
Career Fire Fighter Dies After Becoming Trapped by Fire in Apartment Building – NJ
SUMMARY
 |
| Building involved in fire. |
NIOSH investigators concluded that, to minimize the risk of similar occurrences, fire departments should
Additionally, municipalities should consider
INTRODUCTION
On May 9, 2001, a 40-year-old male career fire fighter (the victim) died after he became trapped in a third-floor apartment while searching above the fire for occupants. The fire fighter assist and search team (FAST) made several attempts to locate the victim but were unsuccessful due to the fire spread and deteriorating conditions of the building. The victim was located in the bedroom of a third-floor apartment, and he was pronounced dead at the scene.
The National Institute for Occupational Safety and Health (NIOSH) was notified of this incident on May 10, 2001, by the United States Fire Administration. On July 15, 2001, three Safety and Occupational Health Specialists from NIOSH’s Fire Fighter Fatality Investigation and Prevention Program investigated this incident. Meetings were conducted with the Chief of the department, an arson investigator from the county prosecutor’s office, and the supervisor of fire department programs for the State of New Jersey. Interviews were conducted with the officers and fire fighters involved in this incident. NIOSH investigators reviewed the arson investigator’s copies of site maps, drawings, photos, and witness statements. The department’s standard operating procedures, dispatch run sheets, and the victim’s training records were also reviewed. The victim’s SCBA was sent to the NIOSH Respirator Branch in Morgantown, West Virginia, for further evaluation. The purpose of the testing was to determine the SCBA’s conformance to the approval performance requirements of Title 42, Code of Federal Regulations (CFR), Part 84, Subpart H. Further testing was conducted to determine conformance to the National Fire Protection Association (NFPA) Air Flow Performance requirements of NFPA 1981, 1997 Edition. A series of tests utilizing a Biosystems PosiChek3 computerized SCBA performance tester were also conducted. The victim’s facepiece had sustained some damage to the chin area. A replacement AV-2000 facepiece was used during the testing of the SCBA unit. The SCBA met the requirements of all six NIOSH SCBA certification tests performed. The SCBA also met the requirements of the NFPA Air Flow Performance Test and all tests performed using the Biosystems Posichek3 (a summary of this report is included as Appendix A).
A site visit was conducted and the incident site photographed. The site of the incident is a three-story apartment building of ordinary construction. The building’s exterior walls were constructed of noncombustable materials (brick), and the floors, roof, and interior partitions were made of combustable materials (wood). Each floor has four apartments.
A follow-up visit was conducted on August 26, 2001, to interview the Chief of the Department, officers, and fire fighters involved in this incident. The fire department involved in this incident consists of 2 stations with a total of 117 uniformed fire fighters. The department serves a population of 70,000 in a geographic area of 3.2 square miles. The department requires all new fire fighters to complete 320 hours of training in basic fire fighting with a 1-year probationary period. The victim was NFPA-certified as Fire Fighter Level I and Level II with 10 years of fire fighting experience with the department. The victim received training in the following areas: apparatus/engine operator, aerial tiller training and testing, hazardous materials, fire inspector, apparatus operation, search and rescue, live fire training, and basic life support. The victim was certified as an emergency medical technician.
INVESTIGATION
On May 9, 2001, at 2037 hours, Central Dispatch received a call from a civilian reporting a structure fire. The career department was notified at 2037 hours, and the following apparatus responded: Engine 1 (Lieutenant, driver/operator, and fire fighter), Engine 2 (Lieutenant, driver/operator, and fire fighter), Engine 3 (Lieutenant, driver/operator, fire fighter), Truck 2 (Captain, Fire Fighter #1 [driver], and victim [tiller operator]) and Deputy Chief 4 (DC 4). Engine 2 was the first to arrive on the scene at 2039 hours, followed immediately by Truck 2. The Lieutenant of Engine 2 reported to Central Dispatch that they had a working fire in a three-story brick building with fire showing in the rear. He requested that all companies make hydrant connections. The driver of Engine 2 parked the apparatus to the north of the incident site on the A-Side of the building (See Diagram 1). Truck 2 parked directly behind Engine 2. The Lieutenant of Engine 2 then pulled the 200-foot, 1¾-inch preconnect "minute-man pack" from the passenger’s side of the apparatus. As the Lieutenant from Engine 2 stepped back off the apparatus, he fell, twisted his ankle, and dropped the "minute-man pack." He then picked up the pile of hose and proceeded toward the street level door on the A-Side of the building. The fire fighter on Engine 2 proceeded toward the corner hydrant, to the north (approximately 160 feet) of Engine 2, with 400 feet of 4-inch supply line. Engine 3 arrived on the scene. At 2040 hours, DC 4 arrived on the scene, assumed incident command (IC), and conducted his initial scene size-up. A police officer approached him and reported that civilians were trapped on the second floor in Apartment #7. Note: Other reports from civilians were that the trapped civilians were a mother and her two children.
