
On May 14, 2006, a 61-year-old male career Lieutenant (the victim) was fatally injured at a residential structure fire as a result of smoke inhalation. Dispatch had reported a residential two-story structure fire with possible trapped victims. The victim’s engine (E9) was first on the scene followed shortly by a ladder truck, where they encountered heavy smoke pouring out of the back of the residence. The victim and two fire fighters from E9 entered the structure in a fast attack mode while fire fighters from the other apparatus rescued a civilian. The victim and fire fighters donned their self-contained breathing apparatus (SCBA) once inside the smoky kitchen. Then the victim and fire fighters advanced the attack line through the first floor of the house and up the stairs where they encountered high heat and zero visibility. After further advancing into what the victim and fire fighters thought was a hallway (it was actually a small bedroom), they concluded that they were not in the fire room. They felt heat and believed they had fire in the attic above them, so they backed out to regroup at the top of the stairs. The two fire fighters assumed the victim was nearby. Both fire fighters ended up exiting the structure, within minutes of each other, when their low air alarms went off. Other fire fighters heard a personnel alert safety system (PASS) alarm when they were on a landing just below the top of the stairs. The Rapid Intervention Team (RIT) was activated but the fire fighters who had reported the PASS alarm also took the initiative to find the victim. They located the victim underneath a mattress and pulled him to the doorway near the top of the stairs. The RIT progressed to the top of the stairs and extricated the victim to the yard where cardiopulmonary resuscitation (CPR) was performed. The hospitalized victim succumbed to his injuries on May 21, 2006.
NIOSH investigators concluded that, to minimize the risk of similar occurrences, fire departments should:
Although there is no evidence that the following recommendations could have specifically prevented this fatality, NIOSH investigators recommend that fire departments:
On May 14, 2006, a 61-year-old male career Lieutenant (the victim) was fatally injured at a residential two-story structure fire. On May 21, 2006, the U.S. Fire Administration (USFA) and the International Association of Fire Fighters (IAFF) notified the National Institute for Occupational Safety and Health (NIOSH) of this fatality. On July 17 - 19, 2006, a General Engineer and two Safety and Occupational Health Specialists from the NIOSH Fire Fighter Fatality Investigation and Prevention Program investigated the incident. Photographs of the incident scene were taken and meetings were conducted with the Fire Chief, three representatives from the City’s Arson Office, and an IAFF representative. Interviews were conducted with officers and fire fighters who were at the incident scene. The NIOSH investigators reviewed the department’s standard operating guidelines (SOGs) and internal investigation report, the arson investigator’s report, the officers’ and victim’s training records, photographs of the incident scene, written witness statements, dispatch transcriptions and the coroner’s report. The victim’s protective clothing, SCBA, and PASS device were examined. At the request of the fire department, NIOSH tested the SCBA against certification requirements and conducted a breathing air analysis. The unit passed all testable requirements (see Appendix).
Fire Department
The career department has thirty three stations with a total of 917 career fire fighters serving a population of about 580,550 residents in a geographic area of approximately 154 square miles.
Personal Protective Equipment
At the time of the incident, the victim was wearing personal protective equipment consisting of turnout coat and pants, gloves, a helmet, hood, an SCBA with an integrated PASS device, and carried a radio. The NIOSH SCBA post incident test results did not suggest any contributing factors to the incident (see Appendix).
Apparatus and Personnel
On scene at 0445 hours:
Engine #9 [E9] – Lieutenant (the victim), engine operator, and two fire fighters (ff#1 and ff#2)
Truck #9 [T9] – Lieutenant (initial IC), engine operator, and two fire fighters
Squirt #10 [Q10] – Lieutenant, engine operator, and two fire fighters
On scene at 0447 hours:
Chief #1 (Incident Commander)
Engine #3 [E3] – Captain, engine operator, and two fire fighters
On scene at 0448 hours:
Truck #8 [T8] – Lieutenant, engine operator, and two fire fighters (ff#3 and ff#4)
On scene at 0449 hours:
Chief #2 (Interior Commander)
On scene at 0452 hours:
Rescue #1 [R1] – Lieutenant, engine operator and two technicians
Training/Experience
The victim had completed the National Fire Protection Association (NFPA) Fire Fighter Level I and II training, Field Officer Training, Developing Fireground Expertise, Fire Fighter Survival Training and various other administrative and technical courses. The victim was a career fire fighter with more than 30 years of fire fighting experience.
