Restaurant Fire
Claims the Life of Two Career Fire Fighters - Texas
Restaurant Fire
Claims the Life of Two Career Fire Fighters - Texas
SUMMARY
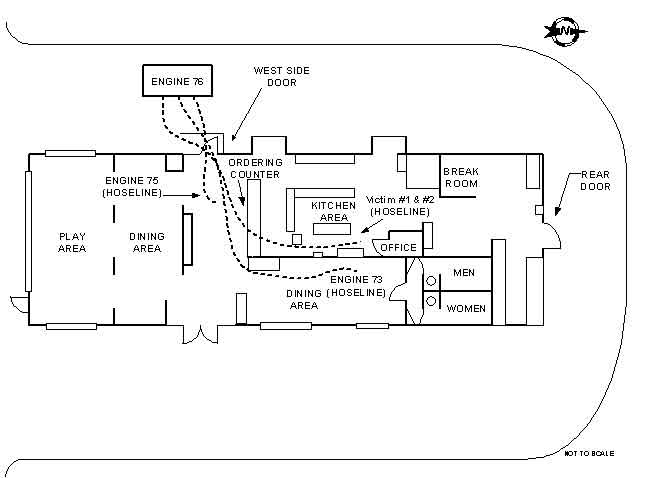
On February 14, 2000, a 44-year-old male and a 30-year-old female, both career fire fighters, died in a restaurant fire. At 0430 hours, Central Dispatch received a call from a civilian who reported that fire was emitting through the roof of the restaurant. Medic 73 was first to arrive on the scene, followed by Engine 76 (Captain, Fire Apparatus Operator (FAO), and two fire fighters (Victim #1 and Victim #2). Upon arrival, dispatch was notified by the two companies that there was visible fire emitting through the roof. The Captain on Engine 76 radioed dispatch reporting that he and his crew were going to complete a "fast attack" (enter the structure with a 1¾-inch hoseline and knock down the fire with the water from their engine). Approximately 2 minutes later, Ladder 76 (Captain, FAO, and one fire fighter) arrived on the scene and the Captain assumed Incident Command (IC). After making forcible entry, the victims entered with a 1¾-inch hoseline as their Captain finished donning his gear. Shortly after, the Captain entered the structure, met up with his crew, and then exited the structure to assist with the advancement of their hoseline. Engine 73 (Captain, FAO, and two fire fighters) arrived on the scene and one fire fighter entered the structure with a 1¾-inch hoseline. He stretched the hoseline past the front counter and around a wall in the dining area (see Diagram 2). The Captain from Engine 76 reentered the structure and followed a hoseline, which he believed the victims were on. After meeting up with a fire fighter on the end of the line, the Captain exited and reentered the structure a second time. As he followed the line, debris began to fall and there was visible fire throughout the middle section of the kitchen (see Diagram 1). Soon after, District 10 (District Chief) arrived, completed a size-up, and assumed command. Due to the heavy fire he observed, he requested all companies convert to a defensive attack and evacuate the structure. At this point the middle roof section (over the kitchen) of the building had collapsed. An interior evacuation took place, and neither of the victims exited. The IC sent several fire fighters inside to search for the victims. The fire fighters located and removed Victim #1 at 0530 hours. He was then transported to a local hospital where he was pronounced dead. The fire fighters located Victim #2 at 0713 hours, and she was pronounced dead at the scene. The scene was then turned over to the City Fire and Arson Bureau, which declared the incident to be a crime scene due to arson.
NIOSH investigators concluded that, to minimize the risk of similar incidents, fire departments should
ensure that the department’s Standard Operating Procedures (SOPs) are followed
ensure that fire command always maintains close accountability for all personnel at the fire scene
ensure that Incident Command conducts an initial size-up of the incident before initiating fire fighting efforts and continually evaluates the risk versus gain during operations at an incident
ensure that vertical ventilation takes place to release any heat, smoke, and fire
ensure that fire fighters are trained to identify truss roof systems
ensure that fire fighters use extreme caution when operating on or under a lightweight truss roof and should develop standard operating procedures for buildings constructed with lightweight roof trusses
ensure that fire fighters performing fire fighting operations under or above trusses are evacuated as soon as it is determined that the trusses are exposed to fire
explore using a thermal imaging camera as a part of the exterior size-up
ensure that, whenever there is a change in personnel, all personnel are briefed and understand the procedures and operations required for that shift, station, or duty
ensure that, whenever a building is known to be on fire and is occupied, all exits are forced and blocked open
consider providing all fire fighters with portable radios or radios integrated into their face pieces
consider adding additional staff in accordance with NFPA standards
establish various written standard operating procedures, ensure record keeping, and conduct annual evaluations to monitor and evaluate the effectiveness of their overall SCBA maintenance program.
Additionally, building owners, utility providers, and municipalities should
ensure that all exterior building utilities are accessible and in working condition
consider placing the building’s construction information on an exterior placard
upgrade or modify older structures to incorporate new codes and standards to improve occupancy and fire fighter safety
Photograph by R. Harris.
Restaurant Fire in This Incident
INTRODUCTION
On February 14, 2000, two fire fighters died while performing an interior fire attack at a restaurant fire. Both victims were using a 1¾-inch hoseline inside the building when the roof collapsed. When the victims failed to exit upon the IC’s interior evacuation call, the IC ordered additional fire fighters to enter the building and search for the victims. Victim #1 was located, removed from the building, and transported to a nearby hospital where he was pronounced dead. Victim #2 was later located and pronounced dead at the scene.
On February 14, 2000, the U.S. Fire Administration notified the National Institute for Occupational Safety and Health (NIOSH) of this incident. On March 6, 2000, three Safety and Occupational Health Specialists from the NIOSH Fire Fighter Fatality Investigation and Prevention Program, as well as an Engineer and a Physical Scientist from the NIOSH Respirator Branch, investigated this incident.
Meetings and interviews were conducted with the Chief, Assistant Chiefs, District Chiefs, Safety Officers, fire fighters who were at the scene, the department’s training officer, a representative from the District Attorney’s Office, a representative from the City Special Crimes and Arson Unit, representatives of the City Fire and Arson Bureau, the county Fire Marshal, and representatives of the International Association of Fire Fighters. Investigators visited the site, and the Engineer and Physical Scientist from NIOSH conducted an evaluation of the department’s respirator maintenance program. Investigators also examined the victims’ SCBAs and the turnout gear that they were wearing during the incident. The SCBAs were severely damaged by fire and further testing could not be conducted. However, no problems were noted in the past with either of the SCBA units. Investigators obtained a copy of the department’s Standard Operating Procedures (SOPs), training manual, both victims’ training records, autopsy reports, photographs of the incident, video footage of the incident, fire department interview statements, dispatch tapes, a transcription of the dispatch tapes, and blueprints of the building. The investigators conducted a site visit at a nearby restaurant which was similar to the one involved in the incident.