The IC informed the Captain of Truck 2 of the trapped civilians. Fire Fighter #1 and the victim were standing near Truck 2 when they heard civilians yelling that there were people in Apartment #7. They proceeded to the building to conduct a primary search. The Lieutenant from Engine 3 made forcible entry to the street-level door on the A-Side of the building. The Lieutenant from Engine 2 then followed the Lieutenant from Engine 3 into the first floor of the building with the preconnect from Engine 2. Note: Fire fighters and officers reported to NIOSH investigators that the conditions on the first floor were clear with little to no heat, and that the conditions encountered on the second floor were light smoke with some heat.
At 2041 hours, Engine 1 arrived and was ordered by the IC to stand by. The IC then called Central Dispatch and requested another engine. The Lieutenant from Engine 3 proceeded up the stairwell to the second floor and to the rear (C-Side) of the building. Following the Lieutenant from Engine 3, the Lieutenant from Engine 2 entered the building and dropped the "minute-man pack" in the stairwell. He proceeded with the nozzle to the second-floor landing and down the hallway toward the rear (C-Side), where he met the Lieutenant from Engine 3. At 2042 hours, Engine 4 (Lieutenant, driver/operator, and fire fighter) responded to the scene. The Lieutenant from Engine 3 forced open the door to Apartment #8 and encountered heavy heat, fire, and smoke. Note: Fire fighters and officers reported to NIOSH investigators that no civilians were seen or found inside the building at any time.
The Captain from Truck 2 followed the hoseline into the building, unkinking the hoseline as he proceeded to the second floor to join the two Lieutenants at Apartment #8. The IC radioed the Lieutenant from Engine 3 to ascertain that they had made entry into the apartment. Replying in the affirmative, the Lieutenant then radioed to the pump/operator of Engine 2 to charge the line. He began hitting the fire in the rear of the apartment but was having problems with low water pressure on the line. At 2043 hours, the pump/operator radioed the Lieutenant of Engine 2 that he was having problems with the throttle at the pump panel. Note: The low-pressure problem resulted from throttle problems at the pump panel and the kinks in the charged line in the stairwell.
The victim (carrying a sledgehammer) and Fire Fighter #1 (carrying a flathead ax) conducted a primary search of three second-floor apartments (#5, #6, and #7) while the two Lieutenants (from Engine 2 and Engine 3) and the Captain (Truck 2) were attacking the fire in the fourth apartment (Apartment #8). No civilians were found on the second floor. At 2044 hours, the interior attack team called for more water pressure. The Engine 2 pump/operator replied that he was still having problems with the throttle mechanism. Engine 4 arrived, and the IC ordered them in for additional manpower. The victim and Fire Fighter #1 ascended the stairwell toward the third floor where they encountered heavy smoke and high heat. The victim and Fire Fighter #1 descended the stairwell to the second-floor landing. Fire Fighter #1 told the victim to stay on the hoseline and to help the Lieutenants in Apartment #8 while he went to get some box lights from the truck. Note: The box lights were to be placed at the top of the third-floor landing as a reference for their point of egress.
At 2045 hours, fire fighters stretched a 1¾-inch backup line from Engine 2 to the second floor. At 2046 hours, members of a mutual-aid company began responding to the incident. At 2047 hours, the IC called Central Dispatch and requested Truck 1, which responded with a Lieutenant, driver, and a fire fighter. The victim radioed Engine 2 that he was trapped on the third floor. Note: For approximately the next 70 seconds, the only radio traffic was between the IC and the Truck 1 officer, who were discussing the assignment and placement for Truck 1 upon their arrival. The IC and the Truck 1 officer did not discuss the victim. The fire department has only one radio channel available to be used as the tactical and fireground channel.