The Incident Commander had completed the National Incident Management System training, Incident Scene, Construction Awareness, Risk Management, Developing Fireground Expertise, Fire Fighter Survival Training, Leadership Skills and various other administrative and technical courses.
The Interior Command Chief had completed the National Incident Management System training, Incident Scene, Construction Awareness, Risk Management, Developing Fireground Expertise, Fire Fighter Survival Training, Field Officer Training, Leadership Skills and various other administrative and technical courses.
Building Information
The building was a two-story, non-sprinklered residential structure that was constructed of wood framing with an exterior stucco finish. The roof consisted of wood rafters with asphalt shingles over wood boards (see Photo1). Also, this photo shows the D-side door the victim entered. The window above is in the room the victim was found and the burnt away roof was over the bedroom where the fire originated.
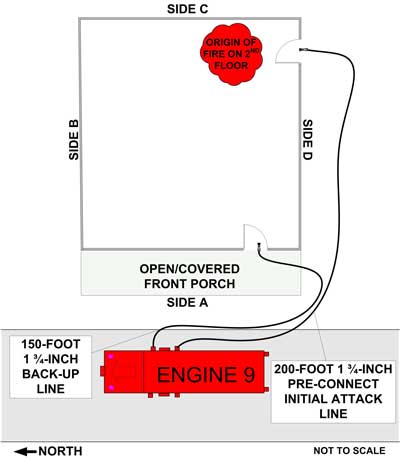
On May 14, 2006, at 0440 hours, six apparatus (E9, T9, Q10, T8, E3, and R1) were dispatched from four stations of the same department to a residential two-story structure fire with possible trapped civilians on the second floor. At 0445 hours, E9 arrived laying out 200 feet of 1 ¾ inch pre-connect attack line to a door on the D-side of the structure (see Diagram #1). E9 reported fire in the back of the residence (C-side). Q10 and T9 arrived at 0445 hours with T9 assuming initial incident command (IC).
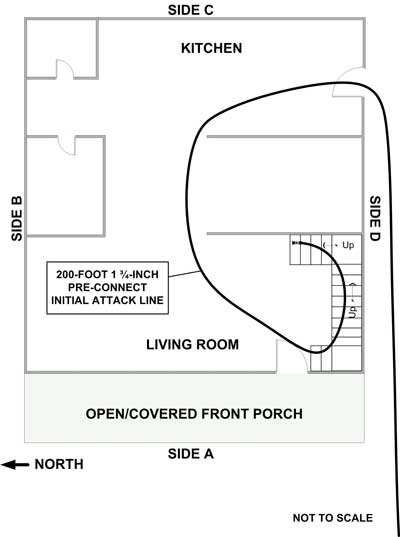
E9 was in fast attack mode and entered the structure into the kitchen. The E9 crew encountered moderate smoke conditions in the kitchen, donned their masks, and advanced the hose line through the cluttered rooms and up the stairs to the second floor. T9 fire fighters spoke with a confused resident of the house and confirmed that at least one female was trapped upstairs. At 0445 hours, Chief #1 called for all personnel to switch to fireground channel 4. Note: Some crew members were unable to switch radio channels due to bulky gloves and visibility.
At 0445 hours and 32 seconds, two T9 fire fighters found an unconscious female in a bedroom at the top of the stairs to the left, and extricated her to the front yard where CPR was performed and an ambulance called. At 0446 hours, Q10 pulled a 2 ½ inch back up line from E9 to help look for other trapped occupants.
