
On October 10, 2006, a 40-year-old male career Fire Fighter (the victim) was fatally injured during a residential structure fire. At 0222 hours, dispatch reported a residential two-story row house structure fire with possible parties trapped. Battalion Chief #1 was the first on scene and assumed Incident Command (IC). Squad 11 (SQ11) arrived followed by Engine 41 (E41) as heavy black smoke poured out of the front of the residence. A civilian jumped from an A-side second story window and another confused civilian was walking around on the sidewalk; both were attended to by fire fighters. Two E41 fire fighters (the victim and ff#1) led a Squad -11 fire fighter (ff#2) into the residence with a 1 ¾ attack line. They entered a narrow hallway and passed through a door to the foot of the stairs that lead to the second floor. The E41 Lieutenant entered the structure and requested the building be vented due to the heat. At 0228 hours, Battalion Chief #2 (Rear IC) arrived on scene and reported to the C-side of the structure per the request of the IC. The victim advanced to the top of the stairs when conditions became extremely hot. Shortly after hearing that the fire’s origin may be in the basement causing the crew to back out, the victim feeling the intense heat ran by ff#1 and into ff#2 (from SQ11) knocking them both to the floor with the front door closing behind them and pinching the hose line. FF#2 struggled to get his arm out the crack of the door while ff#1 was trying to get the victim off of ff#2.
Officers and fire fighters were outside trying to pull the fire fighters out and were able to get ff#1 and ff#2 out through a partial opening of the door. The victim could not get out until the door was removed. FF#1 and ff#2 were pulled out at 0232 hours and the victim was removed at 0235 hours. Immediately, paramedics on scene attended to the two fire fighters and the victim. The victim was given cardiopulmonary resuscitation (CPR) and transported to the hospital. FF#1 and ff#2 were transported to the hospital and treated for severe burns.
NIOSH investigators concluded that, to minimize the risk of similar occurrences, fire departments should:
On October 10, 2006, a 40-year-old male career fire fighter (the victim) was fatally injured during a residential structure fire. On October 11, 2006, the fire department notified the National Institute for Occupational Safety and Health (NIOSH) of this fatality. On October 12, 2006, a General Engineer and an Occupational Safety and Health Specialist from the NIOSH Fire Fighter Fatality Investigation and Prevention Program conducted an investigation. Photographs of the incident scene were taken and meetings were conducted with the Safety Chief of the involved fire department, representatives from the City’s Arson Office, and union representatives. The victim’s protective clothing, SCBA, and PASS device were examined. On November 15-16, 2006 interviews were conducted with officers and fire fighters who were at the incident scene. The NIOSH investigators reviewed the department’s standard operating guidelines (SOGs), the Arson Investigator’s report, the officers’ and victim’s training records, photographs of the incident scene, written witness statements, dispatch transcriptions, the coroner’s report and amateur video of the incident.
Fire Department
The career department has thirty-nine stations with a total of 1,611 career fire fighters serving a population of over 651,154 residents in a geographic area of approximately 92 square miles.
Personal Protective Equipment
At the time of the incident, the victim was wearing personal protective equipment consisting of turnout coat and pants, gloves, a helmet, an SCBA with an integrated PASS device, and carried a portable radio. The NIOSH SCBA post-incident test results did not suggest any contributing factor to the incident (see appendix).
Apparatus and Personnel
On scene at 0225 hours:
Training/Experience
The victim was a career fire fighter with 19 years of fire fighting experience. He had completed the National Fire Protection Association (NFPA) Fire Fighter Level I and II training, Field Training, Developing Fireground Expertise, Fire Fighter Survival Training and various other administrative and technical courses.
The Incident Commander had completed the National Incident Management System training, Incident Scene, Construction Awareness, Risk Management, Developing Fireground Expertise, Leadership Skills and various other administrative and technical courses.
The Rear IC had completed the National Incident Management System training, Incident Scene, Building Construction Awareness, Fire Officer Training, Leadership Skills and various other administrative and technical courses.
