A Volunteer
Assistant Chief Was Seriously Injured and Two Volunteer Fire Fighters Were
Injured While Fighting a Townhouse Fire–Delaware
A Volunteer
Assistant Chief Was Seriously Injured and Two Volunteer Fire Fighters Were
Injured While Fighting a Townhouse Fire–Delaware
SUMMARY
On October 29, 2000, a 26-year-old male volunteer Assistant Chief (the victim) was seriously injured and two other fire fighters (Fire Fighter #1 and Fire Fighter #2) were injured while fighting a townhouse fire. The fire fighters responded to a call that had come in from Central Dispatch at 1909 hours as a reported chimney fire. Engine 9 was the first apparatus to arrive on the scene. The victim conducted a scene size-up and reported to Central Dispatch "smoke showing with fire extension to the roof" and that they were "in-service with a 1¾-inch hoseline." The victim then proceeded with a fire fighter (Fire Fighter #1) with 200 feet of charged 1¾-inch hoseline from Engine 9 into the townhouse’s front door and up the stairs toward the back bedroom. At 1923 hours, Engine 8 arrived on the scene, and the Captain assumed incident command (IC). The IC sent a fire fighter (Fire Fighter #2) from Engine 8 with a portable radio into the structure to provide assistance to the Assistant Chief (victim). Fire Fighter #2 followed the hoseline until he met up with the victim and Fire Fighter #1 at the top of the stairs (see Diagram 1). At 1927 hours, Engine S7 arrived on the scene. The Captain of Engine 8 transferred command to the Assistant Chief of Engine S7. Upon entering the back bedroom, the victim, who was on the nozzle, encountered and quickly knocked down a fire that was burning from floor to ceiling near the window in the back corner. The victim advanced the hoseline to the window to attack the fire on the outside of the building near the top of the chimney (see Diagram 1). While attacking the fire, the victim had Fire Fighter #2 search for fire extension above the bedroom ceiling. Using a Halligan tool, Fire Fighter #2 began pulling ceiling in the bedroom and encountered heavy, black smoke and an increase in heat. As the victim was leaning out of the window attacking the fire around the chimney, he noticed fire coming from the window directly below him. He shut down the nozzle and proceeded toward the bedroom door. Due to the deteriorating conditions of the interior, the IC called Central Dispatch and requested an emergency evacuation. The victim proceeded toward the top of the stairs where he encountered intensifying heat. He then yelled to Fire Fighter #1 and Fire Fighter #2 that they needed to get out. Fire Fighter #1 and Fire Fighter #2 dropped to their knees and followed the hoseline toward the bedroom door. As the victim began hearing the sirens and air horns (signaling an emergency evacuation) he turned and saw the other two fire fighters coming toward the top of the stairs. He then forced himself to descend the stairs through the intense heat. When he got to his feet, he believed he was standing outside the front door due to the cooler air temperatures, so he removed his helmet, facepiece, and hood. After taking a breath, he quickly realized that he was not at the front door but was still inside. He used his helmet to break the window and began climbing out (see Photo 1). A fire fighter and a police officer pulled him out of the window, and he was taken to an ambulance for medical treatment. The victim was transported to the regional level I trauma center before being life-flighted to the regional burn center. Fire Fighters #1 and #2 also encountered intense heat at the top of the stairs and could hear the sirens and air horns. Fire Fighters #1 and #2 forced themselves to descend the stairs through the intense heat. They were transported to the hospital and treated for their injuries.
NIOSH investigators concluded that, to minimize the risk of similar occurrences, fire departments should
ensure that the department’s Standard Operating Procedures (SOPs) are followed and refresher training is provided
ensure that fire fighting teams check each other’s personal protective equipment (PPE) for complete donning
ensure that a Rapid Intervention Team (RIT) stands by with equipment, ready to provide assistance or rescue
ensure that the Incident Commander conducts a complete size-up of the incident and continually evaluates the risk versus gain during operations at an incident
ensure that fire fighters report conditions and hazards encountered to their team leader or Incident Commander
ensure that team continuity is maintained
ensure that a separate Incident Safety Officer (ISO), independent from the Incident Commander, is appointed
ensure that the assignment of a tactical channel is established by Central Dispatch prior to personnel entering a hazardous environment
consider providing fire fighters with a Personal Alert Safety System (PASS) integrated into their Self-Contained Breathing Apparatus (SCBA)
ensure that ventilation is closely coordinated with the fire attack
Incident Site
INTRODUCTION
On October 29, 2000, a 26-year-old male volunteer Assistant Chief (the victim) was seriously injured while attempting to make an emergency evacuation from a townhouse fire. The victim was transported to the regional level I trauma center for immediate medical treatment. He was then life-flighted to the regional burn center where he was placed on a ventilator and hospitalized for 19 days. Two other fire fighters (Fire Fighters #1 and #2) were injured. Fire Fighter #1 received second-degree burns to his wrists while conducting fire suppression efforts and was transported to the regional hospital for treatment. Fire Fighter #2 received first-degree and second-degree burns to the wrist and ears while exiting the building.
