Investigation: # 01MI003
Operator Crushed Between a Rotating Barrel and Its Hoist Support Bar
SUMMARY
|
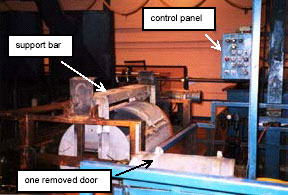
| Figure 1. Operator's Workstation |
RECOMMENDATIONS
INTRODUCTION
On January 20, 2001, an 18-year old male died from crushing head injuries sustained when he was pulled into the hoist support bar of a rotating barrel by the rotation of the barrel. On January 22, 2001, MIFACE investigators were informed by the Michigan Occupational Safety and Health Administration (MIOSHA) 24-hour fatality report system that a work-related fatal injury occurred on January 20, 2001. On February 28, 2001, the MIFACE researcher interviewed the company’s Human Resource Manager. The manager accompanied the researcher into the plant, showed her the incident site and described the metal plating process while she watched the equipment operating. The manager described the events that were thought to have taken place resulting in the fatality.
The MIOSHA investigation resulted in four serious citations: emergency stop not within reach of the operator’s station, guard revolving container where a hazard exists, provide guard for gears, and guard open-sided floor or platform four or more feet above adjacent level.
INVESTIGATION
On Saturday, January 20, 2001, an 18 year-old production worker died as a result of crushing head injuries sustained when he was caught by a rotating barrel and pulled into its supporting frame. On February 28, 2001, a MIFACE investigator visited the site and interviewed the Human Resources Manager, the person responsible for safety in the plant.
The metal finishing company where the fatality occurred had started as a family business. It was purchased from the family in the 60’s by a steel-treating corporation that had been in business 40 years at the time of the purchase. The plant was moved to its present site in the 80’s. This was the first fatality to occur in the corporation since 1927. The company employed 156 people, 100 of whom have the same job title, production worker, as the victim. On the day of the incident five salaried and sixteen hourly employees were at the site.
The company has an arrangement with a temporary manpower agency to hire its clients. If the worker performed satisfactorily on the job for approximately 90 days, then he/she may be hired by the company. The victim had been working at the plant for about three months and was about to be hired by the company. He was familiar with the operation he was running. He had received some safety training at the manpower agency. He received further safety training and on-the-job training related specifically to the equipment operation when he started working at the company.
The victim started work at 0700. The incident occurred at approximately 1000. No one saw or heard the incident occur. Noise levels in the plant require use of hearing protection devices. A fellow worker saw him caught between the hoist support bar of the barrel and the barrel at approximately 10:15 a.m. Police and rescue personnel were called immediately. His body was pried out of the equipment. He was pronounced dead at the scene at 10:31 a.m.
The operator worked at an unload station of a barrel plating operation. In this barrel plating operation, a barrel supported by a hoist dipped small parts into eight coating stations where the parts were coated by plating solution. In order to allow the plating solution to enter and exit the barrel without loss of the parts to be plated, holes are drilled along each side of the barrel. The holes are sized so the parts cannot fall out yet the plating solution can drain.
The barrel approached the operator’s station from the right. The operator’s workstation measures approximately 6 feet by 6 feet and was located 5 feet above the plant floor level. The barrel was approximately the size of a 55-gallon drum, 4 feet in length and 2 feet in diameter. Just before the barrel reached the operator’s station, the hoist placed the barrel on a track that allowed a cart to move the barrel to the station. A ring gear on one end of the barrel engaged a drive motor that rotated it in a clockwise motion. The barrel approached the operator’s station and rotated relatively slowly. Speed of operation was not an issue.
As the barrel reached the operator’s station, a tab located on the barrel opposite the ring gear contacted a wire attached to a limit switch. The limit switch stopped the barrel’s rotation so that two doors on the barrel faced the operator. Each of the two doors was approximately 18 inches square. The operator removed the doors by loosening four 5/8-inch nuts with an impact wrench and removing the nuts. He then lifted the doors off the barrel and set them onto a 28 inch square table to the left of the workstation. He pressed two palm buttons on a 12-inch square control panel located to the right of the workstation to activate the barrel to continue to a dump station eight feet further down the track to the left. The emergency stop for the equipment was located on this control panel.