On March 22, 2000, two Safety and Occupational Health Specialists conducted additional interviews. On September 12-13, a Safety and Occupational Health Specialist from the NIOSH Fire Fighter Fatality Investigation and Prevention Program and an Engineer with the National Institute of Standards and Technology (NIST) conducted additional interviews with fire department personnel to assist in the development of a fire dynamics model for this incident (see section titled FIRE MODEL INFORMATION). On September 14-15, a Safety and Occupational Health Specialist from the NIOSH Fire Fighter Fatality Investigation and Prevention Program conducted additional interviews with fire department personnel and met with a representative from the City Code and Enforcement Department.
The career fire department involved in this incident is comprised of 3,800 total employees, of whom 3,400 are uniformed fire fighters. The department serves a population of approximately 1.8 million in a geographical area of 617 square miles. The department requires all new fire fighters to complete 31 weeks of training at the department’s fire academy. The training consists of 640 hours toward fire fighter Level I and II certification, weight training, a physical fitness test, and 240 hours of emergency medical technician (EMT) courses. All fire fighters are required to complete the State EMT and fire certification examination. Fire fighters are then assigned to a station where they are placed on a 12-month probationary period. There are four levels of certification for fire fighters to achieve. The first level is basic. Once fire fighters graduate from the academy and complete their probationary period they are certified as a basic fire fighter. The second level is intermediate, which requires 4 years of service and 6 semester hours of Fire Science or 96 hours of completed courses at the National Fire Academy. The third level is advanced, requiring fire fighters to have 8 years of service and 6 additional hours of Fire Science or 96 hours of completed courses at the National Fire Academy. The fourth level is master, and it requires fire fighters to have 12 years of service, and 60 semester hours which include 18 semester hours of Fire Science or an associate’s degree in Fire/Science Technology. Both victims’ training records were reviewed and appeared to be sufficient. Victim #1 was listed as a master level fire fighter with 18½ years of fire fighting experience. Victim #2 was listed as an intermediate level fire fighter with 5½ years of experience as a fire fighter. Victim #2 had met all of the certification items at the advanced fire fighter level except for the time in service.
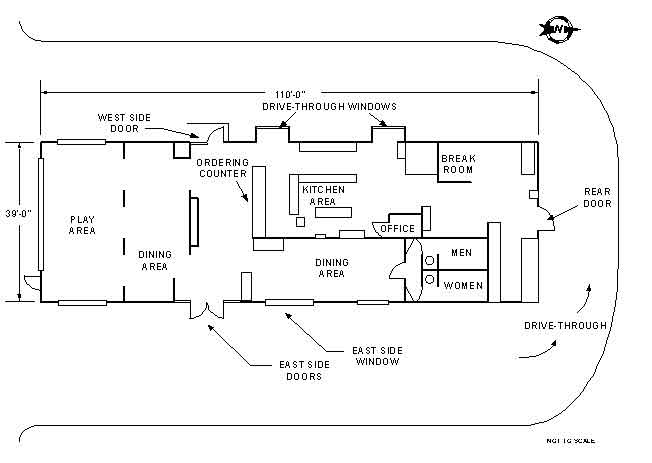
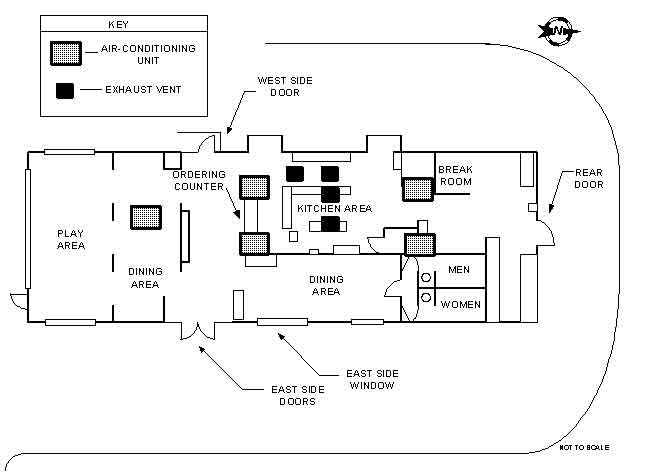
The building involved in this incident served as a restaurant, measuring 110 feet by 39 feet. The structure was one story, formed on a concrete slab foundation. The wall systems consisted of ½-inch drywall, 2- by 4-inch wall studs, 3½-inch insulation, ½-inch low density combustible fiber board, and exterior masonry brick. The roof system was formed using lightweight wood trusses, consisting of 2- by 4-inch and 2- by 6-inch lumber connected with metal gusset plates (see Photo 1). The total span of the trusses over the majority of the structure was 47 feet 6½ inches. There were no interior load-bearing walls noted. The trusses were placed 2 feet on center with 2- by 8-inch lateral bracing. The exterior roof system consisted of 5/8-inch plywood sheathing with fiberglass asphalt built-up roofing. A false roof (parapet) was built around the entire roof section of the building. There were a total of five HVAC units located on the roof (three 10-ton units and two 5-ton units). There were a total of four exhaust vents located on the roof above the kitchen area (see Diagram 3 and Photo 2). The interior ceiling of the building was suspended 1 foot from the trusses, using suspended ceiling panels. According to the city codes, the building was classified as a Group B-3 structure. The Group B-3 code is incorporated in the city’s 1972 Building Codes, Chapter 7, Section 701 - Requirements for Group B Occupancies, Division 3. This code applies to all occupancies with an occupant load of less than 300 people. In 1986, the city adopted the nationally recognized Uniform Building Code and this building was reclassified as a Group A building. This code is incorporated in the 1986 Uniform Building Code, Section 303 - Requirements for Group A Occupancies, Division 3. This code reads the same as the 1972 Building Codes, Chapter 7, Section 701 - Requirements for Group B Occupancies, Division 3. The city is currently using the 1997 Uniform Building Code. This building was not equipped with a sprinkler system and, according to the codes listed above, a sprinkler system was not required. Additionally, the City Code and Enforcement Department did not have any previous violations listed for this building.
The City Fire and Arson Bureau declared the cause of this incident as arson. The origin of the fire was determined to be in the office, which extended into the void space above the suspended ceiling.
Additional companies responded to this incident; however, only those directly involved are included in this report.
FIRE MODEL INFORMATION
Upon a request from NIOSH, the National Institute of Standards and Technology (NIST) completed a fire model of this incident. The fire model demonstrates fire growth and the fire’s reaction when different variables are inputted. The complete fire model will be available for viewing online Spring 2001 at www.fire.nist.gov.