The National Institute for Occupational Safety and Health (NIOSH) was notified of this incident by an official from the fire department in Delaware where the victim and Fire Fighters #1 and #2 are volunteer members.
On November 9, 2000, a Safety and Occupational Health Specialist from NIOSH’s Fire Fighter Fatality Investigation and Prevention Program investigated this incident at the request of the fire department involved. Meetings were conducted with the Chief of the department, a Senior Fire Investigator from the National Fire Protection Association (NFPA), the City Fire Marshal, and the investigator from the State Fire Marshal’s Office. Interviews were conducted with the officers and fire fighters involved in this incident. The NIOSH investigator obtained from the City and State Fire Marshal’s Offices copies of site maps and drawings, witness statements, copies of dispatch run sheets and tapes, and the report completed by the State Fire Marshal’s Office. A report completed by the NFPA Senior Fire Investigator was also obtained. Copies of the department’s standard operating procedures and the victim’s and injured fire fighters’ training records were obtained. The victim’s helmet, pants, coat, and hood were examined. The helmet’s ear flaps were up and turned to the inside of the crown. The chin strap was attached across the back of the helmet. The helmet had thermal damage across the front, top, and back. The back brim of the helmet was burned and broken halfway across, with the brim-support wire exposed around the rear of the helmet. Note: Damage to the helmet indicates that temperatures were in excess of 600E Celsius. The coat had no major or minor thermal damage to the front. The back of the coat had light thermal damage to the back of the sleeves and to the mid-height trim and the trim along the lower back. The loop material for the hook and loop fastener on the left side of the collar had some melting and would not fasten to the hook material on the other side of the collar. There was no thermal damage observed on the victim’s hood. The victim’s SCBA was sent to the NIOSH Respirator Branch in Morgantown, West Virginia, for testing (see Attachment). The purpose of the testing was to determine the SCBA’s conformance to the approval performance requirements of Title 42, Code of Federal Regulations (CFR), Part 84, Subpart H. Further testing was conducted to determine conformance to the National Fire Protection Association (NFPA) Air Flow Performance requirements of NFPA 1981, 1997 Edition. A series of tests utilizing a Biosystems PosiChek3 computerized SCBA performance tester were also conducted. The SCBA met the requirements of all six NIOSH SCBA certification tests performed. The SCBA also met the requirements of the NFPA Air Flow Performance Test and all tests performed using the Biosystems Posichek3.
A site visit was conducted and the site photographed. The site of the incident is a two-story wood frame townhouse with a walkout basement. The building construction is light-weight wood with wood trusses supporting each of the floor levels and the roof. The townhouse has vinyl siding on Sides 1 and 3. Masonry block separates each of the townhouse units. The State Fire Marshal’s Office has ruled that the fire was accidental and was the result of an unknown malfunction of the fireplace/chimney, which ignited nearby combustible materials. The fire occurred inside the enclosure of the chimney, allowing the fire to spread to the interior of the home.
The fire department involved in this incident consists of 3 stations with a total of 150 uniformed fire fighters. The department serves a population of 70,000 in a geographic area of 25 square miles. The department requires all new fire fighters to serve a 1-year probationary period and complete 66 hours of training in basic fire fighting, rescue, and EMS. The victim is a Certified NFPA Fire Fighter Level I and II, and NFPA Officer Level I, and has 6 years of volunteer fire fighting experience.
