
On April 30, 2004, a 58-year-old male career fire fighter (the victim) sustained a fatal head injury when he fell from a moving, cab-forward engine. The engine was responding to a reported gas odor with a fire fighter/driver and an officer in the cab, and two firefighters, including the victim, seated in the open jump seats. Upon departure from the station, the engine made a right turn from the apron onto the street. During this turn, the victim fell out of the driver side jump seat door landing on the street and striking his head. He was treated at the scene for head trauma and transported to a local hospital. He died from his injuries three days after the incident.
NIOSH investigators concluded that, to minimize the risk of similar occurrences, fire departments should:
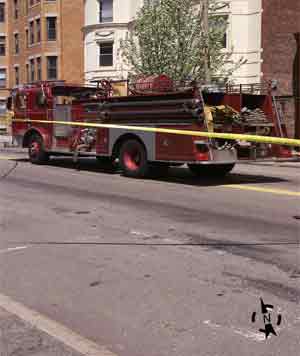 |
Incident scene |
On April 30, 2004, a 58-year-old male career fire fighter (the victim) fell from a moving cab-forward engine and subsequently died from his injuries on May 3, 2004. On May 4, 2004, the U.S. Fire Administration (USFA) notified the National Institute for Occupational Safety and Health (NIOSH) of this fatality. On June 23, 2004, a safety and occupational health specialist from the NIOSH Fire Fighter Fatality Investigation and Prevention Program investigated the incident. The NIOSH investigator met with the chief of the department, the department administrative and medical officer, the maintenance supervisor, the training and safety officer, and crew members who were on the responding apparatus. The police report, training records of the victim, standard operating procedures (SOPs), department training records and procedures, dispatch sheets, apparatus maintenance records, and the death certificate were reviewed. The NIOSH investigator also spoke with, and reviewed evidence collected by, police officers who investigated the incident.
Department The career department has 152 fire fighters and serves an area of about 7 square miles. The department has five fire stations that serve a population of approximately 57,000. The 58-year-old victim had more than 36 years of service as a career fire fighter, and had been with this department his entire career.
The department has a maintenance division that is staffed by two full-time, certified mechanics who service the fire department vehicles, emergency apparatus, and the self-contained breathing apparatus (SCBA).
Training The State where the incident took place has no minimum training requirements for fire fighters. The department requires all new recruits to complete Operation Level for Hazardous Materials training, and to be trained in accordance with the requirements of Fire Fighter Level I, as described in the International Fire Service Training Association Manual, “Essentials of Firefighting” fourth edition.1
In addition to the required courses, the victim had successfully completed numerous training courses including Pre-fire Planning, Incident Command, Driver Training, Rapid Intervention, Structural Hazards, and Interior Fire Attack.
Equipment The victim was riding in a 1976 cab-forward engine that was being used as a reserve unit while the assigned engine was in the shop for maintenance. The fire department purchased the engine new in 1976 and had safety bars installed in the open jump seat area. In 2001, the safety bars were replaced with half-style doors that were equipped with a slam-lock system. The door locking system included an inside vertical and thumb-rotary locking/unlocking feature. The seatbelt was a lap-only type. A self-contained breathing apparatus (SCBA) walk-away wall bracketa was installed behind the victim’s seat (Photo 1).
Fire department apparatus are required to pass an annual State inspection. The inspection protocol includes requirements for a visual inspection of all safety belts, lap belts and shoulder restraints to assure good working order.2 It is standard department procedure to perform weekly and monthly apparatus/equipment maintenance reports, in addition to daily maintenance checks.
Weather / Road Conditions The incident occurred on a city street that runs directly in front of the fire station (Photo 2). The road surface is made of asphalt and is well traveled. There were no defects to the road surface that would hinder the performance of the roadway or interfere with the operation of the engine.
At the time the incident occurred, 0909 hours, there was no precipitation and the pavement was dry. The sky was clear with a temperature of around 64º F. The wind was blowing from the southwest at approximately ten miles per hour (mph).
