
On April 4, 2004, a career fire fighter (the victim) died while fighting a night club arson fire. Crews were dispatched at 0555 hours to a reported truck fire (hazardous material incident), but arrived on the scene to discover a structure fire. Engine 50 was the first to arrive on the scene. The Captain and two crew members (a fire fighter and the victim) initiated a “fast attack.” District Chief 5 arrived on the scene and assumed command. Ladder 38 arrived shortly after Engine 50, and the Ladder 38 crew entered the building to assist the Engine 50 crew.
Fire fighters decided to exit the building as conditions were deteriorating. It is believed that the victim became separated from his crew at this time. The Incident Commander called for operations to go defensive at the same time the crews were making their way out of the building. A fire fighter from Ladder 38 reentered the building after realizing that his Captain had failed to exit with the crew. He found and dragged the Engine 50 Captain (unconscious) to safety before returning and assisting the Ladder 38 Captain (semi-conscious) out of the building. The victim failed to exit the building and was later found in the debris.
 |
Incident scene |
NIOSH investigators concluded that, to minimize the risk of similar occurrences, fire departments should
On April 4, 2004, a 32-year-old male career fire fighter (the victim) died while conducting an interior attack at a night club arson fire. On April 5, 2004, the U.S. Fire Administration notified the National Institute for Occupational Safety and Health (NIOSH) of this incident. On May 11, 2004, two Safety and Occupational Health Specialists from the NIOSH Fire Fighter Fatality Investigation and Prevention Program investigated this incident. Meetings were conducted with the Chief, Assistant Chief and a Senior Captain of the fire department, local International Association of Fire Fighters representatives, and the State Fire Marshal. Interviews were conducted with officers and fire fighters who were at the incident scene. The investigators reviewed the victim’s training records, autopsy report, and death certificate. NIOSH investigators also reviewed the department’s fireground standard operating procedures (SOPs), the fire department’s incident and quality assurance reports, a transcription of the dispatch tapes, and the State Fire Marshal’s report.
The self-contained breathing apparatus (SCBA) worn by one of the injured Captains was sent to the NIOSH National Personal Protective Technology Laboratory located in Bruceton, Pennsylvania for further evaluation. The findings of the evaluation can be found in the Appendix.
Fire Department
The career department involved in this incident is comprised of 3,875 uniformed
fire fighters serving a population of approximately 1.9 million in a geographical
area of about 620 square miles.
Training and Experience
The fire department requires all new fire fighters to complete 640 hours of
fire fighter training and 240 hours of emergency medical technician training
before they are assigned to a station. Following a station assignment, all new
fire fighters are required to complete a 12-month probationary period.
The victim was a fire fighter who had approximately 17 years of experience with a volunteer fire department and approximately 7 months of experience with this department. The victim attended the fire department’s training academy and was certified NFPA Fire Fighter Level I and basic emergency medical technician (EMT-B).
The Captain from Engine 50 (Captain #1) had approximately 5 years of experience with a volunteer fire department prior to being hired in January of 1993 by this department. The experience with this career department included NFPA Fire Fighter Level II, emergency medical technician (EMT-A) and paramedic training, followed by an assignment as a paramedic. The Captain served as a paramedic prior to his promotion to Engineer/Operator in January of 1997. He was promoted to Captain in December of 2000 and assigned to Central Dispatch prior to being assigned as the officer for the Engine 50 crew on December 22, 2001.
Equipment and Personnel
0555 hours - Initial dispatch (hazardous materials box alarma)
included:
DC-5 (District Chief (Incident Commander [IC]) and Chief Officer (driver and Fire Sector Officer));
Engine 50 (Captain #1 [injured], driver/operator and two fire fighters [Fire Fighter #1 and the victim]);
Engine 5 (Captain, driver/operator, and two fire fighters);
Hazmat Unit 1 (Captain, driver, and two fire fighters);
Hazmat Unit 2 (Acting Captain, driver, and two fire fighters);
Ladder 38 (Captain #2 [injured], driver/operator, and two fire fighters [Fire Fighter #2 and Fire Fighter #3]);
Safety 2 (Captain);
Medic 50 (one EMT);
Ladder 4 (Captain, driver/operator, and two fire fighters);
0604 hours - A second hazardous materials box alarm
DC-4 (District Chief);
Engine 38 (Captain, driver/operator, and two fire fighters);
Engine 13 (Captain, driver/operator, and two fire fighters);
District Chief Safety Officer 15 (Chief Officer);
Ambulance 38 (two paramedics);
Foam 22 (driver/operator);
Ladder 77 (Captain, driver/operator, and two fire fighters);
Ladder 67 (Captain, driver/operator, and two fire fighters);
Shift Commander 17 (Chief Officer);
Cascade Truck 2 (operator).