INVESTIGATION
On October 29, 2000, at 1909 hours, a call came into Central Dispatch reporting a chimney fire, and Stations 7, 8, and 9 were toned out. The units responding at 1914 hours included Engine 9 (Assistant Chief [the victim], Driver/Operator, and one fire fighter [Fire Fighter #1]), Engine S7 (Assistant Chief, Driver/Operator, and two fire fighters), and Ambulance 8 (two EMTs). At 1916 hours, Engine 8 (Captain, Driver/Operator, fire fighter, and Fire Fighter #2) responded to the incident. The Assistant Chief (the victim) on Engine 9 requested a ladder truck after a report came in from Central Dispatch of fire with extension to the roof. At 1919 hours, Central Dispatch reported that police were on the scene and reported a working fire. At 1920 hours, Ladder 21 (mutual aid) responded with an Assistant Chief, a Captain, a driver, and five fire fighters. At 1922 hours, Engine 9 arrived on the scene, and the victim reported to Central Dispatch that smoke was showing. After conducting a size-up of the scene, at 1923 hours, the victim reported to Central Dispatch "smoke showing with fire extension to the roof." He reported that they were "in-service with an 1¾-inch hoseline." As Engine 8 approached the scene, the Captain reported to Central Dispatch that they were laying in a line from a hydrant (see Diagram 2). The victim met with the resident of the townhouse to confirm that all of the occupants had exited and to get information on the layout of the townhouse. The victim then proceeded with a fire fighter (Fire Fighter #1) and 200 feet of charged 1¾-inch hoseline from Engine 9 into the townhouse’s front door and up the stairs toward the back bedroom (see Photo 1). At 1924 hours, Engine 8 arrived on the scene, and the Captain assumed incident command (IC). The IC sent a fire fighter (Fire Fighter #2) from Engine 8 with a portable radio into the structure to provide assistance to the Assistant Chief (the victim). The IC then requested the assignment of a Tactical Channel for this incident from Central Dispatch and was assigned Tactical Channel 5. Central Dispatch advised all units on Tactical Channel 3 (operations channel) to switch to Tactical Channel 5. Fire Fighter #2 followed the hoseline until he met up with the victim and Fire Fighter #1 at the top of the stairs (see Diagram 1). At 1924 hours, Engine S7 arrived on the scene. A second 1¾-inch hoseline was being stretched from Engine 9 to the front door of the townhouse. Fire fighters who were arriving on the scene at this time reported to the NIOSH investigator that light smoke was coming from the eaves and that the fire appeared to have been knocked down. The Captain of Engine 8 transferred command to the Assistant Chief of Engine S7. After assuming command, the Assistant Chief (IC) noticed that the conditions had quickly changed, and that a thick, black smoke was pushing out of the front door. At approximately 1925 hours, a police officer (a deputy fire chief) and a civilian (off-duty fire fighter) used an extension ladder to ventilate the second-story windows above the front door (see Photo 1). Note: The police officer and off-duty fire fighter assisted the driver of Engine 9 in laying the 5-inch supply line to the hydrant. The police officer and off-duty fire fighter then ventilated the second-story front windows using the tip of the extension ladder. They left the ladder positioned under the front bedroom window as a possible means of egress for the fire fighters inside.
Upon entering the back bedroom, the victim, who was on the nozzle, quickly knocked down a fire that was burning from floor to ceiling near the window in the back corner of the bedroom. The victim advanced the hoseline to the window and broke it out so that he could attack the fire on the outside of the building near the top of the chimney (see Diagram 1 and Photo 2). Two fire fighters from Engine S7 advanced the second hoseline into the townhouse as a backup for the first crew. The heavy, black smoke was almost to floor level, causing the crew on the second hoseline to miss the hoseline going up the stairs. The IC noted that heavy, black smoke was now pushing out of the front door as well as the two vented windows on the second floor. The IC then sent the police officer around to the back side (Side 3) of the building to check on the conditions. A ladder was pulled from Engine 8 and positioned for access to the roof for possible roof ventilation. The nozzle man and the fire fighter on the second hoseline proceeded down the hallway approximately 5 feet past the base of the stairs (see Diagram 1). Note: The fire fighter on the nozzle of the second hoseline did not realize that the attack crew had gone up the stairs. He believed that they were on the first level in front of him. The heavy, black smoke made it impossible for him to visually confirm the first crew’s location. While attacking the fire on the second level, the victim had Fire Fighter #2 search for fire extension above the bedroom ceiling. Using a Halligan tool, Fire Fighter #2 began pulling ceiling in the bedroom and encountered heavy black smoke and an increase in heat. On the first level, the fire fighter on the nozzle of the second hoseline heard a loud noise, sounding like a "bang," come from the area in front of him. Note: It is believed that the "bang" may have been drywall falling from the ceiling. He noticed that the heat banked down on top of him and was intensifying rapidly. The nozzle man, believing that the first crew was in front of him, held off from applying water. While the victim was leaning out of the second-story window attacking the fire around the chimney, he noticed fire coming from the window directly below him. He shut down the nozzle and proceeded toward the bedroom door. Fire Fighter #1 and Fire Fighter #2 grabbed the nozzle and began applying a straight stream into the attic space where they had removed the ceiling. At 1929 hours, Ladder 21 arrived on the scene. The victim proceeded toward the top of the stairs where he encountered intensifying heat. He yelled to Fire Fighter #1 and Fire Fighter #2 that they needed to get out. Fire Fighter #1 and Fire Fighter #2 dropped to their knees and followed the hoseline toward the