Residential Structure Fire Claims the Life of One Career Fire Fighter–Alabama
Residential Structure Fire Claims the Life of One Career Fire Fighter–Alabama
SUMMARY
On April 20, 2000, a 33-year-old male career fire fighter was fatally injured while battling a residential structure fire. At approximately 1630 hours, Central Dispatch was notified of a reported structure fire at a single family residence. At 1631 hours, Central Dispatch notified the local fire department of the reported structure fire. Car 12 (captain/incident commander [IC]), Engine 1 (lieutenant, engine operator, and fire fighter [FF#1]), Engine 2 (lieutenant, fire fighter [FF#2], and engine operator/fire fighter [victim]), Rescue 52 (two fire fighter/paramedics [FF#3 and FF#4]), Car 14 (air supply van, two fire fighters [FF#5 and FF#6]), and Rescue 50 (two fire fighter/paramedics [FF#7 and FF#8]) responded to the scene. At 1633 hours, a captain arrived on the scene and established incident command (IC). He conducted a scene size-up, including a walk-around of the structure, and confirmed to Central Dispatch that there was a working structure fire with thick black smoke emitting from the garage/basement. As Engine 1 was approaching the scene, the IC instructed the crew to stop and connect to the hydrant. Rescue 52 met up with Engine 1 at the hydrant and assisted them in making the connection. Engine 1 connected their supply line to the hydrant and proceeded to the scene as Rescue 52 finished making the hydrant connection. The IC radioed that the fire was in the garage/basement. Rescue 52 arrived on the scene. The lieutenant from Engine 1 instructed FF#1 to pull a 1¾-inch handline off of Engine 1 and proceed with him into the garage/basement of the structure. At approximately the same time, FF#5 and FF#6 arrived on the scene in Car 14 (air supply van). They reported to the IC and were instructed to pull a 1¾-inch handline and enter through the front door of the structure with the victim. They walked into the structure and immediately dropped to their knees due to heat and lack of visibility. They made their way into the structure, moving to their left approximately 10 feet. The victim was on the nozzle and FF#5 and FF#6 served as backup. Heavy smoke made it impossible to see, so they exited the structure to get a positive pressure fan (PPV) to aid in ventilation. As they exited, FF#4 was setting up the fan at the front door of the structure. The victim and FF#5 and FF#6 reentered the structure through the front door and made their way to the right and into the living room. FF#5, FF#6, and the victim were near the bathroom of the residence when FF#6 heard a loud crack. It is believed that at this time the victim fell through the bathroom floor into the basement. The engine operator from Engine 1 went into the basement bedroom, entering from the garage through the utility room into the downstairs bedroom. The engine operator from Engine 1, with the help of FF#1 and FF#4, removed the victim from the structure. The victim was flown by an emergency-transport helicopter to a regional trauma center where he was pronounced dead.
NIOSH investigators concluded that to minimize the risk of similar occurrences, fire departments should
ensure that fire fighters performing fire fighting operations under or above trusses are evacuated as soon as it is determined that the trusses are exposed to fire
ensure that a rapid intervention team is established and in position upon arrival
ensure that fireground communication is present through both the use of portable radios and face-to-face communications
ensure that exterior fire attack is at a minimum during search and rescue
ensure fire fighters are trained to recognize the danger of searching above a fire
Although there is no evidence that it contributed to this fatal event, the following recommendation is being provided as a reminder of good safety policy.