At 0447 hours, Chief #1 arrived on the scene and assumed incident command (IC) for the duration of the incident. E3 also arrived and was assigned as the RIT. At 0448 hours, T8 arrived on the scene and was assigned to the A-Side for search and rescue. At 0449 hours, Chief #2 arrived and was instructed by Chief #1 to suit up for interior command. Upon completion of a 360 walk around, Chief #2 reported heavy fire in the back and fire venting out of the second story window on the C-side.
At 0450 hours, the T9 crew disconnected electrical services to the structure. At 0451 hours, Chief #1 asked E9 if they had made it to the second floor. The victim responded affirmatively. At this point, the attack line was advanced to the top of the stairs to the right with the victim out in front of ff#1 on the nozzle and ff#2 backing him up (see Diagram #2). There was zero visibility with extreme heat. The hallway to the origin of the fire was blocked with a large box leaving only a 17 inch gap. The crew advanced to their right through a 27 inch doorway thinking they were heading towards the fire’s origin. The crew had entered a small 9 foot by 10 foot bedroom, just prior to the fire’s origin, packed with boxes, clothes and furniture. The victim reportedly was doing a left hand search while ff#1 and ff#2 were doing a right hand search with the nozzle. Thus, the victim was operating alone. A short time later the crew ran into each other. FF#2, who was behind ff#1, heard some discussion between ff#1 and the victim about there being no room to advance and not being able to locate the fire. The IC informed the E9 crew that all of the fire was on the C-side of the building and directed them to get some water on it. FF#2 pulled the ceiling using a pike pole to see if fire was above them. FF#2 told ff#1 to open the nozzle above them. Feeling extreme heat and realizing that they were not in the fire room, ff#1 and ff#2 backed out and regrouped at the top of the stairs. At this point, the victim’s location was not exactly known but ff#1 and ff#2 assumed he was nearby.
At 0452 hours, R1 arrived on the scene and was instructed to vent and ladder the D-side of the building as T9 shut off the gas. T8 fire fighters (ff#3 and ff#4) started up the stairs and passed ff#2 going down the stairs. When they reached the top of the stairs they encountered heavy smoke and heat and ff#1. They advanced further but encountered a partially blocked door, so they moved to the left and encountered more heat and obstructions. FF#1’s low air alarm was going off as he squeezed by ff#3 and ff#4 to go down the stairs. Due to worsening conditions and unable to advance the search, ff#3 and ff#4 retreated down the stairs to the landing.
At 0455 hours, the IC instructed R1 to perform a secondary search on the second floor once the fire was able to be knocked down. At 15 minutes into the incident, Q10 took a second line up the stairs and met the T8 fire fighters on the stair landing. At this time the crews heard a PASS device and reported it to command. The IC asked for confirmation. Q10 confirmed hearing a PASS in the house. At 0456 hours, T8 confirmed hearing a PASS and requested activation of the RIT.
Command instructed interior crews to start backing out and to do a personnel accountability report (PAR) on E9. Q10 arrived at the top of the stairs with high heat and heard a PASS alarm on the second floor. At 0458 hours, the IC sent in the RIT (E3). Q10 reported high heat on the second floor and requested venting. Command confirmed that the windows were vented. FF#3 and ff#4 were in front of the Q10 crew and followed the sound of the PASS device. FF#3 pushed his way through the door and noticed that the floor felt spongy and realized he was on top of a mattress. After moving the mattress the sound of the PASS got louder. FF#3 felt the victim’s air cylinder and directed ff#4 to grab the harness strap. At 0459 hours, a T8 fire fighter radioed, “ back out! back out!, got the victim” (see Diagram #3). FF#3 and ff#4 dragged the victim to the door. The Q10 crew and RIT grabbed the victim, ff#3 and ff#4 and extricated them down the stairs and out into the front yard.
