists were paid on a weekly basis. Most of the drug plans use a somewhat longer payment cycle and pharmacists have expressed concern over when they will be paid. We recognize this concern and want to let pharmacists know that we are aware of it. As we look forward to renewing plan's contracts for 2007, a plan's working relationship with its network pharmacies will be an important factor in our assessment of whether the plan has sufficient personnel and systems in place to effectively administer and manage its operations. CMS continues to hold regular one-on-one calls with the plans to identify issues and solutions. CMS is in constant communication with the plans pertaining to issues as they arise, and the Agency has developed a collaborative process whereby CMS organizes calls with plans and their pharmacists to resolve problems as quickly as possible. ICMS Continues Extensive Outreach to Pharmacists
In addition, CMS is holding weekly conferences with pharmacy associations that help CMS distribute information and educate pharmacists to ensure they have the most complete and up-to-date information possible. Also, CMS is communicating on a daily basis with both chain and independent pharmacies. Pharmacists in CMS� ten regional offices are working directly with local pharmacies, pharmacists, and pharmacy associations to identify troubling trends and specific problems. CMS is working closely with the National Association of Chain Drug Stores (NACDS), the National Community Pharmacist Association (NCPA), the American Pharmacists Association (APhA), the National Council of State Pharmacy Association Executives (NCSPAE), the American Society for the Automation of Pharmacy (ASAP) and other groups to help communicate with and educate their membership. CMS Continues Outreach with Physicians In addition, CMS sent a letter to physicians outlining specific sources of help and information including the following.
CMS Continues Collaboration with States In an effort to assist State Health Insurance Assistance Programs (SHIPs) with their backlog of beneficiary calls, CMS created a virtual call center comprised of over 150 staff from CMS, and the Administration on Aging (AoA). CMS and AoA returned thousands of calls to answer beneficiary questions and assist in finding a prescription drug plan to best fit their needs. CMS Establishes Reimbursement Plan for States that Cover the Cost of Dual Eligible or Low-Income Subsidy Entitled Individuals CMS is working with the States to ensure all dual eligible individuals are able to leave the pharmacy with the drugs they need. In addition, pharmacies need to continue to work with the plans to sort out start-up issues as quickly as possible. However, some States are reporting that dual eligible individuals have been charged the wrong cost sharing amounts when they have gone to the pharmacy and some have left the pharmacy without their drugs. Certain States have taken steps to help their dual eligible and other low-income subsidy entitled beneficiaries by using their State system of reimbursement to pharmacies. These States are now paying for prescriptions that should be paid for by the prescription drug plans, and, if States have stepped in they will be reimbursed. On February 2, CMS sent a letter to all state Medicaid Directors, and State Pharmacy Assistance Program Directors to inform them of a new Medicare demonstration project to defray specific costs they have incurred surrounding the implementation of the Medicare prescription drug benefit. Specifically, the demonstration permits Medicare payment to be made to States for costs they have incurred for medications covered under the drug benefit, including transitional supplies, for both dual eligible and low-income subsidy entitled plan enrollee's, to the extend that those costs are not otherwise recoverable from a drug plan and are not the Medicare beneficiary's cost sharing requirement. Under this demonstration, States will submit to CMS information on claims they paid for dual and low-income subsidy entitled individuals and CMS will work to ensure that prescription drug plans reimburse States for those expenses up to the amount they would otherwise have paid. The Federal government will reimburse States for any differential between plan reimbursement and State payment, as well as for certain administrative costs for paying the State claims and facilitating the correct enrollment of dual and low-income subsidy entitled individuals into a prescription drug plan. States will work with CMS to help obtain accurate beneficiary information on drug spending. They will also use payment approaches that support pharmacists� efforts to primarily bill the Medicare prescription drug plans and ensure the use of the Medicare point-of-sale billing before relying on State payment such that states serve as a payer of last resort. The demonstration requires States to make significant progress by February 15, 2006, toward turning off their State reimbursement systems and supporting beneficiaries and pharmacists in using the Medicare prescription drug system, based on best practices identified by the States and CMS. With input through a State workgroup, CMS developed a template to apply for this demonstration for use by those States. The template was made available on February 2. In addition to providing reimbursement to the States, the demonstration will include timely data sharing and claims identification features. States that participate should provide timely summary information on claims incurred, including summary amount and beneficiary identification information, to facilitate reconciliation and beneficiary transition to prescription drug plans. States should also work with CMS to provide valid data on any set of beneficiaries who may not have been included properly in the State�s previous dual eligible files. Also, States should separate claims for the transition period from claims the States would have otherwise paid through a separate State program. In some States, the State has elected to pay all cost sharing, for example, on behalf of some individuals who would otherwise have paid a co-payment. Under the demonstration, plans, and then Medicare, will reimburse State paid claims previously incurred and up to and through the anticipated end date of this demonstration of February 15, 2006. CMS will continue to work closely with the States, as we have been, to resolve temporary transition issues and make sure people with Medicare can get the new prescription drug coverage if they want it. Medicare Prescription Drug Benefit Significantly Less Expensive than Expected Savings are not coming because enrollment is low. As discussed earlier, we are well on our way to meeting our projected enrollment figures. The savings are coming as a result of lower than expected per-beneficiary costs. Hard data that we now have, not simply estimates, tell us that the average monthly premium will be $25, only 68 percent of the $37 figure we had originally estimated. The net cost to the Federal government for the drug coverage in 2006 is expected to be $30.5 billion down from a previously estimated $38.1 billion. The actual or �net� costs to the Federal government, accounting for Medicaid savings, are also significantly lower over 10 years, dropping from last year�s estimated $737 billion to $678 billion. For the 10-year period from 2006-2015, the �total� Medicare drug benefit cost, without accounting for the Medicaid impact, is now estimated to be about $130 billion less - $797 billion compared to an estimated $926 billion last year. State government will also see significant savings as a result of lower than expected phased-down contributions for the drug coverage. The state payments are now projected to be $37 billion (27 percent) less over a 10-year period. The Medicare Modernization Act included the phased-down contributions, sometimes known as �clawback� payments, to account for a portion of the costs that states had previously paid for Medicare beneficiaries who are also in Medicaid, because they are now getting their drug coverage from Medicare. CMS Continues to Work Hard to Ensure the Most Important New Benefit in 40 Years Delivers Drugs to People with Medicare To summarize, as I have laid out above, we are focusing on the following:
As the New York Times noted in 1966 when Medicare debuted, �This great new experiment must be given ample time to get over its growing pains.� CMS is confident that we too will overcome our �growing pains� as we continue to address the challenges set before us implementing the new Medicare prescription drug benefit. We are especially encouraged by the latest figures demonstrating that the projected costs of the new benefit are less than we had anticipated. I would be happy to answer your questions. Last Revised: February 8, 2006 |