ensure consistent use of personal alert safety system (PASS) devices at all incidents and consider providing fire fighters with a PASS integrated into their self-contained breathing apparatus
Incident Scene
INTRODUCTION
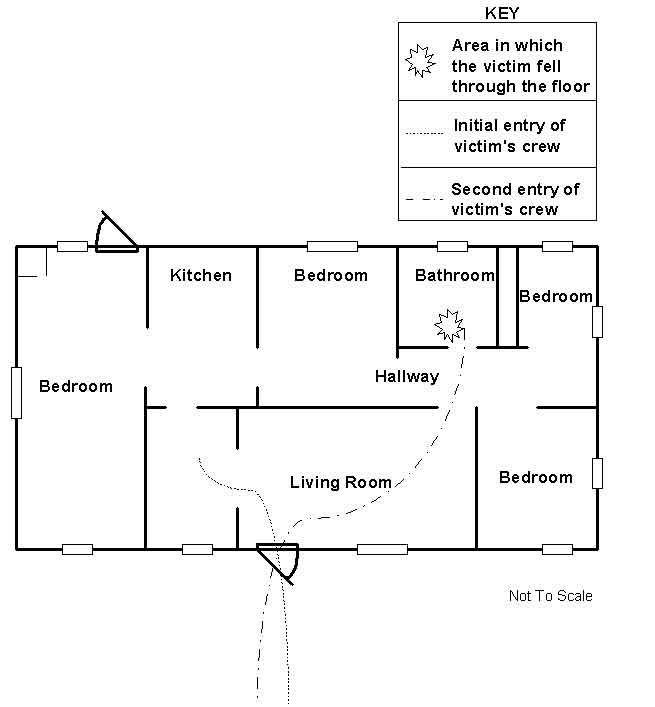
On April 20, 2000, a career fire department responded to a residential structural fire at a local residence. The victim was part of an interior attack crew who was killed when he fell through the upstairs floor while trying to locate the fire. The fire originated in the basement wiring directly under the section of the floor that collapsed (Figure 1). On April 21, 2000, the United States Fire Administration (USFA) notified the National Institute for Occupational Safety and Health (NIOSH) of this incident. On June 5-7, 2000, two safety and occupational health specialists from the Division of Safety Research, Fire Fighter Fatality Investigation and Prevention Program investigated this incident. Interviews and meetings were conducted with the chief of the department, fire fighters who were on the scene of this incident, a representative from the International Association of Fire Fighters (IAFF), and the State Fire Marshal. The incident site was visited and photographs of the fire scene were reviewed. Copies of witness statements, training records, standard operating procedures (SOPs), the death certificate, and a map of the fire scene were reviewed. An inspection of the victim’s self-contained breathing apparatus (SCBA) was conducted by the NIOSH, Division of Respiratory Disease Studies, Respirator Branch (see Attachment).
This career department consists of 85 uniformed fire fighters. The department serves a population of 60,000 in an area of 60 square miles. The structure involved in this incident was a one-story wood frame house, with a one car garage and a partial basement under the living area.
The State of Alabama requires all fire fighters to be NFPA Level I certified. The victim was certified at the NFPA Fire Fighter Level I and II. Additionally, the victim had the following certifications: Driver Operator, EMT, Haz-Mat, Apparatus Operation, First Aid, CPR, Rope Rescue, and Public Safety Telecomm. At the time of the incident, the victim was wearing a full array of personal protective clothing and equipment, consisting of turnout gear (coat and pants), helmet, gloves, boots, Nomex® hood and a self-contained breathing apparatus (SCBA) with a manual personal alerting safety system (PASS) device. The victim had 8 years of experience.
INVESTIGATION
On April 20, 2000, at approximately 1630 hours, Central Dispatch was notified of a reported structure fire. At 1631 hours, Central Dispatch notified the fire department, and the following units were dispatched to the scene:
Car 12–captain/incident commander (IC)
Engine 1–lieutenant, engine operator, and fire fighter (FF#1)
Engine 2–lieutenant, fire fighter (FF#2), and engine operator/fire fighter (the victim)
Rescue 52–two fire fighter/paramedics (FF#3 and FF#4)
Car 14 (Air Supply Van)–two fire fighters (FF#5 and FF#6)
Rescue 50–two fire fighter/paramedics (FF#7 and FF#8)
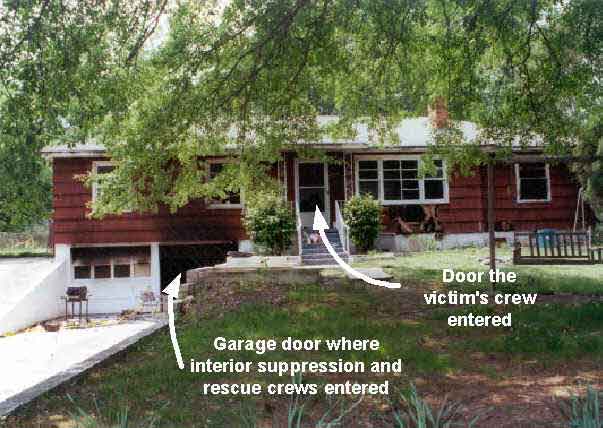
At 1633 hours, the Captain arrived on the scene and established incident command (IC). He conducted a scene size-up, including a walk-around of the structure, and confirmed to Central Dispatch that there was a working structure fire with thick, black smoke emitting from the garage/basement area (Photo 1). As Engine 1 was approaching the scene, the IC instructed the crew to stop and connect to the hydrant. Rescue 52 met up with Engine 1 at the hydrant and assisted them in making the connection. Engine 1 connected their supply line to the hydrant and proceeded to the scene as Rescue 52 finished making the hydrant connection.