Additional units were dispatched; however, only those units directly involved in operations preceding the fatal event are discussed in the investigation section of this report.
Electronic Accountability System
The electronic accountability system utilized at this incident requires that
each fire fighter be assigned an electronic personal alert safety system (PASS)
device. This PASS device is independent from the integrated PASS device of the
self-contained breathing apparatus that the fire fighters were wearing at the
time of the incident. Each electronic PASS device is assigned an identifier
(e.g., E50A that identifies the Captain from Engine 50). The electronic PASS
device transmits a continuous radio signal to a base receiver that is maintained
and monitored at the command post. The base receiver provides an audible and
visual status of each fire fighter on the fireground. An evacuation signal can
be transmitted from the base receiver to all PASS devices where a distinct audible
alarm alerts fire fighters to exit the building. The fire fighters manually
reset their unit which sends an acknowledgement signal to the base unit.
Structure
This structure had various construction methods and materials. The walls, ceilings
and known interior finishes varied throughout the structure and a significant
portion could not be determined due to the extent of fire damage. The structure
had three sections, with the middle section being the original building, and
the west and east sections added on at later dates (Diagram
1).
The exterior walls of the original (middle section) building consisted of concrete blocks with a stucco finish. Steel I-beams supported the gable design with a limited slope roof system that consisted of metal affixed to “S” channel. The interior wall and ceiling finish could not be conclusively determined; however, a portion of this wall appeared to be made of concrete blocks.
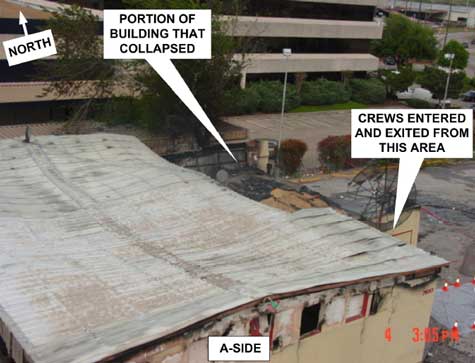
The construction material of the walls of the two additions varied, with portions consisting of concrete blocks, while other sections had wood framing (2x4 construction). The addition on the east end of the building had a roof constructed of wood and was overlaid with asphalt shingles. The pitch of the roof was not significant enough to ensure proper water runoff. The construction of the walls of the west end of the building was very similar to the addition made to the east end of the building. The roof was constructed of wood and was overlaid with a built-up tar and gravel roof. The pitch of the roof at the west end of the building was also not significant enough to ensure proper water runoff. Note: The two additions collapsed prior to recovering the victim. However, the victim was found in the original (middle section) building that had not collapsed (Diagram 2).
Arson investigators determined that the fire was incendiary in nature. A petroleum-based accelerant was ignited at several points around the perimeter.
a This fire department’s hazardous materials box alarm consists of the dispatch of two engine and two ladder companies, one chief officer, one safety officer, two hazardous materials units, and an ambulance.
At approximately 0555 hours, crews were dispatched to a reported truck fire (hazardous material incident). At approximately 0603 hours, Engine 50 arrived on the scene and the Captain (Captain #1) radioed Central Dispatch reporting that they had “heavy smoke” but had not found the address.
At approximately 0604 hours, District Chief 5 (DC 5) arrived on the scene, established Incident Command, and reported to Central Dispatch that “it is a building fire at the dispatched location.” Captain #1 reported to Central Dispatch that they had a “one-story commercial building on fire” and that they were going to make an “interior fast attack.” Central Dispatch advised all units that this incident would be operating on Tactical Channel 7. Ladder 38 arrived on the scene. A second Hazmat alarm was dispatched to complete the Box Alarm.
At 0605 hours, the Engine 50 crew stretched 200-feet of 1 ¾-inch pre-connect handline and positioned themselves at the main entrance (A/D corner, Diagram 1). Captain #1 conducted a partial size-up as he walked through a crowd of people that had gathered in the parking lot on the east end of the building (Side D). There was no visible fire observed on the exterior of the building by the first arriving units. Officers and fire fighters reported to NIOSH investigators that they observed heavy dark smoke emitting from the northwest corner of the structure upon their arrival.