A Q10 fire fighter tried removing the victim’s mask, which reportedly was still properly positioned on the victim’s face, but the airline was getting caught on something. Then the Q10 fire fighter shut off the air and unclipped the victim’s regulator. The facepiece and hood were removed. Realizing that the victim was not breathing, CPR was performed and the victim was transported to the local hospital. The victim spent a week in a drug induced coma, was taken off the ventilator, and died as a result of his injuries on May 21, 2006.
Note: In this incident, the victim had a 23 percent CO level in his blood at the hospital. Witnesses stated that the victim donned his mask once in the structure. When he responded to the IC that he was on the second floor, the dispatch tapes indicated that he had his mask on and was coherent. At sometime during the incident, while the victim was in the small bedroom, apparently the victim’s mask became temporarily dislodged for an unknown reason, accounting for the high concentration of CO in his blood. The victim was found with a mattress on top of him and minimal equipment damage due to heat. Also, the victim’s 4500 psi air tank contained 2000 psi when evaluated after the incident.
The coroner listed the cause of death as complications from hypoxic encephalopathy (lack of oxygen to the brain) due to apparent smoke inhalation.
Discussion: Each fire fighter should be assigned to a team of two or more and given specific assignments to help reduce the chance of injuries. Team continuity relies on knowing who is on your team, knowing the team leader, staying within visual contact at all times (if visibility is obscured then teams should remain within touch or voice distance of each other), communicating your needs and observations to the team leader, rotation to rehabilitation and staging as a team, and watching your team members (practice a strong "buddy system or team" approach). These key factors help to reduce the risks involved in fire fighting operations by providing personnel with the added safety net of fellow team members. 1, 2 In this incident, the three-member E9 crew were separated from one another at different times during the operation.
Since carbon monoxide (CO) is given off in varying quantities during all fires, and other toxic materials are typically present, it is paramount that officers and fire fighters follow the department’s guidelines for the wearing of masks at structure fires. In this incident, the fast attack team reported that they donned their masks inside the structure while encountering moderate smoke conditions. Thus, an unknown level of CO was present in that smoke and inhaled by the fire fighters. Fire fighters whom are frequently exposed to CO may develop a tolerance to it, and function without symptoms, but experience the effects later. Since CO is a narcotic or asphyxiant gas that affects the central nervous system, reduced awareness and clouded judgment may result. 3
Far more fire deaths occur from carbon monoxide than from any other toxic product of combustion. The poorer the ventilation and the more inefficient the burning, the greater the quantity of carbon monoxide formed. Headaches, dizziness, nausea, vomiting, and cherry-red skin can occur at many concentrations, based on an individual’s dose and exposure (see Table 1). 3 These signs and symptoms are not good indicators of safety.
Carbon Monoxide (CO)(ppm) |
Carbon Monoxide in air (percent) |
Symptoms |
100 |
0.01 |
No symptoms-no damage |
200 |
0.02 |
Mild headache; few other symptoms |
400 |
0.04 |
Headache after 1 to 2 hours |
800 |
0.08 |
Headaches after 45 minutes; nausea, collapse, and unconsciousness after 2 hours. |
1,000 |
0.1 |
Dangerous; unconscious after 1 hour |
1,600 |
0.16 |
Headache, dizziness, nausea after 20 minutes. |
3,200 |
0.32 |
Headache, dizziness, nausea after 5 to 10 minutes; unconsciousness after 30 minutes. |
6,400 |
0.64 |
Headache, dizziness, nausea after 1 to 2 minutes; unconsciousness after 10 to 15 minutes. |
12,800 |
1.26 |
Immediate unconsciousness, danger of death in 1 to 3 minutes. |
Table 1. Toxic Effects of Carbon Monoxide. |
||
Because the newly formed carboxyhemoglobin may be traveling through the body, a person previously exposed to a high level of carbon monoxide may react later. If fire fighters develop any of these signs, they, as a team, should immediately exit the structure and receive the proper medical care. Severe exposures to carbon monoxide can cause nerve injury or brain damage. If fire fighters are overcome with carbon monoxide, they should not be allowed to re-enter a contaminated atmosphere. If fire fighters suspect they have been exposed to carbon monoxide, they should notify their officer or the IC and report to EMS for immediate evaluation. In this incident, several fire fighters stated they experienced nausea, dizziness, and disorientation; however, some of these fire fighters had re-entered the structure to search for the victim.