INVESTIGATION
On February 14, 2000, at 0430 hours, Central Dispatch received a call reporting that a restaurant was on fire. At 0433 hours, dispatch toned out a first alarm which consisted of the following:
• District 10 (District Chief)
• District 69 (District Chief)
• Engine 76 (Captain, FAO, Victim #1 and #2)
• Engine 75 (Captain, FAO, two fire fighters)
• Engine 73 (Captain, FAO, two fire fighters)
• Engine 10 (Captain, FAO, two fire fighters)
• Ladder 76 (Captain, FAO, one fire fighter)
• Ladder 75 (Captain, FAO, one fire fighter)
• Medic 73 (FAO, one fire fighter/paramedic)
• Safety 15 (Captain)
• 1102 (EMS Senior Supervisor)
• 1184 (Emergency Medical Service [EMS] Supervisor)
The second-alarm companies were dispatched at 0502 hours and consisted of the following:
• Engine 39 (Captain, FAO, two fire fighters)
• Engine 82 (Captain, FAO, two fire fighters)
• Engine 69 (Captain, FAO, two fire fighters)
• Engine 60 (Captain, FAO, one fire fighter)
• Engine 68 (Captain, FAO, two fire fighters)
• Ladder 68 (Captain, FAO, one fire fighter)
• Ladder 69 (Captain, FAO, one fire fighter)
• Rescue 11 (Captain, FAO, two fire fighters)
• Rehab 17 (Operator)
• District 82 (District Chief)
• District 28 (District Chief)
• Safety 2 (Senior Captain)
• Medic 60 (FAO, paramedic)
• Medic 68 (FAO, paramedic)
• Ambulance 82 (two Emergency Medical Technicians [EMTs])
• Ambulance 69 (two Emergency Medical Technicians [EMTs])
The third-alarm companies were dispatched at 0527 hours and consisted of the following:
• District 2 (District Chief)
• Engine 51 (Captain, FAO, two fire fighters)
• Engine 57 (Captain, FAO, two fire fighters)
• Engine 48 (Captain, FAO, two fire fighters)
• Engine 78 (Captain, FAO, one fire fighter)
• Ladder 78 (Captain, FAO, two fire fighters)
• Ladder 28 (Captain, FAO, two fire fighters)
• Ladder 51 (Captain, FAO, two fire fighters)
• Communications Van (Operator)
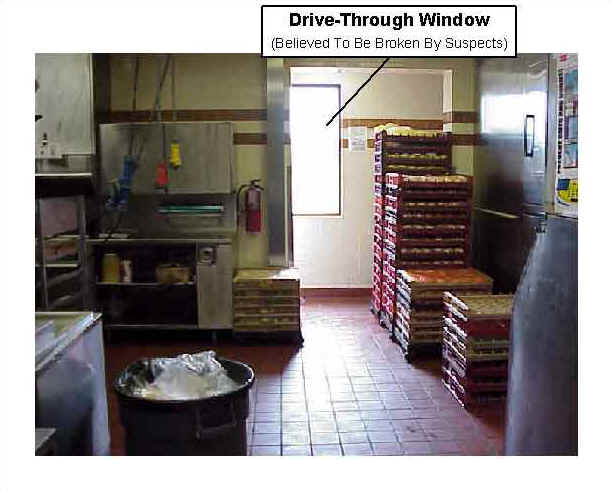
At 0438 hours, Medic 73 was the first to arrive on the scene and reported to dispatch that they had visible fire emitting through the roof (approximately 6-foot flames). Note: Based on information obtained from the City Fire and Arson Bureau, the fire started in the office area approximately 25 minutes prior to Medic 73’s arrival (see Photo 3). Investigators with the City Fire and Arson Bureau had confirmed this to be the point of origin, based on the scene evidence. Additionally, it was reported that one of the suspects broke out the first drive-through window (closet to the north side wall), which provided a direct path of air flow to the office (see Photo 4). All companies that responded to the incident stated that it was very foggy and hard to see, which caused a delay in their response. Approximately 1 minute later, Engine 76 arrived on the east side of the scene and reported the same size-up to dispatch as Medic 73. Engine 76 drove around to the rear of the building (to complete their size-up) and continued to the west side where they parked the apparatus. The Captain from Engine 76 stated the fire was extending from the middle section of the roof approximately 6 feet in the air, possibly venting from one of the exhaust vents, which gave the appearance of a grease fire (see Photo 5). The Captain reported to dispatch that he and his crew (himself, Victim #1, and Victim #2) would be making a "fast attack" (enter the structure with a 1¾-inch hoseline and knock down the fire using the water from their engine). He then radioed Ladder 76 asking them to make forcible entry when they arrived because the building was secured. At 0440 hours, Ladder 76 arrived on the scene and the Captain assumed Incident Command (IC). The IC radioed Engine 73 and ordered them to connect to a plug (fire hydrant) on the south side of the building and lay a supply line to Engine 76 when they arrived. Victim #1 and Victim #2, equipped with a 1¾-inch hoseline, entered the structure as their Captain donned his equipment. The FAO and fire fighter from Ladder 76 went to the west side to prepare entry as requested and stated that entry was already made by removing the bottom panel of the glass-sectioned door (see Photo 6 and Photo 7). Note: It is believed that the victims had made entry after Ladder 76 was requested. Soon after, the Captain from Engine 76 entered the building and stated that it was filled with thick, black smoke which had banked down to the floor. He also stated that there was very little heat and no visible fire. It is believed that the majority of the fire was between the suspended ceiling and the roof and could not be seen from the interior. The Captain met up with Victim #2 approximately 10 feet inside, in front of the ordering counter (see Diagram 1). It is believed that Victim #1 was on the opposite side of the counter (kitchen area) at this time. Victim #2 stated that they were having trouble advancing the hoseline and told the Captain they needed someone to feed them the line. The Captain exited the building to feed his crew additional hoseline.
The IC directed one of the fire fighters from Ladder 76 to set up a positive pressure ventilation (PPV) fan outside the west side door to help clear the smoke from the building. The fire fighter from Ladder 76 retrieved a PPV fan from their ladder truck and placed it approximately 12 feet behind the railing of the west door. The fire fighter stated that the fan was started and set in the highest operating speed. Note: Based on the NIST fire model it was concluded that the PPV fan was not a significant factor to the fire’s growth. As the PPV fan was being set up, the other fire fighter from Ladder 76 vented the other drive-through window, closest to the west side door (see Diagram 1 and Photo 7). The two fire fighters from Ladder 76 then returned to the east side and made forcible entry through the exterior doors and placed lights inside the doors (see Photo 8). One of the fire fighters from Ladder 76 then proceeded back to the rear of the west side and attempted to shut off the gas. However, the attempt was unsuccessful because the gas shut-off valve was stripped. At 0442 hours, Engine 73 arrived on the scene and connected to a plug on the south side across the street from the building. After laying a supply line to Engine 76 the Captain and his two fire fighters from Engine 73 approached the building on the west side. As the Captain from Engine 76 fed additional line to the victims, a fire fighter from Engine 73 pulled another 1¾-inch hoseline off Engine 76 and entered the structure through the west side door to back up the two victims. He assumed that his Captain and the other fire fighter would be right behind him. Instead, the Captain from Engine 73 ordered the other fire fighter to pull a 1¾-inch hoseline off Engine 76 and meet him at the west side door. He was equipped with a thermal imaging camera and was going to enter the structure to conduct an interior size-up with the camera. The fire fighter from Engine 73 pulled the 1¾-inch hoseline off Engine 76, and was only able to stretch it to the west side door before dropping it and entering with her Captain. The two advanced approximately 20 feet inside but never made contact with the other fire fighter, who had stretched his hoseline inside, past the front counter, and around a wall in the dining area (see Diagram 2).