At approximately 0606 hours, the Engine 50 crew reported to the Incident Commander (IC [DC-5]) that they were making an interior fast attack and that the owner of the building informed them that there were propane tanks located inside the rear of the building. The IC assigned Ladder 38 to Sector 1 (interior). The IC assigned Engine 5 to set up and maintain the electronic accountability system. The crew of Engine 5 was also assigned to be the Rapid Intervention Team (RIT).
At approximately 0608 hours, the Engine 50 crew advanced the 1 ¾-inch handline into the building. Crew members reported to NIOSH investigators that smoke was emitting from the top of the door. The victim was on the nozzle followed by Fire Fighter #1 and Captain #1. The three entered and proceeded along the wall to their right. The crew advanced the handline approximately 10 feet before stopping. The crew decided to pull back to the front door after having difficulty finding the seat of the fire. Note: The smoke was banked down to approximately 3 feet from the floor with no visible fire and very limited visibility. After regrouping, Fire Fighter #1 reentered as the nozzleman, followed by the victim and Captain #1. Ladder 38’s crew made their way to the front door with a 1 ¾-inch handline as the Engine 50 crew advanced their handline for the second time. Captain #2 from Ladder 38 asked Captain #1 if they had found the fire. Captain #1 replied that they had not. The fire fighters from Ladder 38 pulled some slack on the 1 ¾-inch handline as it was caught on the exterior corner of the building near the entrance. As the Engine 50 crew advanced the handline toward the north wall, they encountered zero visibility and high heat conditions. There was no visible fire at this time as Fire Fighter #1 sprayed short bursts of water at the ceiling in an attempt to cool down the room.
At approximately 0609 hours, the IC radioed the Fire Sector Officer and informed him that “heavy fire is showing through the roof now.” Approximately two minutes later, the Fire Sector Officer radioed Captain #1 and informed him that “the propane bottles are at the base of the fire” and that “the fire has broken through the roof.” Captain #1 acknowledged the transmission and then told his crew that it was time to exit the building.
At approximately 0612 hours, Captain #1 began following the hoseline when his low-air alarm sounded. He had taken only 2-3 short breaths when he completely ran out of air.b He then disconnected his mask-mounted regulator to radio for assistance. He was quickly overcome by the toxic smoke and collapsed. Fire Fighter #1 could hear some commotion as if someone had knocked something over behind him. He then heard someone yelling something, but he could not understand what was being said. Fire Fighter #1 then heard someone yell “let’s get out of here.” There was a sudden increase in visible fire and heat. Fire Fighter #1 then dropped the nozzle and proceeded to follow the handline toward the door. The IC radioed the rapid intervention team (RIT), instructing them to check on the Engine 50 crew. Note: The RIT did not enter the building at this time. The IC followed up that radio transmission by ordering all companies to go defensive and instructing the accountability officer to activate the “evacuation mode” on the electronic accountability system command base. Fire Fighter #2 and Fire Fighter #3 from Ladder 38 had followed the handline into the structure (approximately 15 feet) when they encountered an increased heat level. The two fire fighters began to follow the handline out when a sudden increase in heat caused them to think that they were heading in the wrong direction. After getting their bearings, they continued down the handline until they reached the door. They then saw Fire Fighter #1 exit behind them. Fire Fighter #2 quickly realized that his Captain (Captain #2) had not exited. The IC ordered all apparatus to sound their air horns notifying everyone on the fireground that the operation had gone defensive and for everyone to exit the building. A personnel accountability report (PAR) was requested by the IC at this time.
At approximately 0615 hours, Fire Fighter #2 re-entered and followed the handline. He came across a downed fire fighter (Captain #1 from Engine 50). Fire Fighter #2 radioed that he had “a fire fighter down.” He dragged Captain #1 to the front door where Fire Fighter #1 and Fire Fighter #3 assisted in getting the Captain moved away from the building before removing his gear. Fire Fighter #2 realized that his Captain (Captain #2) was also still inside. He re-entered for a second time and found Captain #2 stumbling toward the front door. Note: Captain #2 reported to NIOSH investigators that he had become disoriented after being struck in the left shoulder (he was not sure what had struck him) and knocked into a table. Captain #2 also reported that he had experienced intense heat the entire time he was searching for the handline. As Fire Fighter #2 assisted Captain #2 out of the building, the entire room lit up as fire began rolling out the front door.