Although there is no evidence that the following recommendations could have specifically prevented this fatality, NIOSH investigators recommend that:
Discussion: The fireground communications process combines electronic communication equipment, a set of standard operating procedures, and the fire personnel who will use the equipment. To be effective, the communications network must integrate the equipment and procedures with the dynamic situation at the incident site, especially in terms of the human factors affecting its use. The ease of use and operation may well determine how consistently fire fighters monitor and report conditions and activities over the radio while fighting fires. Fire departments should review both operating procedures and human factors issues to determine the ease of use of radio equipment on the fireground to ensure that fire fighters consistently monitor radio transmissions from the IC and respond to radio calls. 4 Thus, the need to drill/practice operating radios with gloves on so they don’t have to be removed during fire operations is critical. In this incident, a team member of E9 indicated that when the IC changed the fireground channel he was unable to set his radio on the proper channel. He indicated that this is a common occurrence due to not hearing the command or not being able to properly select the channel with bulky gloves on and poor visibility.
Discussion: A proper size-up begins from the moment the alarm is received, and it continues until the fire is under control. Several factors must be evaluated in conducting the size-up, for example, the type of structure and its construction, occupants, time of day, contents of the structure, and potential hazards. 5 During the size-up, fire fighters should attempt to determine the approximate location and intensity of the fire and how best to reach the seat of the fire. In this case, a resident of the house was in the yard and did not convey that the stairs were in the front of house. The resident also indicated that perhaps more than one occupant was in the house. In addition to the rescued female, a pet was later recovered. The victim saw that there was smoke coming from the second floor C-side of the house and entered the structure on D-side closest to the C/D corner which required running the 200 feet of 1 ¾ attack line through the house to the A–side and up the stairs. This required additional time and energy when there was an entrance on the A-side nearest the stairs and closer to the engine.
This incident was investigated by Matt Bowyer, General Engineer, Mark McFall, Safety and Occupational Health Specialist, and Jay Tarley, Safety and Occupational Health Specialist, with the Fire Fighter Fatality Investigation and Prevention Program, Division of Safety Research at NIOSH. A technical review of this report was provided by Chief William Goldfeder, Loveland-Symmes Fire Department and editor of http://www.FirefighterCloseCalls.com
NIOSH Reference: TN-14618
The National Institute for Occupational Safety and Health (NIOSH) has concluded its investigation conducted under NIOSH Task Number 14618. This investigation consisted of the inspection and testing of one Scott 4500 psi, 30-minute, self-contained breathing apparatus (SCBA). The SCBA, sealed in a corrugated cardboard box, was delivered to the NIOSH facility in Bruceton, Pennsylvania on May 25, 2006. The sealed package was taken to the Firefighter SCBA Evaluation Lab in building 108 and stored under lock until the time of the evaluation.
SCBA Inspection
The SCBA inspection was performed on July 25, 2006. The SCBA was examined, component by component, in the condition as received to determine its conformance to the NIOSH-approved configuration. The entire inspection process was videotaped. The SCBA was identified as the Scott Air-Pak Fifty 4.5 model.
Overall the SCBA is in very good condition. Many components of the unit are covered in a fine sandy material, and there is some damage to the fabric components of the shoulder straps. The gasket which seals the regulator to the facepiece is also slightly damaged. Otherwise, the SCBA appears to be in good working order.