Building Information
The 1,320 square foot building was a 1920’s two-story residential row house structure without an automatic fire suppression system (see Photos 1 & 2) that was constructed of wood balloon framing with the interior being remodeled to make first and second floor apartments. The basement was accessible from the first floor interior and an exterior alley door. The flat roof consisted of wood rafters with tar and paper over wood boards.
 |
Photo1. Front (A-side) of the structure where the victim entered. |
 |
Photo2. Rear (C-side) of fire structure that was totally involved upon arrival |
On October 10, 2006, a 40-year-old male career fire fighter, (the victim) was fatally injured during a residential structure fire. At 0222 hours, dispatch reported a residential two-story row house structure fire with possible parties trapped. At 0225 hours, Battalion Chief #1 (Incident Commander (IC)) was first to arrive on scene. The IC drove in the front of the structure then drove around the block to look down the alley to the rear (C-side) of the structure during size-up, due to this being a rowhouse in the middle of the block, and returned to the front (A-side). Squad 11 (SQ11) then arrived, followed by Engine 41 (E41) as heavy black smoke poured out of the front of the residence. A civilian jumped from an A-side second story window and another confused civilian was walking around on the sidewalk. Both were promptly attended to by fire fighters. E41 covered SQ11 on the hydrant per standard operating guidelines. However, SQ11 did not stretch the first attack line; instead, two E41 fire fighters (the victim and ff#1) led a Squad 11 fire fighter (ff#2) into the residence with a 1 ¾ attack line from SQ11’s pumper. Other members of SQ11 were putting on their gear and grabbing a second back up line. They entered a narrow hallway and went through an open door at the bottom of the stairs that led to the second floor. The E41 Lieutenant entered the structure and requested the building be vented due to the heat. At 0228 hours, Battalion Chief #2 (Rear IC) arrived on scene and reported to the C-side, where Truck 3 (T3) was trying to position ladders while Engines 5 and 51 were stretching line from opposite ends of the rear alley. The basement was heavily involved and fire was starting to blow out the first and second floors in the rear. Operations were being hindered by numerous electric lines in the rear of the fire structure. At 0231 hours, the IC called for a second alarm and for the utility company to cut the power. Truck 20 (T20) positioned their aerial ladder to the roof so a fire fighter could vent the roof while other crew members positioned a ground ladder to the front second floor window to vent. FF#1 and ff#2 manned the hoseline at the base of the stairs while the victim advanced to the top of the stairs (see Diagram #1). No fire was seen by any member of the interior attack crew at this time and there appeared to be no fire impingement from the interior towards the front of the structure. The T20 fire fighter on the roof opened up several sky lights, but the back skylight had self vented, so the fire fighter went back to the A-side of the first sky light to open up a hole in the roof, but fire started blowing out and he couldn’t finish. At 0231 hours, the interior crew learned that the fire’s origin may be in the basement and to start backing out. At 0232 hours, conditions became extremely hot inside the fire structure and the victim suddenly ran by ff#1 and into ff#2 (from Squad 11). FF#2 fell to the floor with the victim on top of him. They came to rest against the metal front door, forcing it to close off the front entrance. This pinched the hose line in the door frame, leaving a small gap between the metal door and the door frame (see Diagram #2). In addition to being pinched, the hose possibly got bundled up behind the door along with the victim’s body, adding to the difficulty of getting the door open. FF#2 was pinned to the floor and managed to get his arm through the small gap at the door while ff#1 tried to get the victim off of ff#2. At this point, the IC requested a rapid intervention crew (RIC) which had not been established.
The E41 Lieutenant and several other fire fighters, who had exited the fire structure just prior to the door closing, were outside trying to pull the fire fighters out of the structure and began to force open and remove the door. At 0232 hours, ff#1 and ff#2 were pulled out of the partially forced opened door and were attended to by the Paramedics. At 0235 hours, the door was removed, and the victim could be seen on the floor with his mask off and hood missing. Fire fighters carried the victim to the Paramedics, who administered cardiopulmonary resuscitation (CPR) and transported to the hospital where he was pronounced dead. FF#1 and ff#2 were transported to the hospital and treated for severe burns.