bedroom door. At 1930 hours, the IC called Central Dispatch to request an emergency evacuation signal after he had received reports from fire fighters exiting the townhouse that the interior conditions were deteriorating. The IC then received a report from the police officer that there was heavy fire on Side 3. At the top of the stairs, the heat was intensifying, forcing the victim to get down on the floor. The carpet began melting and sticking to his bunker gear. Note: the victim reported to the NIOSH investigator that the heat made his neck, ears, and the sides of his face feel like they were on fire. The damage to the victim’s helmet (occurring at the top of the stairs) indicates that the temperature was in excess of 600E Celsius. As the victim began hearing the sirens and air horns (signaling an emergency evacuation) he turned and saw the other two fire fighters coming toward the top of the stairs. He then forced himself to descend the stairs through the intense heat. When he got to his feet, he believed he was standing outside the front door because the air around him felt much cooler. Note: In the NIOSH respirator investigation report on the victim’s SCBA, it was reported that the facepiece lens was considerably dirty, had several surface scratches on the lens hard coating, and the visibility through the lens was poor (see Attachment). The nozzle man on the second hoseline decided to apply a fog pattern to the back area of the townhouse. He wanted to knock down the heat in an attempt to reduce the potential for a flashover. When Fire Fighter #1 and Fire Fighter #2 reached the bedroom door, they encountered intense heat. Looking for another means of egress, they retreated to the window in the back corner of the bedroom. The window at this time was fully involved with fire, forcing them back toward the top of the stairs. Note: They heard the sirens and air horns signaling for an emergency evacuation at this time. The victim, who was now standing in the kitchen on the first floor, removed his helmet, facepiece, and hood. After taking a breath, he quickly realized that he wasn’t at the front door but was still inside the townhouse. He could see light coming through a window (kitchen window). He used his helmet to break the window and began climbing out (see Photo 1). The Captain from Engine 8 and a police officer pulled him out of the window. Fire Fighter #1 and Fire Fighter #2 now reached the top of the stairs and forced themselves to descend the stairs through the intense heat. Fire Fighter #2, followed by Fire Fighter #1, went down the stairs head-first on their stomachs. Their helmets were knocked off as they ran into the closet door at the base of the stairs and again when they fell over personnel on the second hoseline. Fire Fighter #2 was able to find his way out by first following the stream of water being applied to the stairs by a crew from Ladder 21 and then by assistance from personnel standing at the front door. The nozzle man and the fire fighter on the second hoseline had also felt the extreme heat and had begun exiting when they heard the sirens for the evacuation. The nozzle man was assisted out of the front door by the driver of Ambulance 8. Fire Fighter #1 had gone into the kitchen after falling over the crew on the second hoseline. He was then assisted out the front door by personnel from Ladder 21. The victim was taken to Ambulance 8 and provided medical treatment. He was then transported in Ambulance 8 to the regional trauma center for immediate medical treatment and then life-flighted to the regional burn center where he was hospitalized for 19 days. Fire Fighters #1 and #2 were both transported to the hospital for further treatment and release. Fire Fighter #1 was treated for second-degree burns to his wrists. Fire Fighter #2 was treated for first-degree and second-degree burns to his wrist and ears.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Fire departments should ensure that the department’s Standard Operating Procedures (SOPs) are followed and refresher training is provided.1-7
Discussion: It is imperative that companies perform their duties as described in the Standard Operating Procedures (SOPs) unless directed or approved by the incident command system to do otherwise. According to SOPs of the department involved in this incident, the following procedures should have taken place:
1. First-arriving units should use the radio to provide a description of the conditions found at the scene. This allows other responding units to anticipate what actions might be taken upon their arrival. When giving a report of conditions upon arrival, the following information should be included: (1) address, particularly if other than the one that was initially reported; (2) building and occupancy description; (3) nature and extent of fire; (4) attack mode selected; (5) rescue and exposure problems; (6) instructions to other responding units; (7) location of incident command position; and (8) establishing command. If the first-arriving unit officer elects to pass command of the incident, the officer is instructed by the department’s SOPs to voice the following information: (1) unit to assume command; (2) action and location of initial unit; and (3) assignments given to units already on the scene. The victim had reported to Central Dispatch that smoke was showing and that they were hitting a hydrant upon their arrival. After conducting the size-up of the incident scene, the victim reported to Central Dispatch that there was fire extension from the chimney and that they were going in service through the front door with a 1¾-inch hoseline to knock down the fire. The Captain from Engine 8 reported to Central Dispatch that he had assumed command. The Captain (IC) and other responding units were not aware of the number or location of personnel inside the townhouse or that the resident had reported to the victim that all of the occupants had exited the townhouse. The IC had sent Fire Fighter #2 into the structure to provide assistance to the attack crew because he was unaware of the number of personnel inside. When the backup crew entered the townhouse, they thought that the attack crew was on the same floor level as themselves.
