ISSN: 1080-6059
Volume 13, Number 1–January 2007
Letter
Cryptococcus gattii Risk for Tourists Visiting Vancouver Island, Canada
Jens Lindberg,* ![]() Ferry Hagen,† Alex Laursen,*
Jørgen Stenderup,‡ and Teun Boekhout†§
Ferry Hagen,† Alex Laursen,*
Jørgen Stenderup,‡ and Teun Boekhout†§
*Skejby Hospital, Aarhus, Denmark; †CBS Fungal Biodiversity
Center, Utrecht, the Netherlands; ‡Herning Hospital, Herning, Denmark; and
§University Medical Centre, Utrecht, the Netherlands
Suggested citation for this article
To the Editor: An unprecedented outbreak of Cryptococcus gattii genotype amplified fragment length polymorphism (AFLP) 6/VGII on Vancouver Island, British Columbia, Canada, is affecting both human and animal hosts with normal immunity (1–3). So far, >100 human cases, including at least 6 fatalities, have been reported by the British Columbia Centre for Disease Control (4), (www.bccdc.org, www.cbc.ca). Vancouver Island is a major tourist destination, with ≈7.5 million visits each year (www.bcstats.gov.bc.ca). We report the first known intercontinental transmission of C. gattii from this outbreak in a tourist from Denmark who visited Vancouver Island. This case indicates a potential risk for tourism-related acquisition.
A 51-year-old, HIV-negative, apparently immunocompetent man from Denmark, with known psoriatic gout and under treatment with a nonsteroidial antiinflammatory drug, was admitted to a hospital in Herning, Denmark, with chest pain radiating to the left shoulder and arm, lasting for 1 day. Six weeks before his admission, he returned to Denmark from a 3-week trip to Canada, during which he visited Victoria and surrounding areas on the eastern coast of Vancouver Island for 7 days. During their stay, the patient and his 3 fellow travelers visited gardens and studied the local natural vegetation.
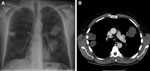 |
Figure. A) Chest radiograph and B) computed tomography scan of the patient showing 3 nodular Cryptococcus gattii infiltrates near pleura. |
During his stay in Canada, the patient had no symptoms, and symptoms had not developed in any of his family members as of October 2006. On admission to the hospital, his temperature was 38.2°C, and a chest radiograph showed 3 large nodular infiltrates suspect for malignancy or abscesses. Neither bacterial nor fungal pathogens could be isolated from sputum by classic and molecular methods. After 4–5 days, his temperature was 40°C, a productive cough with dyspnea was noted, and his condition deteriorated. A chest radiograph showed progression of the infiltrates, and a computed tomography scan of the abdomen and chest showed infiltrates near the pleura, suggesting encapsulated fluid (Figure). An ultrasound-guided lung biopsy was performed, and mucoid material was aspirated. Microscopy and a culture from the aspirate showed a cryptococcal isolate. This isolate was further identified by internal transcribed spacer and D1/D2 sequencing, as well as amplified fragment-length polymorphism analysis (2). In addition, detailed genotyping was performed by using sequences of 7 genes (IGS, CAP10, GPD1, LAC1, MPD1, PLB1, and TEF1; GenBank accession nos. DQ861593–DQ861599) (5).
Extensive molecular research showed that this isolate belonged to the highly virulent AFLP genotype 6A (VGIIa) of Cryptococcus gattii, which is the major genotype involved in the Vancouver Island C. gattii outbreak (1–4). All 7 sequenced genes had a complete match with the sequence types specific for isolates involved in the Vancouver Island outbreak (5). Thus, we conclude that the pathogen was acquired during the patient’s visit to Vancouver Island and imported to Denmark. The presence of 3 cryptococcal masses of more or less equal size suggests that the patient was exposed to a high concentration of infectious cells of C. gattii. The observed incubation time of 6 weeks is shorter than that was previously reported for infections related to the Vancouver Island outbreak (2–11 mo) (4). These observations, in combination with the absence of any known predisposing factor in this patient, such as smoking or treatment with corticosteroids, suggest that this specific AFLP6 genotype of C. gattii is highly virulent (4,5).
This case suggests a potential risk of tourists acquiring cryptococcosis while visiting Vancouver Island. Therefore, we recommend tourists and medical staff of healthcare centers worldwide be alert for symptoms of cryptococcosis after travel to Vancouver Island.
References
- Stephen C, Lester S, Black W, Fyfe M, Raverty S. Multispecies outbreak of cryptococcosis on southern Vancouver Island, British Columbia. Can Vet J. 2002;43:792–4.
- Kidd SE, Hagen F, Tscharke RL, Huynh M, Bartlett KH, Fyfe M, et al. A rare genotype of Cryptococcus gattii caused the cryptococcosis outbreak on Vancouver Island (British Columbia, Canada). Proc Natl Acad Sci U S A. 2004;101:17258–63.
- Hoang LM, Maguire JA, Doyle P, Fyfe M, Roscoe DL. Cryptococcus neoformans infections at Vancouver Hospital and Health Sciences Centre (1997–2002): epidemiology, microbiology and histopathology. J Med Microbiol. 2004;53:935–40.
- MacDougall L, Fyfe M. Emergence of Cryptococcus gattii in a novel environment provides clues to its incubation period. J Clin Microbiol. 2006;44:1851–2.
- Fraser JA, Giles SS, Wenink EC, Geunes-Boyer SG, Wright JR, Diezmann S, et al. Same-sex mating and the origin of the Vancouver Island Cryptococcus gattii outbreak. Nature. 2005;437:1360–4.
Figure
Suggested Citation for this Article
Lindberg J, Hagen F, Laursen A, Stenderup J, Boekhout T. Cryptococcus gattii risk for tourists visiting Vancouver Island, Canada [letter]. Emerg Infect Dis [serial on the Internet]. 2007 Jan [date cited]. Available from http://www.cdc.gov/ncidod/EID/13/1/178.htm
Please use the form below to submit correspondence to the authors or contact them at the following address:
Jens Lindberg, Th. Nielsens Gade 31, DK-7400, Herning, Denmark; email: jens.lindberg@mail.dk
Please note: To prevent email errors, please use no web addresses, email addresses, HTML code, or the characters <, >, and @ in the body of your message.
Please contact the EID Editors at eideditor@cdc.gov
The opinions expressed by authors contributing to this journal do not necessarily reflect the opinions of the U.S. Department of Health and Human Services, the Public Health Service, the Centers for Disease Control and Prevention, or the authors' affiliated institutions. Use of trade names is for identification only and does not imply endorsement by any of the groups named above.
This page posted December 21, 2006
This page last reviewed December 21, 2006
Centers for Disease Control and Prevention, 1600 Clifton Rd, Atlanta, GA 30333, U.S.A
Tel: (404) 639-3311 / Public Inquiries: (404) 639-3534 / (800) 311-3435