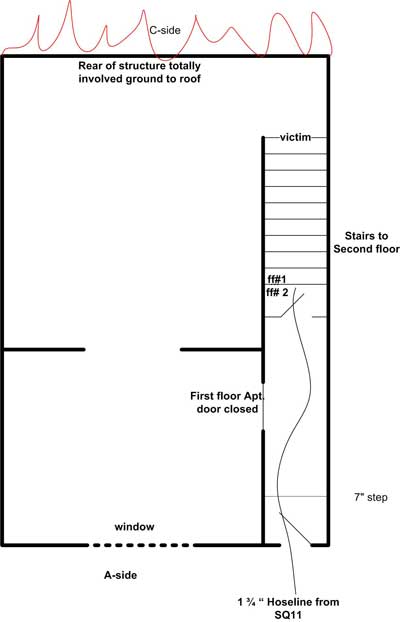 |
Diagram 1. Location of victim and fire fighters on the hoseline prior to incident. |
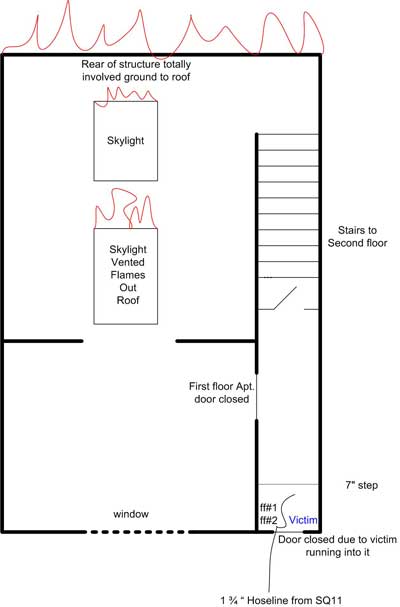 |
Diagram 2. Location of victim and injured fire fighters trapped behind door.
|
Both fire fighters #1 and #2 received burns on both hands, wrists, and forearms with more severe (3rd degree) burns on the left side (approximately covering 3% of their body).
The coroner listed cause of death from smoke inhalation and thermal injuries. Soot was present in the airways. His heart blood carboxyhemoglobin saturation was 26%. Thermal injuries were present over approximately 30% of the body. Affected areas were the head, chest, hands, forearms and lower back.
Discussion: The use of a TIC can provide the IC with additional information during the initial size-up and for locating the seating of the fire. They can be used to quickly gather crucial information on the fire’s location from the exterior of the structure, assisting with determining a rapid and safe approach to entering the structure. Also, firefighters about to enter an area filled with flames and smoke can use the TIC to assist in determining the risks in advancing. TICs can also be useful for identifying structures that have been dangerously weakened by the fire. Thermal imaging cameras (TICs) should be used in a timely manner, and fire fighters should properly be trained in their use and be aware of their limitations.1
Discussion: Ventilation is performed to relieve the products of combustion, allowing fire fighters to advance on the fire. When venting, the principle is to pull the fire, heat, smoke, and toxic gases away from victims, stairs, and other egress routes. 2
In this incident, shortly after the skylights had been vented the fire immediately intensified forcing the victim to run down the stairs trying to escape. The victim was near the top of the stairs, in front of his crew and without a hoseline, and the rear of the structure was fully involved at the time the skylights were vented. The smoked filled second floor provided the needed oxygen when the skylight was vented, thus igniting the unburned fuel and pulling the flames towards the interior of the second floor over the victim near the top of the stairs.
Discussion: Wedges (generally wood or rubber) are commonly carried by fire fighters for a temporary shut-off of activated sprinkler heads or for holding doors open during firefighting or rescue operations. Doors are wedged open to prevent pinched or snagged hoses, which could cut-off a fire fighters protective stream, and to ease ingress/egress of fire fighters.