After stretching approximately 20 feet of additional hoseline to the victims, the Captain from Engine 76 reentered to find his crew. He entered the small opening in the west side door. Grabbing onto a hoseline he thought the victims were on, he followed the hoseline past the front ordering counter and then turned around a corner wall. He met up with a male fire fighter whom he thought was Victim #1, but he was actually the fire fighter from Engine 73 who had stretched a line in by himself. The fire fighter told the Captain that he could not see the fire. The Captain stated that there was still very little heat and no visible fire as he followed the hoseline to the exit and relay the information to the IC, face-to-face.
At 0444 hours, the IC walked around to the east side to check conditions. He noticed a small amount of fire in the middle interior section of the restaurant and then walked back to the west side. At 0445 hours, Engine 10 arrived on the scene and was ordered by the IC to catch a plug on the east side and assist with the fire attack. Engine 10 radioed the IC, stating that they couldn’t catch a plug on that side. The IC then ordered them to set up their deck-gun on the east side and wait for further assignment. Soon after, Engine 75 arrived on the scene, caught a plug on the south side, and laid a supply line into Engine 76. After laying the line, the Captain and two fire fighters from Engine 75 proceeded to the west side of the building. They stated that the roof was self-venting with approximately 25-foot flames emitting from the center of the building. District 69 arrived on the scene and reported to the command post.
The Captain from Engine 76 had exited the structure and relayed that they could not find the fire. The IC stated that it must be in the ceiling and they would need pike poles to get to it. The Captain from Engine 76 then turned and followed the same hoseline to the exit, thinking he would meet his crew.
At 0446 hours, District 10 (District Chief) arrived on the scene and after completing a walk-around size-up, he assumed command. At 0448 hours, the Captain and a fire fighter from Engine 75 grabbed the 1¾-inch hoseline that the other fire fighter from Engine 73 had stretched to the door, and entered approximately 8 feet inside through the west side door. As they opened the nozzle to apply water over the kitchen area they could feel debris falling from above. At the same time the Captain from Engine 76, who was following the hoseline taken in by the fire fighter from Engine 73, crawled past the ordering counter to the corner when he felt debris fall from above, almost knocking him completely to the floor. The Captain proceeded on the line and met up with the fire fighter from Engine 73 who had the nozzle open and was hitting a fire towards the rear of the kitchen area.
Other fire fighters in the vicinity and the Captain and a fire fighter from Engine 73, who were using a thermal imaging camera, later stated that the heat had intensified and became more noticeable. The Captain pointed the camera towards the ceiling and could see heavy, rolling fire. He then pointed it back towards the floor and the screen went completely white, indicating uniformly high levels of heat. It is believed that the roof had already collapsed in the kitchen area during this time, however, no fire fighters can recall seeing or hearing the collapse take place (see Photo 9).
At 0451 hours, the Captain from Engine 75 exited the building to talk with the IC. At this time the following fire fighters were still inside the building: the fire fighter from Engine 75 (on the nozzle of one of the hoselines), the Captain and a fire fighter from Engine 73 (with the thermal imaging camera), Victim #1 and Victim #2 (in the kitchen area and behind the counter with a hoseline), the Captain from Engine 76 and a fire fighter from Engine 73 (on the same hoseline in the dining area). There were now approximately 30-foot flames extending from the center section of the building and the IC could see heavy fire in the kitchen area. Based on this observation of the fire conditions, at 0452 hours the IC decided to evacuate fire fighters from the interior and order a defensive attack. He radioed dispatch and asked them to sound an evacuation tone and ordered the FAOs to blow their apparatus air horns to send an additional evacuation tone. The fire fighters who were inside heard the tones and immediately exited. The Captain from Engine 76 reached the west door and saw fire fighters waiting there. He asked the fire fighters at the door if they had seen any of his crew (Victim #1 and Victim #2) exit, and he received a negative response. He waited for them at the door as another fire fighter exited. After learning that it was the fire fighter from Engine 73, who had been on the line with him, he informed the IC that Victim #1 and Victim #2 had failed to exit. At 0453 hours, the IC ordered a personal accountability request (PAR) from all companies on the scene. By 0500 hours, all companies had confirmed a PAR except Engine 76.
The IC ordered the Captain and a fire fighter from Ladder 75 to act as the rapid intervention team (RIT) and enter and search for the victims. They were given the assignment to enter through the west side door, and follow the victims’ hoseline to the nozzle. Both fire fighters entered and followed what they thought was the victims’ hoseline. Instead, they followed the hoseline taken into the building by the fire fighter from Engine 73. The Captain and fire fighter reached the nozzle but were unable to locate either of the victims.
At 0502 hours, the IC struck a second alarm. Dispatch toned out Engine 39, Engine 82, Engine 60, Engine 68, Engine 69, Ladder 68, Ladder 69, Rescue 11, Rehab 17, and Safety 2 as the second-alarm companies. He then ordered the Captain and two fire fighters from Engine 75 to enter the building through the west side doors with a 1¾-inch hoseline, to hold back the fire as the fire fighters entered. As the Engine 75 crew advanced the line into the building, the Captain and fire fighter from Ladder 75 (RIT) exited. During their exit, the Captain and fire fighter became separated as the fire fighter followed the line out to the west side. Once outside, the fire fighter told the IC that they had reached the nozzle and neither victim was near it. The Engine 75 Captain became concerned over the location of the Captain from Ladder 75. The Engine 75 Captain decided to leave his crew with the hoseline and search for the Captain from Ladder 75. The Captain stated that he located the Captain from Ladder 75, and the two exited the west side doors together.
The fire fighter from Engine 73, who was on an interior hoseline prior to the evacuation tone, heard the IC sending fire fighters inside and decided to reenter to search. Assuming that his Captain was behind him, he reentered and followed the line that he had previously taken in, all the way to the nozzle. He reached the nozzle and opened it on the fire. The IC walked around to the east side and ordered the Captain and two fire fighters from Engine 10 to enter through the east side doors with a 2½-inch hoseline and search for the victims. The Captain and two fire fighters entered the building and were unable to maneuver the 2½-inch line around the fallen debris. They exited and pulled a 1¾-inch hoseline from their engine to the interior. Once inside, the Captain and one of the fire fighters took a rope line, which was tied off to the exterior, and searched for the victims as the other fire fighter manned the 1¾-inch hoseline, approximately 10 feet inside the east door. The Captain and fire fighter heard a personal alert safety system (PASS) device alarming in the southwest section of the building. They followed the tone and found it to be one of the fire fighters on the west side who was searching for the victims. The Captain and fire fighter then met with the other fire fighter (from Engine 73) on the hoseline and exited the structure, due to low air. After exiting, they went to the rear of the building and checked a rear steel door. They stated that the door was extremely hot, discolored, and too hot to open.