At approximately 0617 hours, a crew member from Ladder 38 radioed command reporting that all personnel were accounted for from Engine 50 and Ladder 38. Note: A fire fighter was misidentified as the victim when a personnel accountability report (PAR) was requested. The victim was not assigned to the crew that had responded on Engine 50. He had arrived at work early and relieved the fire fighter assigned to this crew. The Incident Commander was given a PAR. After receiving the PAR, the IC made a radio transmission that this was a defensive fire and ordered everyone away from the building.
At approximately 0624 hours, Medic 50 left the scene transporting Captain #1 to an area hospital. The IC radioed Medic 50 asking if they were transporting Captain #1. Medic 50 confirmed that they were transporting Captain #1 and treating him for smoke inhalation.
At approximately 0630 hours, a crew member from Engine 50 reported to command that they could not account for a fire fighter (the victim) from Engine 50. The IC attempted to radio the victim but did not get a response. Safety 2 began searching the area around the apparatus looking for the victim. The accountability officer checked the electronic accountability system and reported to the IC that the system had accounted for everyone. Note: The base unit had been reset with two electronic PASS devices indicating that they were timed out (not in alarm status) after the evacuation of the building. The operator, who had reset the alarm, surmised that the electronic PASS devices belonged to the two injured fire fighters being transported to the hospital. Numerous attempts were made to physically locate the victim outside of the building.
At approximately 0650 hours, the IC radioed Central Dispatch asking them to contact all of the ambulances that had left the scene to report if they had the victim with them. The IC was then informed that all ambulances had reported that they did not have the victim with them, and that Captain #2 was being transported in Ambulance 13 to an area hospital.
At approximately 0659 hours, the IC ordered Ladder 38 to shut down their ladder pipe. Numerous crews attempted to search the building. Eight minutes later, the search was suspended as the building conditions were too dangerous to continue. Approximately 14 minutes later, a second search was initiated. At approximately 0722 hours, a radio transmission was made that an alarming PASS device could be heard. The IC then ordered all companies to shut down their operations and their engines. Approximately three minutes later the IC was informed that the victim had been found in the debris (Diagram 2 and Photo).
b The self-contained breathing apparatus (SCBA) was evaluated by NIOSH. The findings of the evaluation can be found in the Appendix.
Captain #1 was treated for smoke inhalation (Carboxyhemoglobin saturation level was 27%) and minor burns on his right hand. Captain #2 was treated for smoke inhalation.
The autopsy report listed the victim’s cause of death as high thermal exposure.
Discussion: The initial size-up conducted by the first arriving officer allows the officer to make an assessment of the conditions and to assist in planning the suppression strategy. The following general factors are important considerations during a size-up: occupancy type involved, potential for civilians in structure, smoke conditions, type of construction, age of structure, exposures, and time considerations such as time of incident, time fire was burning before arrival, and time fire was burning after arrival. The evaluation of risk is an assignment that the first arriving officer or Incident Commander is designated to conduct. The Incident Commander must perform a risk analysis to determine what hazards are present, what the risks to personnel are, how the risks can be eliminated or reduced, and the benefits to be gained for both interior or offensive operations.1
The first arriving officer conducted a partial size-up in terms of evaluating the conditions and type of building, the extent of fire spread and exposures. However, a size-up report was not provided to Central Dispatch or responding units, including the IC. Personnel reported to NIOSH investigators that they observed heavy dark smoke emitting from the northwest corner of the structure upon their arrival. There were no reports of civilians in the building upon Engine 50’s arrival, nor were any civilians located in the building at anytime during or after the incident.
Discussion: Frequent progress reports are essential to the Incident Commander’s continuous assessment and size-up of the incident. Interior crews and crews working in areas not visible to the Incident Commander are the eyes and ears of the IC. Progress reports also provide everyone on the fireground with information on other aspects of the fire that relate to their own particular operations (e.g., ventilation, suppression, primary search, etc.).2
The interior crews experienced high heat conditions, zero visibility and were having difficulty locating the seat of the fire. All of these factors are important details that the IC needs to evaluate when establishing and maintaining a plan of action. Progress reports were not provided to the IC by the interior crews.