2. The fire department’s Standard Operating Procedures (SOPs) state that "an accountability system is an integral component of fire fighter safety at an emergency incident that allows for the incident commander to track and account for personnel." The County Fire Chiefs Association adopted (prior to this incident) the Clemens Accountability System V (PAS-V) for use on all emergency incidents. The department’s SOPs state that "this system will enhance the safety of fire fighters operating on emergency incidents by providing the incident commander with a system of tracking the number of personnel and the area of their operation on incidents. This information is vital in the event that an evacuation is ordered or an event occurs that requires accounting for all personnel on the incident site." The system components consist of (1) PAS-V accountability tag, (2) apparatus collector ring and tag, (3) accountability board, and (4) an accountability binder. The SOPs have established three levels (I-III) of accountability. Level I has been implemented with personnel placing their accountability tags on the apparatus ring/tag in the corresponding riding position. At the time of the incident, Levels II and III were not implemented. Levels II and III are in the process of being adopted. Level II includes the accountability board procedures, procedures for passing and transfer of command, and procedures for sector officers. Level III includes the procedures for entry control.
Recommendation #2: Fire departments should ensure that fire fighting teams check each other’s personal protective equipment (PPE) for complete donning.8
Discussion: The key to proper and effective use of PPE is the development of good habits that include fast, proper, and complete donning of the appropriate PPE ensemble. Fire fighting teams should check each others’ PPE to help ensure that the equipment is fully and completely donned. This team check will help prevent burn or injury. To minimize the risk of burn injuries to the head region, it is important to ensure that the hood is donned correctly to provide maximum protection for the ears, neck, and face (not protected by the SCBA face mask). Care must be taken to ensure that the hood does not interfere with the facepiece-to-face seal. Collars must be turned up to protect the wearer’s neck and throat (the front of the collar must be fastened to protect the throat area). The ear flaps on the helmet must be pulled down to protect the back of the neck and the ears. The chin strap on the helmet must be fastened around the chin without obstructing the SCBA’s regulator hose to ensure that helmets stay in place upon impact.
Recommendation #3: Fire departments should ensure that a Rapid Intervention Team (RIT) stands by with equipment, ready to provide assistance or rescue.3,4,5
Discussion: A Rapid Intervention Team (RIT) should respond to every working structure fire. The team should report to the officer in command and remain at the staging area until an intervention is required to rescue a fire fighter. The Rapid Intervention Team should have all the tools necessary to complete the job–e.g., a search rope, rescue rope, first-aid kit, and a resuscitator to use in case a fire fighter needs assistance. These teams can intervene quickly to rescue fire fighters who become disoriented, lost in smoke-filled environments, trapped by fire, involved in structural collapse, or run out of air. National Fire Protection Association (NFPA) 1500: Standard on Fire Department Occupational Safety and Health, section 6-4.4 states that, "In the initial stages of an incident where only one team is operating in the hazardous area at a working structural fire, a minimum of four individuals is required, consisting of two individuals working as a team in the hazard area and two individuals present outside this hazard area for assistance or rescue at emergency operations where entry into the danger area is required. The standby members shall be responsible for maintaining a constant awareness of the number and identity of members operating in the hazardous area, their location and function, and time of entry. The standby members shall remain in radio, visual, voice, or signal line communications with the team."
Recommendation #4: Fire departments should ensure that the Incident Commander conducts a complete size-up of the incident and continually evaluates the risk versus gain during operations at an incident.6,7
Discussion: The initial size-up conducted by the first-arriving officer who assumes command allows the officer to make an assessment of the conditions, allowing his decisions to be proactive as opposed to reactive. The following general factors are important considerations during a size-up: occupancy type involved, smoke conditions, type of construction, age of structure, exposures, and time considerations such as time of incident, time fire was burning before arrival, time fire was burning after arrival, and type of attack. The Captain’s (the IC from Engine 8 ) initial size-up involved all available information received prior to his arrival and what he saw upon his arrival on the scene (the west and south sides of the structure). A view of the north side (Side 3) of the structure may have revealed fire extension to the family room located below the floor the attack crew was working on.