The Captain and a fire fighter from Ladder 76 pulled a 2½-inch line off Engine 76 and applied water from the exterior through one of the drive-through windows to hold back the fire in the kitchen area. The fire fighter from Engine 73, who was still inside applying water, stated that he did not feel that he was making any progress and the heat was intensifying. He decided to turn and exit the building. As he attempted to exit, his SCBA air cylinder became entangled in fallen wires and debris. As he fought to untangle himself, his foot got caught in a dining table. After an exhausting struggle to free himself, he saw a light towards the east side and crawled towards it. The light appeared to be from a large window (which self-vented during the fire) which he climbed through and fell into a flower bed. Unable to move due to exhaustion, the fire fighter laid there until the FAOs from Engine 10 and Engine 75 assisted him to Engine 10, where they requested an ambulance to treat him for exhaustion.
At 0510 hours, Engine 82 arrived on the scene and attempted to shut off the gas (a second time). As they attempted to shut off the gas, the Captain from Ladder 75 put a ladder up to the roof line on the west side to look down inside the building. At approximately the same time, one of the fire fighters from Engine 75, who was on the hoseline inside the west door, exited the building. The Captain from Engine 73 noticed that his fire fighter, who had entered through the west door, had never come out and the Captain became concerned. He informed the IC that he had a fire fighter missing and he was going to go around to the east side to look for him. He told his other fire fighter to stay with the IC. The IC noticed that only one fire fighter from Engine 75 was on the hoseline and ordered the fire fighter from Engine 73, who was standing with him, to enter and back up the Engine 75 fire fighter on the hoseline. Shortly after this, the Captain from Engine 73 found his missing fire fighter, on the east side, receiving medical attention. Note: This was the fire fighter from Engine 73 who had climbed out the east side window and received assistance.
At 0517 hours, the Captain from Ladder 75, who had put the ladder up to the roof line, stated that he heard a PASS device going off in the kitchen area. Engine 68 and Engine 69 arrived on the scene shortly after. The IC was informed that a PASS device was sounding in the kitchen area. The IC immediately ordered Engine 82 and Engine 68 to enter the east side to search for the victims. The Captain and two fire fighters from Engine 82 and the Captain and two fire fighters from Engine 68 entered the east side window to search for the victims. They stated that there was a lot of debris and that there were small fires burning. One of Engine 68’s fire fighters found a hoseline and opened it up on the small fires.
At 0527 hours, the IC struck a third alarm. Dispatch toned out Engine 48, Engine 57, Engine 78, Ladder 28, Ladder 78, Ladder 51, District 21, and the communications van as the third-alarm companies. The IC then ordered Engine 69 to enter the east side with a hoseline and hold back fire on that side as crews searched. The Captain and two fire fighters from Engine 69 entered through the east side window with a 1¾-inch hoseline.
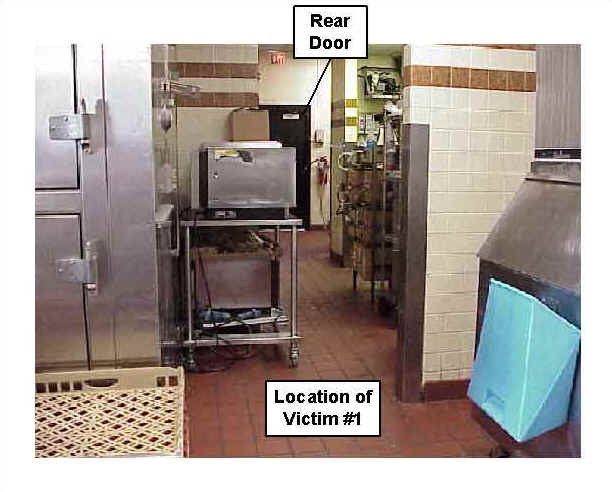
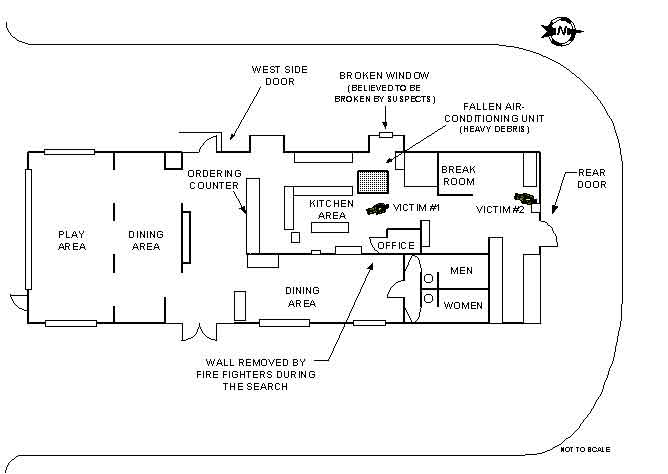
At 0528 hours, Ladder 68, which arrived on the scene shortly after Engine 68, forcibly opened the rear (north) steel door (see Photo 10). They stated that there were visible spots of fire inside the doorway. At approximately the same time, the IC radioed the Engine 82 crew, which was still inside on the east side, to exit. The Captain radioed the IC stating that he felt they were close to the victims because they could hear a PASS device in the area. Note: All fire fighters were equipped with PASS devices integrated into their SCBAs. At 0530 hours, a fire fighter from Ladder 68 entered through the rear door and told his Captain, who was still standing at the rear door, that he could see one of the victims. The Captain then radioed the IC stating that they had found one of the fire fighters and would need assistance at the rear door. At approximately the same time, fire fighters from Engine 82 had broken down a section of wall separating them from the office, and were able to get to the victim (see Photos 11 and 12). The fire fighter from Ladder 68 found the victim, who was identified as Victim #1, with his SCBA facepiece donned, but his regulator not connected. His SCBA air cylinder harness was partially removed and entangled in wires. The victim also had several items of debris on him. The fire fighter from Ladder 68, with the assistance of a fire fighter from Engine 82, freed the victim from the wires and debris and attempted to remove him from the structure. As they moved him, he kept getting caught on other wires and debris. At 0532 hours, additional fire fighters entered the rear door of the structure and removed Victim #1. Cardiopulmonary resuscitation (CPR) was administered by fire fighters as the victim was loaded into an ambulance and transported to a nearby hospital. He was later pronounced dead at the hospital.