At 2049 hours, the victim radioed Truck 2, reporting that he could not breathe and that he was trapped on the third floor. The victim radioed a third transmission that he was on the third floor, trapped, and needed help. The Lieutenant from Engine 3 heard the victim’s third radio transmission and called "Mayday - Mayday" over the radio. The victim made a fourth transmission that he was on the third floor, trapped, and needed help. Central Dispatch transmitted, "We got a Mayday, Mayday. Dispatch, Dispatch to Deputy 4. We got a Mayday calling from the third floor." Command acknowledged Central Dispatch’s notification of the Mayday. Trying to determine the victim’s location, the Lieutenant from Engine 3 maintained radio contact with him. The victim responded that he was on the third floor, upstairs, and to the right. At 2050 hours, the victim radioed that there was heavy fire and that he couldn’t get out. Approximately 1 minute later, he radioed that he was running out of air. The Lieutenant made numerous calls for a line to be brought up to the third floor. At 2052 hours, Truck 1 arrived and parked in the lot on the D-Side of the fire building (See Diagram 1). Approximately 13 minutes after the victim had arrived on the scene, at 2053 hours, he made his final transmission that he was out of air. At 2054 hours, the IC radioed for the mutual-aid company to report in as a fire fighter assist and search team (FAST). The Lieutenant from Engine 3 told Fire Fighter #1, who had just returned to the second-floor landing, that the victim had radioed that he was trapped in a third-floor rear apartment. The Lieutenant from Engine 2 attempted to stretch the initial attack line up the stairwell to the third floor but found that the line would not reach the rear apartments. Note: The line was still fully charged and kinked in the stairwell between the first and second floors.
Fire Fighter #1 followed the Lieutenant from Engine 2 to the third floor; however, he was forced to exit the building because he was low on air. The Lieutenant from Engine 3 advanced a handline down the hall toward Apartment #6 where he received an electric shock while attempting to knock down the fire. Note: The department’s SOPs list the shutting off of utilities as a Truck company function.
At this incident, Truck 2 was immediately assigned to conduct a search for trapped civilians. Two fire fighters assisted the Lieutenant from Engine 3 out of the building, and emergency medical technicians (EMTs) provided him medical attention. Fire Fighter #1 got a ladder off Truck 2 and proceeded to the D-Side of the building. He positioned the ladder beneath the window of the third-story apartment where he believed the victim was located. Fire Fighter #1 broke the window, which was located in the kitchen of Apartment 12. He was unable to gain entry because a refrigerator blocked the window (See Diagram 2 and Photo). At 2055 hours, a radio transmission was sent out asking the victim if he was still on the radio. The victim did not reply. The Administrative Director of the department arrived at this time to provide logistical support. At 2100 hours, the Chief of the department arrived and assumed command from the IC. Mutual-aid also arrived at this time. The IC radioed Central Dispatch requesting another engine and truck company for manpower. At 2102 hours, the fire fighter in the bucket of Truck 1 radioed that heavy fire was coming through the roof and the third floor rear. At 2103 hours, Engine 2 (additional mutual-aid) arrived. At 2104 hours, the IC radioed Central Dispatch for an additional ambulance. At 2105 hours, the fire fighter in the bucket of the ladder of Truck 1 radioed the IC that the rear of the third floor was fully involved. The Lieutenant from Engine 2 radioed from the interior that the rear of the second floor was fully involved. At 2107 hours, the fire fighter in the bucket of Truck 1 radioed the IC to get the fire fighters out of the building because "the whole rear of the roof is lit up." At 2110 hours, the fire fighter in the bucket of Truck 1 reported to command that the roof had partially collapsed into the third floor. At 2111 hours, the IC radioed Truck 1 on the status of the roof, and the fire fighter replied that "the rear of the building has collapsed and the front is lighting up." The IC then ordered an evacuation of the building and a personnel accountability report (PAR) from all units. Truck 1 and Engine 2 knocked down the fire with master streams, allowing the fire fighter assist and search teams (FAST) several attempts to locate the victim. Note: The FAST was comprised of the on-duty personnel on the scene and not the mutual-aid company. While the FAST was operating on the interior of the building, the Administrative Director ordered Truck 1 to hit the fire on the roof with the aerial appliance. Fire fighters reported to NIOSH investigators that during one of the search attempts, water applied to the roof by the aerial appliance forced the FAST to retreat down the hall.