Engine 2 arrived on the scene with a lieutenant, the engine operator/fire fighter (victim), and FF#2. The lieutenant from Engine 1 approached the IC to determine the location of the fire. The IC stated that the fire was in the basement. Rescue 52 (FF#3 and FF#4) arrived on the scene. The lieutenant from Engine 1 instructed FF#1 to pull a 1¾-inch handline off of Engine 1 and proceed with him into the structure through the garage/basement door (Figure 1).
At approximately the same time, FF#5 and FF#6 arrived on the scene in Car 14 (air supply van). They reported to the IC and were instructed to pull a 1¾-inch handline and enter through the front door of the structure, along with the victim. FF#5, FF#6, and the victim pulled the handline into the structure and immediately dropped to their knees because of heat and lack of visibility. They made their way into the structure, moving to their left, for approximately 10 feet. The victim was on the nozzle and FF#5 and FF#6 served as backup. Due to poor visibility, they exited the structure to get a positive pressure fan (PPV) to aid in ventilation. As they exited, FF#4 was already setting up the fan at the front door of the structure. The victim (nozzleman) and FF#5 and FF#6 reentered the structure, with a 1¾-inch handline, through the front door, made their way to the right, and continued into the structure to the bathroom area (Figure 1). FF#3 proceeded into the garage/basement of the structure, entering through the garage door, and made his way into the basement about 10 feet and met up with the lieutenant from Engine 1 and FF#1. Note: At this point, there was zero visibility in the garage/basement. The lieutenant from Engine 1 and FF#1 and FF#3 attacked the fire with a 1¾-inch handline, but were forced to exit due to the extreme heat. After exiting the structure, FF#3 went to the rear of the structure to check for fire extension and for a better path to attack the fire.
The lieutenant from Engine 1 and FF#1 reentered the garage/basement area to attack the fire for a second time. They again were forced to exit due to extreme heat. The lieutenant from Engine 2 placed a PPV fan in front of the garage door, then went into the basement with FF#1 to continue suppression activities. They opened the nozzle to suppress the fire, and the heat and steam that was created forced them to drop to the floor. FF#3 reentered the garage and met up with the lieutenant from Engine 2 and FF#1. The lieutenant from Engine 1 proceeded to the rear of the structure and noticed an opening approximately in the middle of the foundation wall, covered by plywood. He cleared the opening and saw "blowtorch-like" fire conditions coming from the opening. The lieutenant from Engine 1 then went to the front of the structure (garage area) and retrieved a 1¾-inch handline. He and FF#1 proceeded to the rear of the structure with the handline to hit the fire through the opening in the foundation at the rear of the structure. FF#5, FF#6, and the victim continued their search for the fire inside the structure. At this time FF#6 heard a loud crack, and saw the victim had fallen through the bathroom floor into the basement area. FF#5 and FF#6 crawled to the area where the victim fell through the floor and saw flames in the basement. They dropped to their stomachs to distribute their weight on the floor and yelled to the victim to protect himself from the fire by opening his nozzle and hitting the flames. They reached into the opening of the floor, grabbed the victim’s hands, and tried unsuccessfully to pull the victim back up to them.