At 0533 hours, Rescue 11 was on the scene and reported to the rear door. Assuming that Victim #2 was in the general vicinity where Victim #1 was found, the IC ordered Rescue 11 to enter the rear door and search for her. The fire fighter from Ladder 68, who found Victim #1, reentered with Rescue 11 (Captain and two fire fighters) and showed them where Victim #1 was found. He then exited as Rescue 11 searched. They searched for approximately 20 minutes and then exited to change their air cylinders. Rescue 11 stated that there was a lot of debris and that there was a 2-inch main gas line burning in the area they were searching. At 0543 hours, the Chief arrived on scene and assumed command. At 0556 hours, Rescue 11 noticed a fire fighter’s boot near the area where Victim #1 was found. They radioed the Chief reporting that they thought they had found Victim #2. The Chief, a Captain and two fire fighters from Rescue 11, and the Captain from Ladder 76, entered the rear door of the building. They walked to the area where Victim #1 was found and located the fire fighter’s boot, near a HVAC unit on the floor. They assumed—based on the location of the boot and on the nearness to the other victim’s location—that Victim #2 was under the fallen debris and HVAC unit (see Photo 11). Concerned about the burning gas line and fearing another collapse, the Chief then ordered everyone out and requested a PAR for all companies. He then ordered all first-alarm companies to report to the designated rehabilitation area. He radioed dispatch and requested the gas company to respond and shut off the gas. He again received a complete PAR for all companies except Engine 76.
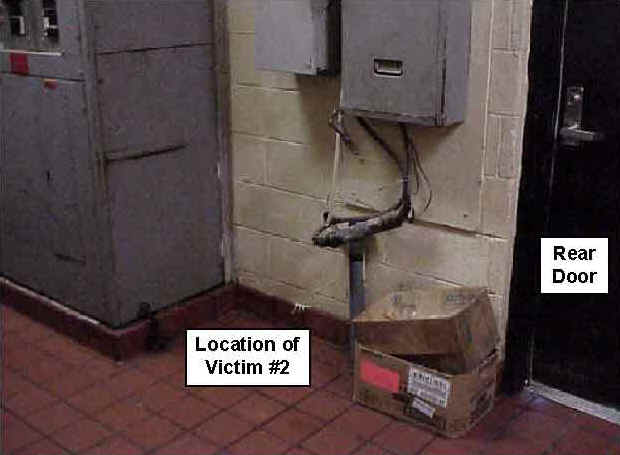
At approximately 0600 hours, the Chief radioed dispatch and requested a crane to the location to remove the large HVAC unit. Shortly after, the gas company arrived and shut off the gas supply to the restaurant. Based on the amount of fire throughout the incident, the time which had elapsed to this point, and the location where they thought Victim #2 to be, the Chief had declared this incident as a recovery. As they waited for the crane to arrive, the Chief and fire fighters discussed how they would remove the HVAC unit when the crane arrived. Rescue 11 (Captain and two fire fighters), District 69, Safety 2, Engine 60 (Captain and two fire fighters), and the Chief entered the rear door to determine how they would hook the HVAC unit to the crane. At 0713 hours, the Chief and fire fighters exited. As they exited, Safety 2 and District 69 decided to search the northwest area of the rear door. Safety 2 noticed what appeared to be fibers of a SCBA air cylinder and alerted District 69. As they walked closer they noticed that it was Victim #2. She was found by a safe, approximately 6 feet to the west side of the rear, steel door (see Photo 13, Photo 14, and Diagram 4). She was found entangled in wires and a pair of wire cutters (believed to be hers) were found nearby. Investigators could not determine if the victim was wearing her SCBA at the time of her death due to severe fire damage to the SCBA unit. However, she was seen entering the restaurant with her SCBA donned. Victim #2 was pronounced dead at the scene. The scene was then turned over to the City Arson Bureau who declared this fire as arson. Fire fighters were then released from the scene and the department set up debriefing at a nearby fire station.
Note: The SCBAs used by the fire fighters in this incident have been referenced in a safety notice, which was issued by the SCBA manufacturer.1 The notice states that the distress alarms (integrated PASS) can inadvertently alarm, reset, or be shut off, possibly by interference from a portable two-way radio. Neither of the victims were equipped with a portable radio nor were found with a portable radio near them. Neither of the SCBAs could be tested due to severe heat damage. To obtain a copy of the safety notice contact Scott or your Authorized Scott Service Center.
Scott Tech Support 1-800-247-7257
e-mail to hsservice@scottaviation.com
website: www.scottaviation.com
CAUSE OF DEATH
The medical examiner listed the cause of death for both victims as asphyxia due to smoke inhalation.
RECOMMENDATIONS AND DISCUSSION
Recommendation #1: Fire departments should ensure that the department’s Standard Operating Procedures (SOPs) are followed.2
Discussion: According to this department’s SOPs, the following procedures should take place:
• Ensure that crews enter and exit together, stay together, and be equipped with a portable radio.2
Department’s SOPs state that crews should stay together, especially when performing a "fast attack." The company officer should remain with his or her crew and provide the appropriate level of supervision. Fire fighters should enter and exit together and no fire fighter should operate alone. When the decision is made to make a "fast attack," company officers should also be equipped with a portable radio. The radio will permit the officer to communicate directly with the Incident Commander. If problems occur, the Incident Commander could be immediately notified.
• Ensure that a Tactical Evaluation and Assessment Plan is completed for possible hazardous buildings.2, 3
Department SOPs state that a Tactical Evaluation and Assessment Plan should be established to gather information on buildings within the fire department’s jurisdiction. Other fire departments may refer to this as a prefire plan or inspection. Prefire plans or inspections are excellent opportunities for fire departments to determine the following: age of the structure, structural integrity, exposed interior insulation materials, type of roof structure and supports (truss, bowstring, etc.), type of interior support structures, type of materials used in the structure (such as wood, steel, plastics, foam, or materials that produce toxic gases when subject to heat), storage of flammable or toxic materials, amount of load (HVAC units, coolers, etc.), water supply, and automatic sprinkler systems. Prefire plans or inspections provide a wealth of information to fire fighters when responding to an incident. When fire fighters respond to an incident, the prefire plan information could alert them to any hazards or possible unsafe conditions that they could be exposed to.
As a part of the prefire plan or inspection, fire departments can visit buildings in their jurisdiction that are under construction and make notes of the interior building components. Additionally, fire fighters can record information regarding structures in their jurisdiction that incorporate a truss system. For example, a Captain with the Phoenix Fire Department put together a photo log which contained information on all buildings with truss systems in their responding territory. The log consisted of pictures, addresses, occupancy of buildings, operating hours, roof systems (truss, bowstring, etc.), flammable materials, and additional notes. When the Captain and his crew respond to an incident, the Captain can refer to the log and predetermine if the structure incorporates a truss system. If so, fire fighters can be provided with important information before arriving on the scene. This could also provide the Incident Commander with the opportunity to develop or make changes to the strategic plan or tactics on the scene.