In this incident, a wedge may have kept the door open and kept the hose from getting pinched and bundled up behind the door which further hindered getting the door open.
Discussion: A rapid intervention crew (RIC) should be available for the rescue of members operating at emergency incidents. The team should report to the officer in command and remain at the command post until an intervention is required to rescue a fire fighter(s) or civilians. The RIC should have all tools necessary to complete the job (e.g., a search rope, first-aid kit, and a resuscitator) to use if a fire fighter becomes injured. Many fire fighters who die from smoke inhalation, from a flashover, or from being caught or trapped by fire actually become disoriented first. They are lost in smoke and their SCBAs run out of air, or they cannot find their way out through the smoke, become trapped, and then fire or smoke kills them. The primary contributing factor, however, is disorientation. The RIC’s only assignment should be to prepare for a rapid deployment to complete any emergency search or rescue when ordered by the IC. They will provide the suppression companies the opportunity to regroup and take a roll call instead of performing rescue operations. A RIC should preplan a rescue operation by finding out fire structure information (i.e., construction materials, layout, entry/egress routes, etc.), crew location and assignments, and monitor radio traffic. When the RIC enters to perform a search and rescue, they should have full cylinders on their SCBAs and be physically prepared. When a RIC is used in an emergency situation, an additional RIC should be put into place in case an additional emergency situation arises. 3 This additional RIC should be comprised of fresh, well-rested fire fighters.
In this incident, when the IC requested a RIC, one had not been established. Numerous fire fighters were at the door and promptly extricated two fire fighters and retrieved the victim after removing the door.
Operational protocols, minimum equipment, personnel requirements, qualifications for team membership, and issues of training, drills, health and safety are all addressed in the fire department’s standard operating procedures (SOPs). However, SOPs should be reviewed in-house, at a minimum, on an annual basis to see whether any changes are necessary. Every department member should have a copy of or easy access to SOPs, and each member should sign a statement indicating that he/she has read, understands, and agrees to abide by them.
In this incident, there were some SOPs that may have been deviated from unintentionally or circumstances didn’t allow. For example, the information to “back-out” was received by the interior crew fire fighters but it was unclear who gave the order. The fireground operations SOP describing the duties of the first and second arriving engine was not followed, in that, the second engine initiated the search and rescue operation instead of the first engine. 4 In addition, there where issues regarding protective equipment, such as, missing hood, cylinder valve shut-off, and right hand glove removed. Witnesses state that the victim entered the structure with his mask on and the second stage regulator clicked in and gloves on. No one verified seeing the victim with his hood on. During the incident his cylinder valve was shut-off, his right hand glove was missing, his mask was dislodged, and his hood was missing, either initially or not recovered assuming the victim removed it in the fire structure.
This incident was investigated by Matt Bowyer, General Engineer and Steve Berardinelli, Occupational Safety and Health Specialist, with the Fire Fighter Fatality Investigation and Prevention Program, Division of Safety Research at NIOSH. An expert technical review was provided by Harry Carter, Ph.D., CFO, MIFireE.
Summary of Status Investigation Report
NIOSH Task No. 14886
Background
As part of the National Institute for Occupational Safety and Health (NIOSH) Fire Fighter Fatality Investigation and Prevention Program, the Technology Evaluation Branch agreed to examine and evaluate one Dräger Safety 4500 psi, 45-minute, self-contained breathing apparatus (SCBA).
This SCBA status investigation was assigned NIOSH task number 14886. The submitter was advised that NIOSH would provide a written report of the inspections and any applicable test results.
The SCBA, sealed in a corrugated cardboard box, was delivered to the NIOSH facility in Bruceton, Pennsylvania on October 30, 2006. The sealed package was taken to the Firefighter SCBA Evaluation Lab (building 108) and stored under lock until the time of the evaluation.