Recommendation #5: Fire departments should ensure that fire fighters report conditions and hazards encountered to their team leader or Incident Commander.8
Discussion: Individual fire fighters should keep their team leader (a senior fire fighter or officer) advised of conditions and hazards they find as work is performed. The team leader can relay conditions and hazards encountered by their crew to the Incident Commander (IC) by portable radio or face-to-face. This information would allow the IC to continuously evaluate the risks and benefits of tasks being performed on the fireground.
Recommendation #6: Fire departments should ensure that team continuity is maintained.1,8
Discussion: Each fire fighter should be assigned to a team of two or more and given specific assignments to help reduce the chance of injuries. Team continuity relies on some very important key factors: knowing who is on your team and the team leader, staying within visual contact at all times (if visibility is obscured then teams should remain within touch or voice distance of each other), communicating your needs and observations to the team leader, rotation to rehab and staging as a team, and watching your team members (practice a strong "buddy-care" approach). These key factors help to reduce serious injury or even death resulting from the risks involved in fire fighting operations by providing personnel with the added safety net of fellow team members.
Recommendation #7: Fire departments should ensure that a separate Incident Safety Officer (ISO), independent from the Incident Commander, is appointed.3,4,9,10
Discussion: According to NFPA 1561, paragraph 4-1.1, "The Incident Commander (IC) shall be responsible for the overall coordination and direction of all activities at an incident. This shall include overall responsibility for the safety and health of all personnel and for other persons operating within the incident management system. While the IC is in overall command at the scene, certain functions must be delegated to ensure adequate scene management is accomplished." According to NFPA 1500, paragraph 6-1.3, "As incidents escalate in size and complexity, the IC shall divide the incident into tactical-level management units and assign an ISO to assess the incident scene for hazards or potential hazards." The most effective ISOs are those who operate as a consultant to the IC. The ISO establishes a relationship with the IC by asking what the action plan is, followed by a summary of the current situation status and resource status. With this information, the ISO can collect more information in the form of a reconnaissance or 360-degree size-up of the incident. With this additional information, the ISO can report concerns and possible solutions to the IC. During this incident, the IC was also acting as the Safety Officer and thus was limited in being able to perform the additional functions of a separate ISO.
Recommendation #8: Fire departments should ensure that the assignment of a tactical channel is established by Central Dispatch prior to personnel entering a hazardous environment.1
Discussion: The radio communications system should reflect the size and complexity of the incident. Often, when one radio channel is primarily used for dispatching, it is necessary to operate on a different channel for an incident. Tactical channels are most often used for larger incidents such as structure fires. When units in this county are initially dispatched, they operate on the county-wide operations channel (Tactical Channel 3). Upon arrival on the scene, the units switch to a tactical channel that has been assigned to them by Central Dispatch when it is determined to be a working incident. Having a fireground channel assigned prior to personnel entering a structure would increase the likelihood that all personnel would hear the assignment of the tactical channel, allowing them to set their portable radios to the desired channel. Tactical channels can be assigned either while the units are en route to the scene and the fire confirmed to be a working fire by police officers, or when the initial size-up is reported by the first-arriving unit. Noisy environments, such as encountered inside a burning structure, make it difficult for fire fighters to hear radio traffic, and the protective equipment (heavy gloves) can make it difficult to switch channels, especially in low-visibility situations like the one encountered by the victim and Fire Fighters #1 and #2. These environmental factors (heat, noise, and low visibility) and the equipment worn by fire fighters while working in hazardous environments necessitate personnel to have their portable radios turned on and set to the channel that has been established by Central Dispatch or the IC.
Recommendation #9: Fire departments should consider providing fire fighters with a Personal Alert Safety System (PASS) integrated into their Self-Contained Breathing Apparatus (SCBA).
Discussion: PASS devices that are integrated into the fire fighters’ SCBAs would activate when the fire fighters turn on their air supply. The victim had a manually activated PASS device, which apparently was not activated. The victim’s PASS device was found on the kitchen floor the following day. The fire department had purchased some integrated PASS devices prior to the incident and is in the process of purchasing additional integrated PASS devices. Where fire departments utilize manually operated PASS devices, fire fighters should be trained and routinely reminded to activate their PASS devices when operating on the fireground. Activation of manually operated PASS devices should be enforced to assist with search-and-rescue operations on the fireground if required.