Recommendation #2: Fire departments should ensure that fire command always maintains close accountability for all personnel at the fire scene.4, 5, 6
Discussion: Accountability on the fire ground is paramount and may be accomplished by several methods. It is the responsibility of every officer to account for every fire fighter assigned to his or her company and relay this information to Incident Command. Accountability on the fire ground can be maintained by several methods: by a system using individual tags for every fire fighter and officer responding to an incident, or by a company officer’s riding list, stating the names, assigned tools, and duties of each member responding with every fire company. One copy of the list should be posted in the fire apparatus and one copy carried by the company officer. The list posted in the apparatus is used if the company officer or the entire company is reported missing. Additionally, fire fighters should not work beyond the sight or sound of the supervising officer unless equipped with a portable radio. Fire fighters should communicate with the supervising officer by portable radio to ensure accountability and indicate completion of assigned duties. Standard Operating Procedures (SOPs) should address accountability, including the location and the duties of the responding fire companies. Just as company officers should know the location of all fire fighters assigned to the company, the chief officer in command should know the operating locations of officers and companies assigned on the first-alarm assignment. As a fire increases and additional fire companies respond to the fire, a communication assistant with a command board should assist the Incident Commander with accounting for all fire companies at the scene, at the staging area, and at rehabilitation. One of the most important aids for accountability at a fire scene is an incident management system. It should be established by the Incident Commander of the incident. The department in this incident had in place a personal accountability report (PAR) system at the time of this incident. The PAR system is set up by the dispatcher sending a message to the IC requesting an accountability report for all crews on the scene. The message is sent every 30 minutes once the crews are on the scene. When this message is received, the officer for each crew is responsible for communicating to the sector officer a report of accountability for their crew. Since this incident, the department has been testing a tag accountability system. Regardless of which system is used, proper communication and adherence to SOPs are necessary to ensure personnel accountability on the fireground.
Recommendation #3: Fire departments should ensure that Incident Command conducts an initial size-up of the incident before initiating fire fighting efforts and continually evaluates the risk versus gain during operations at an incident.3, 5, 7-9, 10-12
Discussion: One of the most important size-up duties of the first-in officers is locating the fire and determining its severity. This information lays the foundation for the entire operation. It determines the number of fire fighters and the amount of apparatus and equipment needed to control the blaze, assists in determining the most effective point of fire extinguishment attack, and the most effective method of venting heat and smoke. A proper size-up begins from the moment the alarm is received, and it continues until the fire is under control. Several factors must be evaluated in conducting the size-up - e.g., type of structure, time of day, contents of the structure, potential hazards, etc. The size-up should also include risk versus gain during incident operations. The following factors are important considerations:
1. Occupancy type involved. The type of occupancy can have a great effect on the aspects of the fire attack. The type of occupancy could assist in determining the structure’s layout, hazardous materials, and the possibility of civilians (e.g., civilians will be present in a hospital around the clock).
2. Smoke conditions. The smoke conditions can provide the Incident Commander with additional information about the fire. For example, if the fire is in the roof and burning roofing materials, the smoke would probably appear to be thick and black.
3. Type of construction. The type of construction will be one of the most important areas to identify. The type of structure could provide the Incident Commander information such as how the building may hold up under fire conditions, or if the building is generally subject to collapse under fire conditions.
4. Type of roof system. The roof system should be one of the first things that is determined before fire fighters enter a burning structure. One type of roof system is the lightweight truss roof. It is generally formed by 2- by 4-inch or 2- by 6-inch lumber, attached together with metal gusset plates. The structural idea of the lightweight truss is to distribute loads over a large area.
5. Age of structure. The Incident Commander should ascertain the age of the building when determining strategy or tactics. The age of the structure can provide the Incident Commander with information to help determine the building’s integrity or other vital information such as construction methods or construction materials.
6. Exposures. The Incident Commander should evaluate the whole picture. The protection of exposures near or connected to a burning building should be included in the strategic plan.
7. Time considerations. Information such as time of incident, time fire was burning before arrival, time fire was burning after arrival, and type of attack, is some of the most important information the Incident Commander could have.
• Departments should ensure that the first officer or fire fighter inside evaluates interior conditions and reports them immediately to the Incident Commander.
Interior size-up is just as important as exterior size-up. Since the IC is staged at the command post (outside), the interior conditions should be communicated as soon as possible to the IC. Interior conditions could change the IC’s strategy or tactics. For example, if heavy smoke is emitting from the exterior roof system, but fire fighters cannot find any fire in the interior, it is a good possibility that the fire is above them in the roof system. It is important for the Incident Commander to immediately obtain this type of information to help make the proper decisions.
Recommendation #4: Fire departments should ensure that vertical ventilation takes place to release any heat, smoke, and fire.7, 10, 13
Discussion: Ventilation is necessary to improve the fire environment in order for fire fighters to approach a fire with a hoseline for extinguishment. Additionally, smoke, heat, and gases should be vented above the fire to prohibit conditions necessary for a flashover. This should be completed as soon as possible. Vertical ventilation will delay heat buildup at the ceiling level of the burning room; it may also delay flashover long enough to allow a quick search for a victim; and it may assist in the advancement of an attack hoseline. Ventilation decisions should be a part of the initial size-up. If it is determined that ventilation cannot be completed because of unsafe areas or conditions (e.g., spongy roof, trusses exposed to fire, etc.), then fire fighters should not be exposed or operate under the unsafe areas or conditions.
Recommendation #5: Fire departments should ensure that fire fighters are trained to identify truss roof systems.13-15
Discussion: Trusses come in many sizes, shapes, and design. It is important that fire fighters are able to identify them and the dangers they may pose. Trusses generally consist of wood but may also be constructed with other types of metals. All the materials may act differently under fire conditions, but all are subject to failure. Fire fighters should be provided with training to identify the different types of truss systems and their potential hazards in a fire.
Fast-food restaurants have been known to incorporate the truss as a roof support system. The majority of fast-food restaurants are designed to incorporate large open spaces for dining. The truss system can be designed to span large areas and allow for large open areas. Training to identify trussed buildings should be a part of the fire department’s prefire fire planning or inspections.