With each attempt by the FAST to locate the victim, the fire spread and conditions deteriorated in the building. The IC called for additional evacuations. On the fourth attempt by the FAST to find the victim, a Captain was using a thermal imaging camera when a member of the team heard a PASS device coming from Apartment #12. The FAST entered Apartment #12 and discovered the refrigerator door open in front of the door to the bedroom where the victim was found (See Diagram 2 and Photo). The victim was lying face down on his PASS device, which was activated but barely audible. The victim was unresponsive and not breathing. Note: There was a wall-mounted mirror in the bedroom that had been broken by the victim. The victim had struck the mirror and the wall numerous times with his sledgehammer. The mirror may have appeared to the victim to be a window. Paramedics responded to the third floor where they pronounced the victim dead. The victim was then removed from the building at approximately 2300 hours.
CAUSE OF DEATH
The death certificate lists the cause of death as asphyxiation.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Fire departments should ensure that the department’s standard operating procedures (SOPs) regarding structure fires are followed unless otherwise directed by the Incident Commander. 1
Discussion: The department’s SOPs for structure fires state that "where a large body of fire exists, a 2½-inch line shall be the initial attack line unless otherwise directed by the Incident Commander." The SOPs also state that "the second due engine company shall provide a second attack line of equal capacity or larger to the initial attack line." At this incident, the first arriving units reported to Central Dispatch that they had a working fire based on their observations of heavy smoke coming from the rear of the building. The attack crew encountered heavy fire upon their initial entry into the rear apartments. A 1¾-inch attack line and a 1¾-inch backup line were utilized off the first due engine.
Recommendation #2: Fire departments should ensure that adequate fire control forces are on the scene and available for deployment for fire control activities. 2, 3, 4
Discussion: The initial response by the department included a total of 13 personnel on three engines, one ladder truck, and one command vehicle. NFPA states that "fewer than 11 fire fighters would be most hard pressed to accomplish safe, effective, initial interior fire attack in a timely manner at a detached single-family dwelling (low-hazard occupancy), not including an incident commander." The fire suppression equipment needed at a multifamily occupancy fire is outlined in the National Fire Protection Association (NFPA) Fire Protection Handbook. The NFPA suggests that, for this type of occupancy (medium-hazard occupancy), the staffing should be at least three pumpers, one ladder truck (or combination apparatus with equivalent capabilities), not fewer than 16 fire fighters and one chief officer, and other specialized apparatus as may be needed or available. Command and Control of Fires and Emergencies states that "some fire departments have officers participate in the hose stretch. This violates principles of safety and management. You cannot supervise an attack hose team if you are pulling hose, removing kinks from hose, chocking doors or directing nozzles in a fire room."
Recommendation#3: Fire departments should ensure that team continuity is maintained with two or more fire fighters per team. 1, 5, 6
Discussion: Each fire fighter must be assigned to a team of two or more and be given specific assignments to help reduce the chance of injuries. Team continuity relies on some very important key factors: knowing who is on your team and the team leader, staying within visual contact at all times (if visibility is obscured then teams should remain within touch or voice distance of each other), communicating your needs and observations to the team leader, rotating to rehab and staging as a team, and watching your team members (practice a strong "buddy-care" approach). These key factors help to reduce serious injury or even death resulting from the risks involved in fire fighting operations by providing personnel with the added safety net of fellow team members. The department’s standard operating procedures state that "fire fighters should always work in pairs and keep in constant contact, remembering that each is responsible for the other."
Recommendation #4: Fire departments should ensure that fire fighters notify their officer when they go above a fire. 7
Discussion: Even if the fire fighters’ assignment has been preplanned, the fire fighters’ officer should be informed, by portable radio or face-to-face communication, that they are going above the fire. This information is a form of fireground control that increases fire fighter safety. A company officer should know where all of his assigned fire fighters are operating during a fire. All fire fighters searching above a fire should understand the fire fighting priorities of risk-taking. Dunn [1992] states that "a fire fighter should not risk his life on the report of a missing person or even the high probability of a person trapped above a fire."
Recommendation #5: Fire departments should ensure that fire fighters, when operating on the floor above the fire, have a charged hoseline. 1, 7
Discussion: It is a good practice to get a hoseline on the floor immediately above the fire. Where there is risk of extension to concealed spaces and attics, additional precautionary lines are needed at each of these areas. Backup lines may also be needed in other areas above the fire. The department’s SOPs state that "when operating on the floor above the fire, have a charged hoseline ready. Hoselines can be used as life lines in addition to supplying an emergency fire fighting capability."