Discussion: The fire department involved in this incident has an established standard operating procedure (SOP) regarding thermal imaging camera use at structure fires. The SOP states “Senior Captains/Captains will be responsible to ensure that the thermal imaging camera (TIC) is removed from their assigned apparatus and deployed on every dispatched structure fire and other identified situations that will enhance the safety of fire fighting personnel or rescue operations.” The SOP outlines and prioritizes the various situations for the use of the TIC. The SOP also states “the TIC will be utilized in every structure fire” with priority given to search and rescue operations followed by the fire attack and rapid intervention teams.3 A thermal imaging camera was available but not utilized during the early stages of this incident as per the SOPs.
Discussion: Annual refresher training provides an opportunity to ensure that all fire fighters and line officers are proficient in their knowledge and skills in recognizing and mitigating hazards. Annual refresher training on structural fire fighting should include, but not be limited to, departmental standard operating procedures, fire fighter safety, building construction, and fireground tactics.4 NFPA 1500, chapter 5, requires that the fire department provide an annual skills check to verify minimum professional qualifications of its members.5 Training is an ongoing process, whether held daily, weekly or monthly, which allows members to maintain proficiency at their present levels, meet certification requirements, learn new procedures, and keep up with emerging technology.6
Discussion: For newly appointed, promoted, or reassigned officers, a department’s orientation and training program can help to ensure that their officers have the skills, knowledge and abilities to be successful in their newly assigned position. The fire department can also establish a certification program where a designated committee defines the requirements of the company officer’s job and the competency requirements that address the knowledge, skills, and abilities needed to perform that job.6 As part of an overall training program, a newly appointed officer could serve as an aid to a Chief Officer, gaining further knowledge and experience while under the supervision and guidance of a seasoned professional.
Discussion: When fire fighters enter smoke-filled structures, the visibility is usually very poor, thereby reducing the possibilities of easily identifying each other. Some fire departments color code their helmets so fire fighters, officers, or the chief can be easily identified on the fireground. Fire departments can also use name, number, or company emblems to identify each individual fire fighter on the fireground. This could assist fire fighters on the fireground to identify fellow crew members.7 This becomes more of a factor in larger fire departments where new members are assigned to a crew or a member fills in at a station short on manpower. Team continuity also plays a vital role in accountability as it allows the company officer or senior fire fighter to quickly account for crew members.
The fire department involved in this incident utilizes an electronic accountability system. The system requires that each fire fighter is assigned an electronic personal alert safety system (PASS) device. This PASS device is independent from the integrated PASS device of the self-contained breathing apparatus that the fire fighters were wearing at the time of the incident. Each electronic PASS device is assigned an identifier (e.g., E50A that identifies the Captain from Engine 50). However, the PASS device does not identify the individual by name. Utilizing identification emblems on helmets or turnout gear in conjunction with the electronic accountability system would aid in the identification of individual members at the fire scene.
This incident was investigated by Mark McFall and Jay Tarley, Safety and Occupational Health Specialists, Surveillance and Field Investigations Branch, Division of Safety Research, NIOSH.
 |
 |
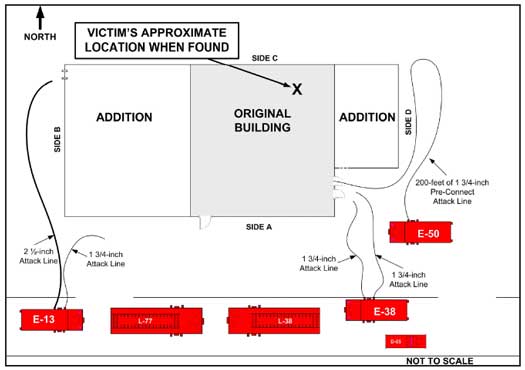 |
Diagram 2. Aerial view of incident site. |
Status Investigation Report of One
Self-Contained Breathing Apparatus
NIOSH Task No. 13617
Background
As part of the National Institute for Occupational Safety and Health
(NIOSH) Fire Fighter Fatality Investigation and Prevention Program,
the National Personal Protective Technology Laboratory’s Respirator Branch
agreed to examine and evaluate one Scott 4500 psi, 30-minute, self-contained
breathing apparatus (SCBA). This SCBA status investigation was assigned NIOSH
task number 13617.