On April 30, 2004, at 0905 hours, a career fire department was dispatched to a residential structure where there was a reported gas odor. The assigned engine was out of service for maintenance so the crew responded in a cab-forward engine that was used as a reserve apparatus. The engine was manned by a fire fighter/driver and lieutenant in the enclosed front cab and two fire fighters, including the victim, in the open jump seats.
Due to the nature of the call, the victim stopped to retrieve a gas detectorb from the charging station located adjacent to the apparatus bay and was last to board the engine. The lieutenant who was in the officer’s seat gave the go-ahead signal to the driver after determining that both fire fighters in the open jump seat area had boarded and were seated. The engine, with emergency lights activated, moved from the garage bay onto the apron. According to the police report, all doors on the engine were closed at this time; otherwise the engine would not fit through the door opening.
Traffic signal lights are located in both the east and westbound lanes of the street in front of the station. These lights remain on flash until activated to go to a solid red signal by a switch that is located on a control panel at the front desk of the fire station. The control was not activated and the lights remained flashing, thus permitting normal traffic flow. After moving onto the apron, a vehicle approaching from the left caused the driver to sound the siren and come to a complete stop before entering the street. After stopping, the engine made a sharp turn to the right crossing slightly over the center line before continuing straight at an estimated speed of approximately five mph. Fire fighters on the engine could not verify the victim’s actions during this time. However according to the police investigation, witnesses reported that the victim may have been donning gear as the engine left the station and he appeared to be standing facing forward when the engine straightened out of the right turn after leaving the apron. Eyewitness accounts indicate that, while standing, the victim appeared to rotate to his left and subsequently fall from the driver side jump seat door onto the eastbound traffic lane. It is reported that he landed on his right foot and then fell backwards striking his head on the pavement.
The fire fighter who was seated adjacent to the victim in the passenger side jump seat realized the victim had fallen and called for the driver to stop. Simultaneously, the driver reported hearing a “banging sound, like metal” and when he looked in the side-view mirror he saw the driver side jump seat door open and the victim lying on the street. He immediately stopped the engine and all personnel onboard rushed to provide emergency care to the victim, and provide traffic control around the incident. Fire fighters radioed for assistance and requested emergency medical services be dispatched to the scene. Due to the reported severity of the victim’s injuries, a nearby ambulance was re-directed to the incident.
Paramedics arrived within minutes and transported the victim to a local hospital. He died from his injuries three days after the incident, on May 3, 2004.
The death certificate listed the cause of death as blunt force head trauma.
Discussion: Fire fighters and emergency responders make many life-and-death decisions during a tour of duty, and one of the most important for their own safety is securing their seat belt or restraint device after climbing aboard a responding emergency apparatus. It is critical that personnel remain seated and restrained until they have arrived at their destination and the apparatus has come to a safe stop.3
NFPA 1500 Standard on fire department occupational safety and health program4 specifies the minimum requirements for an occupational safety and health program for a fire department. Section 6.3.2 states that, “seat belts shall not be released or loosened for any purpose while the vehicle is in motion, including the donning of respiratory protection equipment or protective clothing.” Departments should establish SOPs that clearly define requirements for riding in emergency apparatus. They should enforce and repeatedly train all personnel on the safety requirements, including the use of safety restraints when riding in emergency vehicles. Additionally, drivers should ensure that riders are seated and restrained before moving the apparatus.
During the police investigation immediately following the incident, the victim’s seat belt was found wedged under the seat cushion, indicating that the belt was not being worn.
Discussion: It is extremely important that a system is in place to ensure every piece of emergency equipment, and apparatus, is functional and safe. Preventative maintenance should be conducted at periodic intervals with results, and any required remedies, documented. The safety of responding personnel must be of paramount importance to fire departments.