Recommendation #6: Fire departments should ensure that fire fighters manually activate their PASS device after radioing Mayday. 6
Discussion: When a fire fighter becomes lost or disoriented, a few simple steps can facilitate a quick rescue and reduce the chance of injury. The first step is the radio transmission of the Mayday situation, followed by the fire fighter providing the FAST and IC with clues as to his last known location. The fire fighter’s second step involves manually activating the PASS device. The final step requires the fire fighter to remain calm (conserving air), stay in radio contact with command and the FAST, and to survey the surroundings in an attempt to gain a bearing of direction or potential escape routes. It is important that if the fire fighter is not in immediate danger of fire impingement or collapse, that he remains in the safe area and moves as little as possible. This will conserve air and possibly help the FAST find the fire fighter more quickly than if the fire fighter were constantly moving. These steps should be incorporated into the department’s standard operating procedures with fire fighters trained on those procedures. Investigators were unable to determine, through interviews or equipment examination, whether the victim had manually activated his PASS device or the device had gone into alarm mode.
Recommendation #7: Fire departments should ensure that Incident Commanders size up the stretch of the first attack hose line. 4
Discussion: One of the most important size-up criteria is to assess the stretch of the fire attack hoseline. Kinks or bends in the hoseline, centrifugal pump failure, or a hose bursting from over-pressure can significantly hamper the fire fighting operation.
Recommendation #8: Fire departments should ensure that a fire fighter assist and search team (FAST) is established and in position. 8, 9
Discussion: A fire fighter assist and search team (FAST), commonly referred to as a rapid intervention team (RIT), should respond to every major fire. The team should report to the officer in command and should remain at an area designated by the IC until an intervention is required to rescue a fire fighter. The FAST should have all the tools necessary to complete the job–e.g., a search rope, rescue rope, first-aid kit, and a resuscitator to use in case a fire fighter needs assistance. These teams can intervene quickly to rescue fire fighters who become disoriented, lost in smoke-filled environments, trapped by fire, involved in structural collapse, or run out of breathing air. Many fire fighters who die from smoke inhalation or flashover, or who are caught or trapped by fire, actually become disoriented first. Fire fighters on the scene were designated as the FAST after the initial evacuation.
Recommendation #9: Fire departments should ensure that the Incident Commander is clearly identified as the only individual responsible for the overall coordination and direction of all activities at an incident. 10
Discussion: The Incident Commander (IC) shall be responsible for the overall coordination and direction of all activities at an incident. The incident management system shall clearly identify who is in overall command at the scene for the duration of the incident. The IC shall make assignments based on the availability, qualifications, and expertise of individuals. It is imperative that the IC clearly be in charge of all operations on the fireground to ensure the successful completion of an operation. This particular incident had an established IC, but some of the fireground operations were directed by the Director of the department and were not coordinated with those of the IC. An effective fireground operation revolves around one incident commander. If there is no command, or if there are multiple commands, fireground operations can quickly break down.
Recommendation #10: Fire departments should establish and enforce standard operating procedures on the use of thermal imaging cameras for search and rescue operations. 6
Discussion: Standard operating procedures (SOPs) provide specific information and instructions on how a task or assignment is to be accomplished. SOPs are established so that all members of a department will perform the same function with the same level of uniformity. These procedures are generally tactical in nature because in most instances they address emergency operations. At the time of the incident, the department did not have any SOPs regarding the use or application of thermal imaging cameras for search and rescue operations. Thermal imaging cameras were assigned to and present on Truck 1, Truck 2, Engine 2, and Engine 4. Thermal imaging cameras were not utilized during the primary search or the initial search for the victim.
Additionally, municipalities should consider
Recommendation #11: Establishing and maintaining multiple operating frequencies for emergency services, allowing portable radios at incidents to be equipped with two frequencies, one channel for tactical messages and one channel for command. 4
Discussion: If portable radios have one channel for tactical messages and a command channel can not be established, there is no way to manage radio transmission overload. The fire department involved in this incident has only one radio channel available to be used as the tactical and fireground channel. The department is currently operating on an 800 MHz system with three established channels; one for fire, one for police, and one as a shared channel for simultaneous incidents.
REFERENCES
INVESTIGATOR INFORMATION
This incident was investigated by Mark McFall, Kimberly Cortez, and Nancy Romano, Safety and Occupational Health Specialists, Division of Safety Research, NIOSH.