The lieutenant from Engine 2 and FF#3 were continuing suppression activities in the garage and made it approximately 5 feet through the doorway leading into the downstairs utility room. As they entered the doorway, they saw the glow from the fire. FF#3’s low-air alarm was sounding and he was forced to exit. The IC made his way to the rear of the structure to assess the conditions. At this time FF#3, with a fresh bottle, was instructed by the lieutenant from Engine 1 to enter the front door and meet up with the crew from Rescue 52. He made his way into the structure approximately 6 feet and noticed that the floor felt spongy. The lieutenant from Engine 1 and FF#1 and FF#4 opened the nozzle and sprayed water into the opening in the rear (vent) of the structure for approximately 1 minute when they heard someone yelling from the upstairs of the structure. They shut the handline down so they could hear who was yelling and what was being said. They heard the interior crew yell "man down" and "get a scuttle-hole ladder." FF#3 then exited the structure to get the scuttle-hole ladder to assist in the removal of the victim. After several attempts by FF#5 and FF#6 to pull the victim up through the hole, FF#6 exited the structure to inform the IC of the situation and retrieve a scuttle-hole ladder to aid in removal of the victim from the basement. FF#5 stayed inside the structure to try to aid in the removal of the victim. FF#6 was met at the front door by FF#3 with the scuttle-hole ladder. FF#3 and FF#6 took the ladder into the structure. After several attempts to place the ladder, FF#5, FF#6, and FF#3 exited the structure to find a better way to reach the victim. Note: The ladder was very hard to maneuver and set into place due to the confined area of the hallway of the structure. The IC instructed FF#3 to switch duties with the engine operator from Engine 1. The IC then pulled a 2½-inch hoseline off of Engine 1 and instructed FF#5 to go to the basement with the engine operator from Engine 1 to aid in suppression and search efforts. FF#6 reentered the structure through the garage door, took the 2½-inch line from FF#5, and sprayed water as long as he could before exiting. Note: FF#6 did not have an air pack on at this time. FF#5 went in to assist in rescue operations because he knew the general area where the victim could be located. FF#5 crawled into the basement bedroom entering from the garage through the utility room into the downstairs bedroom. The engine operator from Engine 1 made his way into the structure, crawling on his knees, following FF#5 and a handline. The engine operator from Engine 1 heard FF#5 yell that he found the victim. The engine operator went to FF#5 and, with the help of FF#1 and FF#4, removed the victim from the structure. The victim was flown by emergency-transport helicopter to a regional trauma center where he was pronounced dead.
CAUSE OF DEATH
According to the medical examiner’s report, the cause of death is listed as thermal injuries (full-thickness burns to roughly one-third of body surface area).
RECOMMENDATIONS/DISCUSSION
Recommendation # 1: Fire departments should ensure that fire fighters performing fire fighting operations under or above trusses are evacuated as soon as it is determined that the trusses are exposed to fire.1
There is no specific time limit on how long fire fighters should operate under or on truss systems that are exposed to fire. A time limit is often used by fire departments as a guide for operation under or on truss systems. Even though standard fire-engineering calculations show that lightweight trusses may be expected to collapse after about 10 minutes in a fully developed fire, it is not recommended to set a time limit. As stated in Building Construction For the Fire Service,1 "under fire conditions, truss failure is unpredictable." When fire fighters arrive on the scene of a building with trusses exposed to fire, it is virtually impossible to identify how long the trusses have been exposed to fire and consequently set a time limit for fire suppression. When it is determined that the building’s trusses have been exposed to fire, any fire fighters operating under or above them should be immediately evacuated. If it is not clear that the building’s trusses have been exposed to fire, a defensive attack should take place until the conditions can be verified.
Fire fighters may have difficulty finding the exact location of fire in a building, even though heavy smoke makes it clear that fire is present. The fire could be in a void or concealed area. For example, a floor truss can span great lengths with no breaks or fire stops, creating a void space that can conceal the fire, allowing it to grow rapidly. The term "fire-rated" should not be misinterpreted. It does not provide any fire resistance, but merely meets fire code requirements for rate of flame spread. The design of floor trusses provides a void to hide the fire and allow carbon monoxide to accumulate. If the floor truss would collapse while fire fighters were under or on them, the fire fighters could become trapped inside the structure. In this incident the floor trusses were exposed to fire, causing the structural members to weaken.