Maintenance checks should include an inspection of all seat belts and safety restraints to ensure they are securely mounted and operate freely. Webbing must not be cut or frayed and buckles must open and close properly. The location of the seat belts or safety restraints should confirm that they are positioned to be worn. A check of the apparatus following the incident found the victim’s seat belt lodged beneath the bottom seat cushion.1, 5
Discussion: The 2003 edition of the NFPA 1901 Standard for automotive fire apparatus5, specifies the minimum design requirements and building specifications for new automotive fire apparatus. This standard is recognized as the “benchmark” from which newer apparatus are being designed. Chapter 14.1.1 states that “each crew riding position shall be within a fully enclosed personnel area.” Although newer apparatus are designed with fully enclosed cabs, older apparatus with jump seat riding areas are still in service. Some of these are equipped with safety bars or gates that are intended to prevent a fire fighter from falling out of a jump seat. However, these devices do not substitute for safety procedures that require fire fighters to ride in enclosed positions secured by an approved restraint system. It is recommended that apparatus not built to NFPA revised standards, or that was manufactured prior to 1979, should be considered for replacement or upgrading.
The engine involved in this incident was a 1976 cab-forward model and was used as a spare during maintenance operations of assigned apparatus. At the time of the incident, the engine had been retrofitted with a half-door that was equipped with a slam-lock system. The door locking mechanism included an inside vertical and thumb-rotary locking/unlocking feature. Police determined that the door locking mechanisms were operational at the time of their investigation. When police officers closed and locked the door, the handle would not move under normal pressure and the door would not open. This indicated that the lock may not have been engaged at the time of the incident.
At the time of the NIOSH investigation, the department had removed all cab-forward apparatus from service and was systematically replacing them.
Discussion: NFPA 1901, Section14.1.5 states that “all interior crew and driving compartment door handles shall be designed and installed to protect against accidental or inadvertent opening.” The requirements in NFPA 1901 pertain to new apparatus design; however, NFPA 1912 Standard for apparatus refurbishing6, specifies the minimum requirements for the refurbishing of automotive fire/rescue apparatus, and recommends in several sections that the refurbished crew compartment comply with all applicable requirements of NFPA 1901.
When at rest, the interior handle on the driver side jump seat door faces upward in a vertical position (Photo 3). Immediately following the incident, a police officer attempted to open the locked door by turning the handle and pushing his body forcefully against the door several times. These actions did not cause the door to open. The door could be opened only when it was unlocked and the handle was moved in a counterclockwise direction. These actions indicate that the door was not locked at the time of the incident.
A recessed door handle, or one that is positioned to require intentional effort or deliberate motion to activate, would provide an extra safety measure that may prevent inadvertent opening.
Discussion: NFPA 1451, Standard for a fire service vehicle operations training program7, contains the minimum requirements for a fire service vehicle operations training program. Section 8.3.6 states that “while the vehicle is in motion, the donning or doffing of equipment and personal protective clothing that requires removal of any restraining belt or device shall be prohibited.”
According to the police investigation, witnesses reported that the victim was standing, facing forward when the engine made the turn from the apron, and that he may have been putting on gear as the engine left the station. A pair of bunker pants and boots was found in the open jump seat area on top of the motor housing. Markings inside of the gear identify the victim as the owner. Records show that the victim was wearing his bunker coat but was not wearing bunker pants or boots when the incident occurred.
Fire departments should develop SOP’s, enforce their implementation, and repeatedly train on requirements for the safe donning and doffing of equipment.
a A walk-away wall bracket is a positive-latching, mechanical means of securing an SCBA in a stowed position. It is mounted to the wall directly behind the seat. The bracket is meant to secure the SCBA during transit and also provide a method for quick donning in emergency situations.
b A gas detector is an instrument that senses and measures combustible gasses.
This incident was investigated by Virginia Lutz, Safety and Occupational Health Specialist, NIOSH, Division of Safety Research, Surveillance and Field Investigation Branch.
 |
 |
 |
Photo 3. Depiction of door handle
operation |

Return to Fire Fighter Homepage
![]()
This page was last updated on 05/11/05.