EXPERT REVIEW
Expert review was provided by Vincent Dunn, Deputy Chief (Ret.), FDNY.
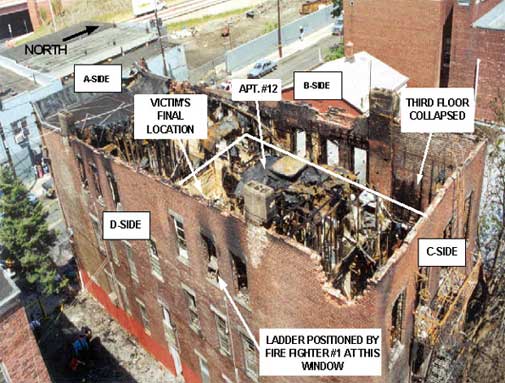
Photo. Site of Incident.
Diagram 1. Aerial View of Incident Scene.
Diagram 2. Aerial View of Apartment Where Victim Was Found.
APPENDIX A
NIOSH Reference: TN-12066
Phone: 304-285-5907
Fax: 304-285-6030
October 3, 2001
The National Institute for Occupational Safety and Health (NIOSH or the Institute) has concluded its investigation conducted under NIOSH Task Number TN-12066. This investigation consisted of the inspection and performance-testing of one self-contained breathing apparatus (SCBA) submitted by your office. The SCBA, sealed in a corrugated cardboard box, was delivered to the NIOSH Appalachian Laboratory for Occupational Safety and Health (ALOSH) on June 21, 2001. Upon arrival, the sealed package was taken to the Firefighter SCBA Evaluation Lab (Room 1520) and stored under lock until the time of the evaluation.
SCBA Inspections
I opened the package from your office and initiated the SCBA inspection on September 4, 2001, in Room 1520 of the ALOSH Building. I completed the inspection of the SCBA (referred to as Unit #1) on September 5, 2001. I examined the SCBA, component by component, in the condition as received to determine its conformance to the NIOSH-approved configuration. The entire inspection process was videotaped. I identified the SCBA as a Scott Air-Pak® 2.2.
The complete SCBA inspection is summarized in Appendix II of the enclosed SCBA Status Investigation Report. The condition of each major component was also photographed with a digital camera. Images of the SCBA are contained in Appendix IV of the enclosed report.
The most significant finding of the inspection was that the chin area of the facepiece assembly shows signs of exposure to extreme heat and flames. The faceseal has been partially consumed. (The damage to the faceseal can be seen in Figure 4 in Appendix IV of the enclosed report.) It should be noted that it is not known when the facepiece sustained the observed damage. It is possible that the damage to the facepiece assembly occurred after the firefighter succumbed to his injuries.
SCBA Testing
The purpose of the testing was to determine the SCBA’s conformance to the approval performance requirements of Title 42, Code of Federal Regulations, Part 84 (42 CFR 84). Further testing was conducted to provide an indication of the SCBA’s conformance to the National Fire Protection Association (NFPA) Air Flow Performance requirements of NFPA 1981 - Standard on Open-Circuit Self-Contained Breathing Apparatus for the Fire Service, 1997 Edition.
The following performance tests were conducted on the SCBA:
NIOSH SCBA Certification Tests (in accordance with the performance requirements of 42 CFR 84):
- Positive Pressure Test [42 CFR 84.70(a)(2)(ii)]
- Rated Service Time Test (duration) [42 CFR 84.95]
- Gas Flow Test [42 CFR 84.93]
- Exhalation Breathing Resistance Test [42 CFR 84.91(c)]
- Static Facepiece Pressure Test [42 CFR 84.91(d)]
- Remaining Service Life Indicator Test (low-air alarm) [42 CFR 84.83(f)]
National Fire Protection Association (NFPA) Tests (in accordance with NFPA 1981, 1997 Edition):
- Air Flow Performance Test [NFPA 1981, Chapter 6, 6-1]
Testing of the SCBA was initiated on September 6, 2001. I completed five performance tests that day. The first two performance tests listed above were conducted concurrently. During those tests, I observed air leaking between the damaged chin area of the Scott AV-2000 facepiece faceseal and the anthropometric head form. My repeated attempts at repositioning the facepiece and adjustment straps failed to achieve an adequate seal. Despite the observed air leak, I completed the Rated Service Time Test and the Positive Pressure Test with the damaged faceseal.