At the dump station, the barrel rotated and dropped its coated parts onto a conveyor that carried the parts to a drying oven. The barrel continued to rotate to locate the door opening into the correct position for replacement of the doors as it returned to the operator. The limit switch was to have stopped the barrel with the opening for the doors facing the operator. The operator would have replaced the doors and nuts and sent the barrel to the next station by pressing the two buttons on the control panel.
Although no one saw the incident take place, it is presumed that the operator reached into the barrel to remove some parts that had not fallen out at the dump station as the barrel was returning to the operator’s station. The barrel would have been rotating to find its position for the replacement of the doors. It is believed that his sweater became entangled on something inside the barrel, and he was not able to extricate himself. His sweater was torn on the left arm. Apparently the limit switch did not function to stop the barrel from rotating at the unload station. The left side of the victim’s head was pulled into the hoist support bar and crushed between the bar and the rotating barrel. When the equipment was tested after the event, the limit switch did not stop the barrel rotation.
The following safety changes were made to the left side of the operator’s station before the MIFACE investigation:
CAUSE OF DEATH
The cause of death as stated on the death certificate was crushing head injuries. No alcohol or drugs of abuse were detected in the victim’s blood and urine.
RECOMMENDATIONS/DISCUSSION
• Review the design characteristics of the barrel to ensure that parts tumble out freely when it is tilted.
Because of the possibility that the operator was trying to retrieve parts that had not fallen out of the barrel at the dump station, the barrel perforations and size of door opening should be reviewed to insure that the plated parts tumble out unimpeded.
• Guard moving parts at equipment point of operation.
Guards must cover all moving parts in such a way that no part of the operator’s body can come into contact with them. All rotating equipment parts have inherent dangers. Even slowly rotating equipment can grip material it contacts. Where there are protrusions, the potential for catching increases, and the travelling motion of a rotating piece of equipment is a cause for yet greater vigilance. This piece of equipment encompassed all three.
• Allow time at the beginning of each shift for the operator to perform a check of equipment to ensure that all machinery is operating correctly.
Even when management has with the best intentions tried to engineer out all potential safety hazards, situations will occur that require attention. Equipment should be checked by the worker following a safety checklist at the beginning of his/her shift to ensure all equipment is operating as it has been designed to operate. Operators should receive training on using the checklist and be instructed to report any equipment malfunction or repairs needed. Management should ensure that the job will not run until repairs to imminently dangerous conditions are addressed.
• Establish a written schedule for conducting preventive maintenance on critical parts of the system.
A good preventive maintenance plan includes inspection of equipment and machinery that might affect the safety of workers. In this case, the limit switch was a critical part in the system. It was relied upon solely to stop the barrel rotation at the appropriate position for the removal and replacement of the barrel doors. Because of its importance in the operation, the limit switch should have been in top working condition. It is unknown if the limit switch had not functioned properly in the past and/or if the malfunction had not been corrected or inadequately repaired. Keeping records of the number of trouble reports on equipment can help determine the maintenance inspection schedule.
• Place a warning sign on the equipment depicting the potential danger of the body or clothing becoming entrapped in moving portions of the machinery.
The potential hazards of entrapment in rotating, travelling equipment are well-documented. In terms of hazard control, engineering and guarding are at the top of the hierarchy. Warning signs cannot be used in place of the engineering and guarding controls, yet pictorials have been used as safety reminders to workers of the dangers associated with their jobs. A well-designed warning sign depicting the danger of a part of the body or clothing becoming entangled in the equipment would serve as a reminder of the hazard.
• Do not allow operators to wear loose clothing while operating moving equipment.
As described above, the potential hazards of entrapment in rotating, travelling equipment are well-documented. Loose clothing, long hair, and jewelry are often cited as a cause of entanglement.
REFERENCES
MIFACE (Michigan Fatality and Control Evaluation), Michigan State University (MSU) Occupational & Environmental Medicine, 117 West Fee Hall, East Lansing, Michigan 48824-1315. This information is for educational purposes only. This MIFACE report becomes public property upon publication and may be printed verbatim with credit to MSU. The author of this report is working under contract to MSU and is affiliated with Wayne State University. Reprinting cannot be used to endorse or advertise a commercial product or company. All rights reserved. MSU is an affirmative-action, equal opportunity employer.
To contact Michigan State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.

![]()