The SCBA, sealed in a corrugated cardboard box, was delivered to the NIOSH facility in Bruceton, Pennsylvania on July 16, 2004. Upon arrival, the sealed package was taken to the Firefighter SCBA Evaluation Lab in building 108 and stored under lock until the time of the evaluation.
SCBA Inspection
The package was opened and the SCBA inspection was performed on October 28,
2004. The SCBA was examined, component by component, in the condition as received
to determine its conformance to the NIOSH-approved configuration. The entire
inspection process was videotaped. The SCBA was identified as the Scott Air-Pak
4.5 model.
The SCBA shows signs of heavy use and wear, and was overall in good to fair condition. The backframe and harness in particular have suffered damage, and many of the labels, including the NIOSH approval label and NFPA certification label, are absent from the SCBA.
Personal Alert Safety System (PASS) Device
Two Personal Alert Safety System (PASS) devices are included with this SCBA—an
integrated device and a stand-alone device which is clipped to the left shoulder
strap. The integrated device is approved by NIOSH as an accessory to this SCBA,
but the stand-alone device has not been evaluated by NIOSH. During the inspection,
attempts were made to activate both PASS devices manually and automatically.
The integrated unit appeared to function normally although the low-battery signal
sounded and some damage was noted to the console. The stand-alone unit did not
activate at all. Neither unit was tested against the specific requirements of
NFPA 1982, Standard on Personal Alert Safety Systems (PASS), 1998 Edition.
Since NIOSH does not certify PASS devices, no further testing or evaluations
were conducted on the PASS units.
SCBA Testing
The purpose of the testing was to determine the SCBA’s conformance to
the approval performance requirements of Title 42, Code of Federal Regulations, Part 84 (42
CFR 84). Further testing was conducted to provide an indication of the SCBA’s
conformance to the National Fire Protection Association (NFPA) Air Flow Performance
requirements of NFPA 1981, Standard on Open-Circuit Self-Contained Breathing
Apparatus for the Fire Service, 1997 Edition. As the unit provided to NIOSH
did not include a facepiece or cylinder, substitutes were used where needed.The
following performance tests were conducted on the SCBA:
NIOSH SCBA Certification Tests (in accordance with the performance requirements of 42 CFR 84):
1. Positive Pressure Test [§ 84.70(a)(2)(ii)]
2. Rated Service Time Test (duration) [§ 84.95]
3. Static Pressure Test [§ 84.91(d)]
4. Gas Flow Test [§ 84.93]
5. Exhalation Resistance Test [§ 84.91(c)]
6. Remaining Service Life Indicator Test (low-air alarm) [§ 84.83(f)]
National Fire Protection Association (NFPA) Tests (in accordance with NFPA 1981, 1997 Edition):
7. Air Flow Performance Test [Chapter 5, 5-1.1]
Testing was conducted on October 28, 2004. All testing was videotaped with the exception of the Exhalation Resistance Test and Static Pressure Test. The SCBA met the requirements of each test. However, during the Rated Service Time Test the low-air alarm activated intermittently. This did not cause the unit to fail the test, but normally the alarm activates continuously until the cylinder is exhausted.
Summary and Conclusions
The SCBA was submitted to NIOSH for evaluation was delivered to NIOSH on July
16, 2004 and inspected on October 28, 2004. The unit was identified as a Scott
Air-Pak 4.5 30-minute, 4500 psi, SCBA (NIOSH approval number TC--13F--76). The
SCBA was determined to be in a condition safe for testing.
The unit was subjected to a series of seven performance tests on October 28, 2004. Although the SCBA met the requirements of all tests, the low-air alarm activated intermittently during the Rated Service Time Test. No maintenance or repair work was performed on the unit at any time.In light of the information obtained during this investigation, the Institute has proposed no further action at this time. Following inspection and testing, the SCBA was returned to the package in which it was received and stored under lock in building 108 at the NIOSH facility in Bruceton, Pennsylvania pending its return.
If the SCBA is to be placed back in service, it must be thoroughly inspected and repaired by a qualified service technician. The batteries in the integrated PASS device should be replaced and the console repaired. The stand-alone PASS device should be brought into working order or removed from the SCBA. Replacement labels should be affixed to the backframe and the damaged parts of the harness replaced.

Return to Fire Fighter Homepage
![]()
This page was last updated on 09/15/05.