Recommendation #10: Fire departments should ensure that ventilation is closely coordinated with the fire attack.1, 11
Discussion: Chapter 10 of the Essentials of fire fighting, 4th edition, states that, "ventilation must be closely coordinated with fire attack. When a ventilation opening is made in the upper portion of a building, a chimney effect (drawing air currents from throughout the building in the direction of the opening) occurs." Ventilation is necessary to improve a fire environment so that fire fighters can approach a fire with a hoseline for extinguishment. However, window and door ventilation should be coordinated with fire extinguishment. Only after a charged hoseline is in place and ready for extinguishment is ventilation of windows and doors most effective. Command should determine if ventilation is needed and where ventilation is needed. The type of ventilation should also be determined, based on evaluation of the structure and conditions on arrival.
REFERENCES
1. IFSTA [1998]. Essentials of fire fighting. 4th ed. Stillwater, OK: International Fire Service Training Association.
2. Delaware fire department’s Standard Operating Procedures (SOPs) [2000].
3. NFPA [1997]. NFPA 1500: standard on fire department occupational safety and health program. Quincy, MA: National Fire Protection Association.
4. NFPA [1995]. NFPA 1561, standard on fire department incident management system. Quincy, MA: National Fire Protection Association.
5. Dodson DW [1999]. Fire department: incident safety officer. New York: Delmar Publishers.
6. Dunn V [1992]. Safety and survival on the fireground. Saddle Brook, NJ: Fire Engineering Books & Videos.
7. Brunacini AV [1985]. Fire command. Quincy, MA: National Fire Protection Association.
8. Fire Fighter’s Handbook [2000]. Essentials of fire fighting and emergency response. New York: Delmar Publishers.
9. Smoke CH [1999]. Company officer. New York: Delmar Publishers.
10. NFPA [1997]. NFPA 1521, standard for fire department safety officer. Quincy, MA: National Fire Protection Association.
11. Collapse of Burning Buildings, Vincent Dunn, Publisher Penn Well, 1988.
INVESTIGATOR INFORMATION
This incident was investigated by Mark McFall, Safety and Occupational Health Specialist, Division of Safety Research, NIOSH.
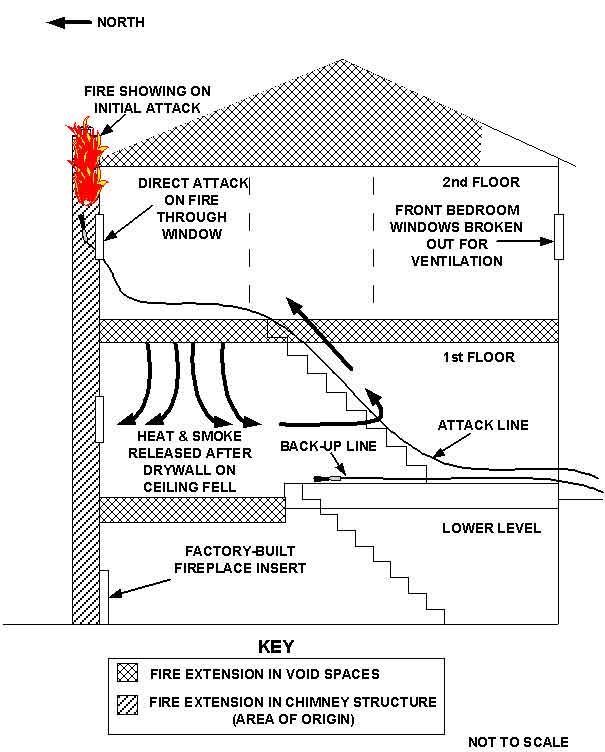
Diagram 1. Diagram depicting the cross-sectional view of the townhouse apartment, showing the fireplace insert on the lower level, the path of the heat and smoke after the ceiling drywall fell on the first floor, the windows used by the fire fighters on the second floor, and the paths of the attack line and the back-up line.