Personal Alert Safety System (PASS) Device
A Personal Alert Safety System (PASS) device was incorporated into the pneumatics of the SCBA. During the inspection, the PASS device was activated both manually and automatically. Although the unit appeared to function normally, it was not tested against the specific performance requirements of NFPA 1982, Standard on Personal Alert Safety Systems (PASS), 1998 Edition. Because NIOSH does not certify PASS devices, no further testing or evaluations were conducted on the PASS unit.
SCBA Compressed Air Cylinder Contents
During the inspection it was noted that the compressed air cylinder was partially pressurized. An air sample was collected from the cylinder and forwarded to an accredited laboratory for analysis. The laboratory, Dräger Lab Services, analyzed the sample in accordance with the standards and methodologies found in the Compressed Gas Association’s standard, ANSI/CGA G-7.1, Commodity Specification for Air.
The test report indicates that the sample met the standard for Grade D air. The sample also met OSHA’s moisture content requirement in 29 CFR 1910.134(i)(4)(iii) as well as the more stringent moisture content guidelines published in NFPA 1500, Standard on Fire Department Occupational Safety and Health Program, 2002 Edition.
SCBA Testing
The purpose of the testing was to determine the SCBA’s conformance to the approval performance requirements of Title 42, Code of Federal Regulations, Part 84 (42 CFR 84). Further testing was conducted to provide an indication of the SCBA’s conformance to the National Fire Protection Association (NFPA) Air Flow Performance requirements of NFPA 1981, Standard on Open-Circuit Self-Contained Breathing Apparatus for the Fire Service, 1997 Edition.
NIOSH SCBA Certification Tests (in accordance with the performance requirements of 42 CFR 84):
National Fire Protection Association (NFPA) Tests (in accordance with NFPA 1981, 1997 Edition):
Testing was conducted on July 26, 2006. All testing was videotaped with the exception of the Exhalation Resistance Test and Static Pressure Test. The SCBA met the requirements of all tests.
Summary and Conclusions
The SCBA was delivered to NIOSH on May 25, 2006 and underwent inspection on July 25, 2006. The unit was identified as a Scott Air-Pak 4.5 30-minute, 4500 psi, SCBA (NIOSH approval number TC‑13F‑76). The SCBA was determined to be in a condition safe for testing.
The unit was subjected to a series of seven performance tests on July 26, 2006. The SCBA met the requirements of all tests.
Following inspection and testing, the SCBA was returned to the package in which it was received and stored under lock in building 108 at the NIOSH facility in Bruceton, Pennsylvania pending return to the Fire Department.
If the SCBA is to be placed back in service, it should be cleaned to remove the sand from it, the damaged shoulder straps repaired or replaced, and the damaged regulator gasket replaced. It should be inspected and tested by a qualified service technician before being returned to use.
In light of the information obtained during this investigation, the Institute has proposed no further action at this time. The investigation under task number 14618 will be considered closed. If you have any questions or require additional information, please contact me at 412‑386‑4029.
Sincerely yours,
Vance Kochenderfer
Quality Assurance Specialist
Respirator Branch
National Personal Protective Technology Laboratory
 |
 |
 |
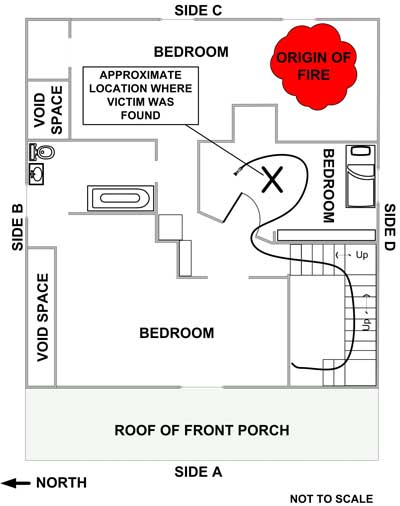 |
Diagram 3. Aerial View of Second Floor |

Return to Fire Fighter Homepage
![]()
This page was last updated on 06/27/07.