SCBA Inspection
The package was opened and the SCBA inspection was initiated on March 6, 2007. A complete visual inspection of the SCBA was completed on that day by Vance Kochenderfer, Quality Assurance Specialist, of the Technology Evaluation Branch, National Personal Protective Technology Laboratory (NPPTL), NIOSH. The SCBA was examined, component by component, in the condition as received to determine its conformance to the NIOSH-approved configuration. The visual inspection process was videotaped. The SCBA was identified as the Dräger AirBoss Evolution model.
Although the SCBA showed signs of extensive use and wear, it was determined that it could be safely pressurized and tested. The interior of the demand valve outlet was very dirty, suggesting the demand valve was detached from the facepiece in a smoky environment. There are a few signs of heat damage on the cylinder retention band, shoulder straps, and cylinder valve. The cylinder bears some scrapes which may render it unfit for use; it should be examined by a qualified retester before being returned to service. The damage to the cylinder valve is such that it should be repaired or replaced.
SCBA Compressed Air Cylinder Contents
During the inspection it was noted that the compressed air cylinder was partially pressurized. An air sample was collected from the cylinder and forwarded to a laboratory for analysis. The laboratory, Lab Services-ITR, analyzed the sample in accordance with the standards and methodologies found in the Compressed Gas Association’s standard, ANSI/CGA G-7.1, Commodity Specification for Air. The analysis is attached as Appendix II.
The test report indicates that the sample met the standard for Grade D air. The sample also met OSHA’s moisture content requirement in 29 CFR 1910.134(i)(4)(iii) as well as the more stringent moisture content guidelines published in NFPA 1500, Standard on Fire Department Occupational Safety and Health Program, 2002 Edition.
SCBA Testing
The purpose of the testing was to determine the SCBA’s conformance to the approval performance requirements of Title 42, Code of Federal Regulations, Part 84 (42 CFR 84). Further testing was conducted to provide an indication of the SCBA’s conformance to the National Fire Protection Association (NFPA) Air Flow Performance requirements of NFPA 1981, Standard on Open-Circuit Self-Contained Breathing Apparatus for the Fire Service, 1997 Edition.
The following performance tests were conducted on the SCBA:
NIOSH SCBA Certification Tests (in accordance with the requirements of 42 CFR 84):
National Fire Protection Association (NFPA) Tests (in accordance with NFPA 1981, 1997 Edition):
The NIOSH tests were performed on March 7, 2007. Although the SCBA was not labeled as compliant with NFPA 1981, it was requested that the NFPA Air Flow Performance Test be performed and this was conducted on March 23, 2007. All testing was videotaped with the exception of the Exhalation Resistance Tests and Static Pressure Tests.
The SCBA ran out of air before its rated service time, causing the unit to fail the Rated Service Time Test and Positive Pressure Test. It also had excessive exhalation resistance during the NFPA Air Flow Performance Test. A rattling noise was observed coming from the facepiece exhalation valve; it is possible that improper function of this valve could cause the failing test results. The unit met the requirements of all other tests. While the unit was capable of supplying air to the user, it was unable to provide the designed level of protection.
Summary and Conclusions
The SCBA submitted for evaluation was delivered to NIOSH on October 30, 2006 and inspected on March 6, 2007. The unit was identified as a Dräger AirBoss Evolution 45-minute, 4500 psi SCBA (NIOSH approval number TC‑13F‑379). The unit was determined to be in a condition safe for testing.
The unit was subjected to a series of seven performance tests. Testing was performed on March 7 and 23, 2007. The SCBA was able to meet the requirements of all tests except the Rated Service Time Test, Positive Pressure Test, and NFPA Air Flow Performance Test. No maintenance or repair work was performed on the unit at any time.
In light of the information obtained during this investigation, NIOSH has proposed no further action on its part regarding the SCBA at this time. Following inspection and testing, the SCBA was returned to the package in which it was received and was shipped back to the submitter on April 5, 2007.
If the SCBA is to be placed back in service, it must be thoroughly inspected, repaired, and tested by a qualified service technician. The cylinder should be inspected by a certified retester before being put back into use, and the cylinder valve repaired or replaced.

Return to Fire Fighter Homepage
![]()
This page was last updated on 12/10/07.