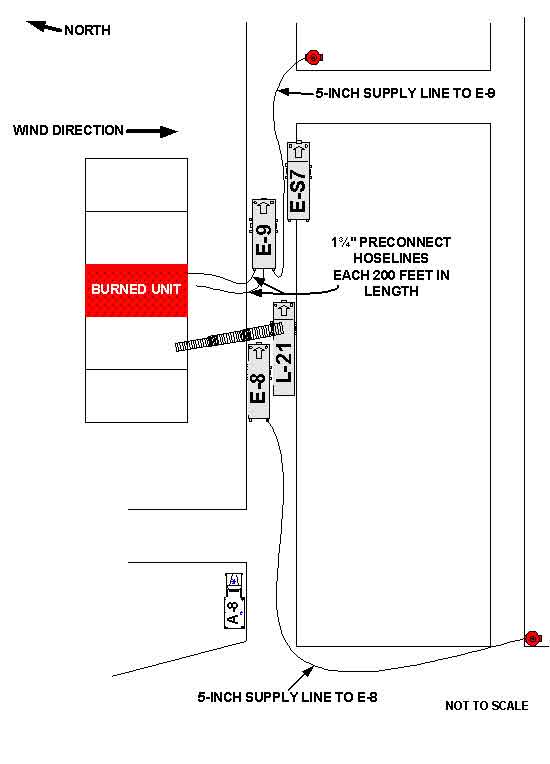
Diagram 2. Aerial View of Incident Site, showing the apparatus involved and the layout of the hoselines.
Photo 1. View of Side 1, showing the point of entry and exit, the window through
which
the victim was removed, and the windows ventilated using the extension ladder.
Photo 2. View of Side 2, showing the fire extension into the truss void space, the outline of the
chimney framing, the fire extension into the truss void space, and the back bedroom window.
The following is a summary of NIOSH Task No. TN-11790. For a full report contact NIOSH, Division of Respiratory Disease Studies, Respirator Branch at (304) 285-5907.
NIOSH Reference: TN-11790
December 21, 2000
The National Institute for Occupational Safety and Health (NIOSH or the Institute) has concluded its investigation conducted under NIOSH Task Number TN-11790. This investigation consisted of the inspection and performance-testing of one self-contained breathing apparatus (SCBA) received by NIOSH from the Delaware fire department on November 27, 2000. The primary purpose of this investigation was to determine the SCBA’s conformance to the NIOSH certification requirements of Title 42, Code of Federal Regulations, Part 84 (42 CFR 84). Six selected performance tests were conducted in accordance with these NIOSH approval requirements. In order to provide you with additional information about the SCBA’s performance, the National Fire Protection Association (NFPA) Air Flow Performance test, was also conducted. The NFPA Air Flow Performance test was conducted in accordance with NFPA 1981, Standard on Open-Circuit Self-Contained Breathing Apparatus for the Fire Service - 1997 Edition. Our inspection report and results of all tests are contained in a detailed Status Investigation Report which is enclosed.
Inspection of the SCBA shipped to NIOSH by the Delaware fire department was initiated on November 28, 2000, and was completed on November 29, 2000. During the inspection, the NIOSH approval label was found to be intact and readable. The label indicates that the SCBA is a Scott® Aviation 4.5, 30-minute, 4500 psi, SCBA (NIOSH approval number TC-13F-76). The SCBA is in fairly good condition but has the appearance of having seen extensive use. The facepiece lens is considerably dirty. Several surface scratches were observed on the lens hard coating. The visibility through the lens is poor. A key ring was found attached to the SCBA head harness. This ring is not a part of the NIOSH-approved configuration. However, this unapproved change to the configuration would not be expected to have any effect on the SCBA performance.
The SCBA was thoroughly inspected and determined to be in a condition safe for testing. Because no compressed air cylinder was shipped with the SCBA, an appropriate Scott® compressed air cylinder was obtained from NIOSH record material and was used during the performance testing. Performance testing was initiated and completed on November 29, 2000. The SCBA met the requirements of all of the six NIOSH performance tests conducted. The SCBA also met the requirements of the NFPA Air Flow Performance Test. The complete SCBA test report with results of all performance testing conducted on the SCBA is presented in Attachment Three of the enclosed report.
It is strongly recommended that this SCBA be inspected and serviced by an authorized Scott® service technician and all necessary overhaul and repair work be completed before placing the unit back into service. It is also recommended that all SCBA inspection, handling, use, and maintenance procedures be reviewed with regard to activities and practices that could impact the safe use of all SCBA.
No further action will be taken by NIOSH and the investigation of Task Number TN-11790 will be considered closed. The SCBA will be stored under lock in room H-178A of the NIOSH Appalachian Laboratory for Occupational Safety and Health (ALOSH) pending return to your office.
Quality Assurance Team
Respirator Branch
Division of Respiratory Disease Studies

Return to Fire Fighter Homepage
![]()
This page was last updated on 11/21/05