Recommendation #2: Fire departments should ensure that a rapid intervention team is established and in position upon arrival.2
A rapid intervention team (RIT) should respond to every major fire. The team should report to the officer in command and remain at the command post until an intervention is required to rescue a fire fighter(s) or civilians. The RIT should have all tools necessary to complete the job (e.g., a search rope, first-aid kit, and a resuscitator) to use if a fire fighter becomes injured. Many fire fighters who die from smoke inhalation, from a flashover, or from being caught or trapped by fire actually become disoriented first. They are lost in smoke and their SCBAs run out of air, or they cannot find their way out through the smoke, become trapped, and then fire or smoke kills them. The primary contributing factor, however, is disorientation. The RIT will be ordered by the IC to complete any emergency searches or rescues. They will provide the suppression companies the opportunity to regroup and take a roll call instead of performing rescue operations. When the RIT enters to perform a search and rescue, they should have full cylinders on their SCBAs and be physically prepared. When a RIT team is used in an emergency situation, an additional RIT team should be put into place in case an additional emergency situation arises. This additional RIT team should be comprised of fresh, well-rested fire fighters.
Recommendation #3: Fire departments should ensure that fireground communication is present through both the use of portable radios and face-to-face communications.3,4
During the course of the fireground operations, the IC must be heard and also must hear everyone on the scene. All members should follow radio communications guidelines, keeping transmissions short, specific, and clear. However, these areas cannot be completed if electronic problems occur, or not all fire fighters are equipped with portable communication equipment. Therefore, fire departments should implement a backup communications plan to avoid a communication breakdown on the fireground. The plan should include backup electronic equipment, additional channels, training, and consideration of face-to-face communications, or the utilization of runners to communicate an important message if radio communication fails.
Recommendation #4 : Fire departments should ensure that exterior fire attack is at a minimum during search and rescue.5
Once search and rescue operations are in place, fire departments should ensure that the fire fighters completing the search and rescue are not placed in danger by the fire attack. It is a complicated procedure to determine the position of the fire fighters completing search and rescue operations in the interior, from an exterior position. If an exterior fire attack is being performed while the interior search and rescue operations are taking place, there is a possibility that the fire could shift and place the interior fire fighters conducting search and rescue operations in an unsafe position. Additionally, the use of an exterior hoseline to direct water through a window could possibly cause a collapse, placing the interior fire fighters in a dangerous position. Command and operations must be in communication at all times on the fireground to ensure coordination of tactics.
Recommendation #5: Fire Departments should ensure fire fighters are trained to recognize the danger of searching above a fire.6
The danger of being trapped above a fire is greatly influenced by the construction of the burning building. Of the five basic building construction types–fire resistive, noncombustible, ordinary construction, heavy timber, and wood frame–the greatest danger to a fire fighter who must search above the fire is posed by wood frame construction. Vertical fire spread is more rapid in this type of structure. Flames may spread vertically and trap fire fighters searching above the fire in four ways: up the interior stairs, windows (autoexposure), concealed spaces, and flame spread up the combustible exterior siding.
Although there is no evidence that it contributed to this fatal event, the following recommendation is being provided as a reminder of good safety policy.
Recommendation #6: Fire departments should ensure consistent use of personal alert safety system (PASS) devices at all incidents and consider providing fire fighters with a PASS integrated into their self-contained breathing apparatus.
PASS devices are electronic devices worn by the fire fighter, which will emit a loud and distinctive alarm if the fire fighter becomes motionless for more than 30 seconds. Fire fighters entering hazardous areas should be equipped with a PASS device. There are several types of PASS devices available. One device that could be used is a PASS that is integrated into the SCBA. PASS devices integrated into the SCBA will be activated when the SCBA air cylinder is turned on. Manual PASS devices are also used throughout the fire service. These devices require the fire fighter to manually turn on the device each time they use it.
REFERENCES
1. Brannigan FL [1999]. Building construction for the fire service. Quincy, MA: National Fire Protection Association.
2. National Fire Protection Association [1997]. NFPA 1500, standard on fire department occupational safety and health program. Quincy, MA: National Fire Protection Association.
3. Dunn V [1998]. Collapse of burning buildings, a guide to fireground safety. Saddle brook, NJ: Fire Engineering Books and Videos.