An inadequate facepiece seal could affect the SCBA’s ability to meet the performance requirements of some of the selected performance tests. Because the damage to the faceseal on Unit #1 prevented an adequate seal, a replacement AV-2000 facepiece assembly was obtained from NIOSH record material and was used during the remaining performance tests. It should be noted that the AV-2000 facepiece assembly contains no valves, diaphragms, or orifices that would affect the SCBA’s ability to meet the NIOSH performance requirements. Therefore, it would be expected that the results obtained during performance testing with the replacement AV-2000 facepiece would have been identical to the results obtained during performance testing with the damaged New Jersey facepiece assembly if an adequate seal had been achieved.
On September 7, 2001, I repeated the Rated Service Time Test and the Positive Pressure Test on the SCBA using the replacement facepiece. I also completed the NIOSH Exhalation Breathing Resistance Test and the NFPA Air Flow Performance Test that day.
SCBA Test Results
Due to the air leak observed during the initial run of the NIOSH Rated Service Time Test and the Positive Pressure Test, the SCBA failed to meet the requirements of the Rated Service Time Test. Once the damaged facepiece assembly was replaced with a new AV-2000 facepiece, the SCBA met the requirements of all six selected NIOSH tests performed. Additionally, the SCBA met the facepiece pressure requirements of the NFPA Air Flow Performance Test.
Appendix III of the enclosed report contains the complete NIOSH and NFPA test reports for the SCBA. Table One summarizes the NIOSH test results. Table Two summarizes the NFPA test results.
Personal Alert Safety System (PASS) Devices
A Personal Alert Safety System (PASS) device was clipped to the waist belt of the SCBA. During the SCBA inspection, I pressed the PASS unit’s manual activation switch. The PASS device did not function. I made no attempt to determine why the device failed to activate. Because NIOSH does not test or certify PASS devices, no further testing or evaluations were conducted on the PASS unit.
The Safety Equipment Institute (SEI) is the approval authority for PASS devices. For more information, you can contact Mr. Stephen R. Sanders, Technical Director with SEI, at (703) 442-5732.
Summary and Conclusions
On June 21, 2001, a package arrived at NIOSH from the Prosecutor’s Office. The sealed package was immediately taken to the Firefighter SCBA Evaluation Laboratory (room 1520) for secured storage. I broke the package seal on September 4, 2001. I found the package to contain one complete Scott Air-Pak 2.2, 30-minute, 2216 psi, SCBA (NIOSH approval number TC-13F-80). I initiated the SCBA inspection that day, and I completed the inspection on September 5, 2001.
The SCBA has the appearance of having seen considerable use. However, with the exception of the chin area of the facepiece faceseal, all components on the SCBA appeared to be fully functional. I determined that the SCBA was in a condition safe for testing.
I subjected the SCBA to a series of seven performance tests. I began testing the unit on September 6, 2001, and I completed testing on September 7, 2001. No maintenance or repair work was performed on the SCBA at any time. However, I observed air leaking between the damaged chin area of the facepiece faceseal and the anthropometric head form during the initial run of the Rated Service Time Test and the Positive Pressure Test. Therefore, in order to achieve an adequate seal during the remaining performance tests, a replacement AV-2000 facepiece assembly was obtained from NIOSH storage and used during the balance of the tests. During the initial run, the SCBA failed to meet the requirements of the Rated Service Time Test. Utilizing the replacement facepiece, the SCBA met the requirements of all six selected NIOSH tests performed, including the Rated Service Time Test. Additionally, the SCBA met the facepiece pressure requirements of the NFPA Air Flow Performance Test.
In light of the information obtained during this investigation, the Institute has proposed no further action at this time. Following inspection and testing, the SCBA was returned to the package in which it was shipped to NIOSH and stored under lock in Room 1520 pending return to the Prosecutor’s Office.
Recommendations
It is strongly recommended that the SCBA be inspected and serviced by an authorized Scott service technician and all necessary overhaul and repair work be completed before placing the unit back into service. It is also recommended that all SCBA inspection, handling, use, and maintenance procedures be reviewed with regard to activities and practices that could impact the safe use of all SCBA.
No further action will be taken by NIOSH and the investigation of Task Number TN-12066 will be considered closed. I trust this information is beneficial to your needs. If you have any questions or require additional information, please contact the Respirator Branch, National Personal Protective Technology Laboratory at (304) 285-6337.

Return to Fire Fighter Homepage
![]()
This page was last updated on 5/14/02