4. NFPA [1995]. NFPA 1561, Standard on fire department incident management system. Quincy, MA: National Fire Protection Agency.
5. Coleman J [1997]. Incident management for the street-smart fire officer. Saddle Brook, NJ: Fire Engineering MA: National Fire Protection Association.
6. Dunn V [1992]. Safety and survival on the fireground. Saddle Brook, NJ: Fire Engineering Books and Videos.
INVESTIGATOR INFORMATION
This investigation was completed by, Thomas P. Mezzanotte and Kimberly L. Cortez, Safety and Occupational Health Specialists, Division of Safety Research, Surveillance and Field Investigations Branch.
Photo 1. Points of Entry of Fireground Personnel for Fire Suppression and Rescue Crews
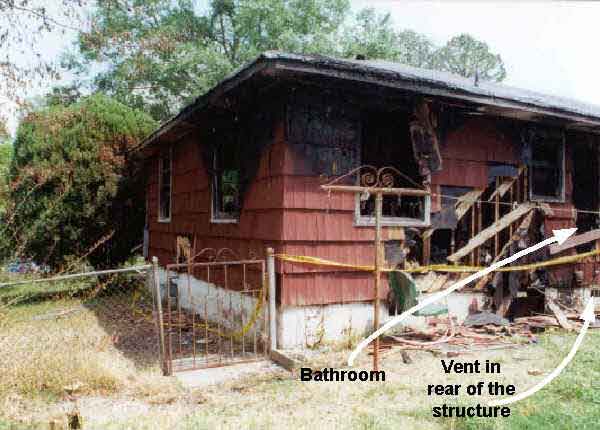
Photo 2. Rear of the Structure, Bathroom Area
Figure 1. Aerial View of First Floor
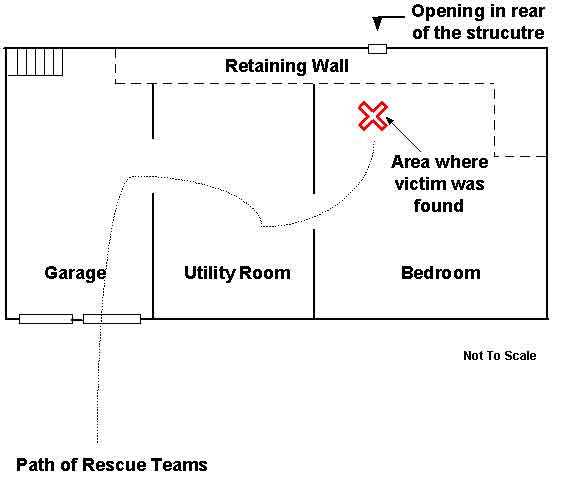
Figure 2. Aerial View of Basement
The following is a summary of NIOSH Task No. TN-11541. For a full report, including attachments, photos, and tables, contact NIOSH, Division of Respiratory Disease Studies, Respirator Branch at (304) 285-5907.
NIOSH Reference: TN-11541
Centers for Disease Control and Prevention (CDC)
National Institute for Occupational Safety and Health - ALOSH
1095 Willowdale Road
Morgantown, WV 26505-2888
John S. Robison,
State Fire Marshal
State of Alabama
Department of Insurance
201 Monroe Street, Suite 1780
P. O. Box 303352
Montgomery, Alabama 36130-3352
Dear Sir:
The National Institute for Occupational Safety and Health (NIOSH) has concluded its investigation conducted under NIOSH Task Number TN-11541. This investigation consisted of the inspection and performance-testing of one self-contained breathing apparatus (SCBA) shipped to NIOSH by your office on May 25, 2000. The primary purpose of this investigation was to determine the SCBA’s conformance to the NIOSH certification requirements of Title 42, Code of Federal Regulations, Part 84 (42 CFR 84). Six selected performance tests were conducted in accordance with these NIOSH approval requirements. In order to provide you with additional information about the SCBA’s performance, the National Fire Protection Association (NFPA) Air Flow Performance test, was also conducted. The NFPA Air Flow Performance test was conducted in accordance with NFPA 1981, Standard on Open-Circuit Self-Contained Breathing Apparatus for the Fire Service - 1997 Edition. Our inspection report and results of all tests are contained in a detailed Status Investigation Report which is enclosed.
Inspection of the SCBA shipped to NIOSH by the Alabama State Fire Marshal was completed on July 31, 2000. The NIOSH approval label is damaged but readable. The label indicates that the SCBA is a Mine Safety Appliances (MSA) Ultralite II, 30-minute, 2216 psi, SCBA (NIOSH approval number TC-13F-138). The SCBA is worn and has the appearance of having seen considerable use. The facepiece lens is considerably dirty. The visibility through the lens is very poor.
The compressed air cylinder shipped with the SCBA is a Survivair 2216 psi cylinder. It is important to note that the NIOSH regulations listed in Subpart D of Title 42, Code of Federal Regulations (CFR), Part 84, Section 84.30 (a) and (b) state:
(a) The Institute shall issue certificates of approval pursuant to the provision of this subpart only for individual, completely assembled respirators which have been examined, inspected, and tested, and which meet the minimum requirements set forth on subparts H through L of this part, as applicable.
(b) The Institute will not issue certificates of approval for any respirator component or for any respirator subassembly.
While the Survivair cylinder shipped with the MSA SCBA is approved for use on several SCBA with certificates of approval held by Survivair, this cylinder is not a part of any of MSA’s NIOSH-approved configurations. Therefore, the MSA SCBA with the Survivair cylinder attached, is not considered to be a NIOSH-approved SCBA configuration.
The SCBA was thoroughly inspected and determined to be in a condition safe for testing. The Survivair cylinder from the Center Point Fire Department was used during the performance testing even though the use of a Survivair cylinder on an MSA SCBA represents an unapproved configuration. Performance testing was initiated on August 1, 2000, and was completed on August 2, 2000. The SCBA met the requirements of five of the six NIOSH performance tests conducted. The SCBA failed to meet the requirements of the NFPA Air Flow Performance Test. The complete SCBA test report with results of all performance testing conducted on the SCBA is presented in Attachment Three of the enclosed report.
While the SCBA was tested with the cylinder shipped with the unit, this is not meant to condone the use of a Survivair cylinder with an MSA SCBA. In fact, this SCBA configuration is not approved by NIOSH.
During the Static Facepiece Pressure test, the facepiece pressure was found to be slightly higher than the NIOSH limitation. Excessive static facepiece pressure could potentially shorten the duration time of the SCBA air supply due to air leakage through the facepiece exhalation valve. However, this SCBA met the requirements of the Rated Service Time Test. While the unit failed to maintain positive pressure during the NFPA Air Flow Performance Test, the possibility of inward leakage into a firefighter’s facepiece would be dependant upon the face to facepiece seal, the ventilation rate at the time of use, as well as other factors such as age, weight, and the physical condition of the firefighter. Test results indicate that air was flowing to the facepiece in a sufficient quantity to meet the NIOSH requirements. It should be noted that the SCBA facepiece pressure remained positive throughout the NIOSH Rated Service Time Test. It is also important to note that the SCBA was evaluated in the "as received" condition. The condition of the SCBA prior to the incident cannot be determined.
It is strongly recommended that this SCBA be inspected and serviced by an authorized MSA service technician, all necessary overhaul and repair work be completed, and the SCBA returned to a NIOSH-approved configuration by incorporating a proper MSA compressed air cylinder before placing the unit back into service. It is also recommended that all SCBA inspection, handling, use, and maintenance procedures be reviewed with regard to activities and practices that could impact the safe use of all SCBA.
No further action will be taken by NIOSH and the investigation of Task Number TN-11541 will be considered closed. The SCBA will be stored under lock in room H-178A of the NIOSH Appalachian Laboratory for Occupational Safety and Health (ALOSH) pending return to your office.
I trust this information is satisfactory to meet your needs. If you require further assistance, please contact me at (304) 285-6337.
Sincerely yours,
Thomas W. McDowell,
Physical Scientist
Quality Assurance Team
Respirator Branch
Division of Respiratory Disease Studies

Return to Fire Fighter Homepage
![]()
This page was last updated on 10/15/01