Recommendation #6: Fire departments should ensure that fire fighters use extreme caution when operating on or under a lightweight truss roof and should develop standard operating procedures for buildings constructed with lightweight roof trusses. 10, 13, 16
Discussion: The lightweight, wood truss incorporates wooden members which can be as small as 2- by 4-inch timber connected with metal gusset plates. Fire engineering calculations show that lightweight trussed rafters may be expected to collapse in as soon as 10 minutes in a fully developed fire.10
The trusses are designed according to specified load amounts. The loads are generally HVAC units, compressors, air ducts, cooling lines, rest room ventilation fans, grease exhaust ducts and exhaust fans, snow, and ice. Additional loads, which could be applied after the truss is in place, are antennas, satellite dishes, flags, banners, large air-filled advertisements with air blowers, and improperly stored items. The trusses are designed to distribute the loads throughout the roof system and can span large openings without interior load-bearing walls. Since the trusses are tied together and are designed to distribute the load, if one of the trusses fails it places an additional load on the others, which could cause a chain reaction of failure leading up to a collapse. The document, Building Construction for the Fire Service, states that "The metal gusset plates can also be weakened or destroyed by fire by acting as a heat collector, delivering the heat to the metal gusset plate teeth, which can pyrolytically destroy the tensioned wood fibers, which had been gripping the metal teeth. Sometimes trusses are set in multiples to cope with a concentrated load. This does not suffice in a fire because all the trusses can be exposed to the same fire conditions. An additional load not incorporated into the design can shorten the time to failure in a fire. When a fire occurs in this type of truss, it generally travels rapidly throughout them reducing their structural integrity." 13
Additional hazards that exist with truss systems are "truss voids" or "trussloft." It is described as the void of space between the ceiling and roof, which is not high enough to be called an attic. The lightweight trusses are designed in a series of triangles which create the trusses’ structural integrity. The area from the top chord of the truss to the bottom chord is known as the "truss void" or "trussloft," which creates a path for rapid fire spread. Even if firestops are placed in the voids, openings for duct work, appliance lines, electrical lines, conduit, or additional utility installations create a path for fire to spread. Additionally, Building Construction for the Fire Service notes that no tests exist which demonstrate the effectiveness of firestopping or draftstopping for its intended purpose:
All personnel at a fire scene should be alert to exterior conditions. Fire or heavy smoke from the roof indicates that the trusses are on or have been exposed to fire. The truss voids in the ceiling may harbor a well-concealed fire that is ready to burst out with almost an unbelievable fury when oxygen is admitted to a void containing heated carbon monoxide. The reaction can range from a deflagration to a detonation, from a backdraft or flashover to an explosion capable of blowing a building apart. Any ceiling below a truss void should be pulled and examined by disciplined fire fighters under control, standing near a doorway for rapid escape. If there is a fire barrier in the void, the same procedure should take place on the opposite side.13
The above-referenced document also states that fire fighters should be extra careful when responding to a fire in a fast-food restaurant at night. Due to less light and possible weather conditions, the conditions can be misleading. After a line is stretched to the interior, the ceiling is pulled or tiles are raised. In most cases, minor fire is found and extinguished. In the worst case, the fire in the void is accelerated and the roof falls. A well-known cautionary phrase within the fire service bears repeating - "Beware of the Truss!"13
• Develop standard operating procedures for buildings constructed with lightweight roof trusses.
Standard operating procedures should be developed and implemented for buildings constructed with lightweight roof trusses. The SOPs should be provided to all fire fighters and training should take place to identify buildings constructed of lightweight roof trusses (see also Recommendation #5).
A past article authored by Vincent Dunn, retired Deputy Chief, New York Fire Department, states that if fire fighters arrive upon a structure fire and the fire involves the burning of the truss structure, a defensive fire fighting strategy should be employed: Remove people from the building and attack the fire from the exterior.16 Over the past 4 years, approximately 10 fire fighter fatalities have occurred due to truss-related incidents.
Recommendation #7: Fire departments should ensure that fire fighters performing fire fighting operations under or above trusses are evacuated as soon as it is determined that the trusses are exposed to fire.13
Discussion: There is no specific time limit on how long fire fighters should operate under or on truss roofs that are exposed to fire. A time limit is often used by fire departments as a guide for operation under or on truss roofs. Even though standard fire engineering calculations show that lightweight trusses may be expected to collapse after about 10 minutes in a fully developed fire, it is not recommended to set a time limit. "Under fire conditions, truss failure is unpredictable."13 When fire fighters arrive on the scene of a building with trusses exposed to fire, it is virtually impossible to identify how long the trusses have been exposed to fire and set a time limit for fire suppression. When it is determined that the building’s trusses have been exposed to fire, any fire fighters operating under or above them should be immediately evacuated. If it is not clear that the building’s trusses have been exposed to fire, a defensive attack should take place until the conditions can be verified.
Fire fighters may have difficulty in finding the exact location of fire in a building, even though heavy smoke makes it clear that fire is present. The fire could be in a void or concealed area. For example, fire-rated suspended-ceiling panels create a space between them and the top chord of the roof truss. The void creates a path for rapid fire spread and can shield the fire from the fire fighter’s sight. The term "fire-rated" should not be misinterpreted. It does not provide any fire resistance, but merely meets fire code requirements for rate of flame spread. The design of suspended-ceiling panels provides a void to hide the fire and store carbon monoxide. If the suspended ceiling would collapse while fire fighters were under it, the fire fighters could become entangled in the steel supporting grid. Additionally, fire fighters could become entangled in wire and other loose debris falling from the suspended ceiling and could be trapped in the building.
Recommendation #8 : Fire departments should explore using a thermal imaging camera as a part of the exterior size-up.9, 17-19
Discussion: Thermal imaging cameras are being more frequently used by the fire service. One function of the cameras is to locate the fire or heat source. Additionally, "Infrared thermal imagers assist fire fighters in quickly getting crucial information about the location of the source (seat) of the fire from the exterior of the structure, so they can plan an effective and rapid response with the entire emergency team. Knowing the location of the most dangerous and hottest part of the fire helps fire fighters determine a safe approach and avoid structural damage in a building that might have otherwise have been undetectable. Ceilings and floors that have become dangerously weakened by fire damage and threatened to collapse can be spotted with a thermal imaging camera. A fire fighter about to enter a room filled with flames and smoke can judge whether or not it will be safe from falling beams, walls, or other dangers."18 The use of a thermal imaging camera may provide additional information the Incident Commander can use during the initial size-up.
Recommendation #9: Fire departments should ensure that, whenever there is a change in personnel, all personnel are briefed and understand the procedures and operations required for that shift, station, or duty.
Discussion: If a change in personnel is made, such as adding a new officer or fire fighter, a briefing process should take place. Although most officers and fire fighters will complete the same training, procedures and operations can vary by personnel, shift, or station crews. Crew integrity should remain the top priority for all fire departments. To ensure crew integrity, briefing sessions should take place to ensure that all officers and fire fighters understand their positions and what is expected of each other.
Recommendation #10: Fire departments should ensure that, whenever a building is known to be on fire and is occupied, all exits are forced and blocked open.17
Discussion: When fire fighters are in a building, the building is now occupied and all exits should be available, even if the doors must be torn down. The doorway should be clear and free of any debris, so fire fighters and any other occupants can exit if needed. Fire fighters should be aware of the building’s exits and be trained how to force open different doors they may encounter in a building.
Recommendation #11: Fire departments should consider providing all fire fighters with portable radios or radios integrated into their face pieces.6
Discussion: Communication on the fireground between fire fighters and Incident Command is paramount. Fire fighters will enter buildings as a pair or team, and generally a company officer will accompany them. In most fire departments, the company officer or one of the fire fighters will be equipped with a portable radio to keep a line of communication with Incident Command. All the other fire fighters who enter a hazardous condition should also be equipped with a portable radio so, if the officer or fire fighter with the portable radio becomes separated from his partner or crew, voice contact can still be maintained.
Recommendation #12: Fire departments should consider adding additional staff in accordance with NFPA standards.4
Discussion: The NFPA Appendix A-6-4.4 recommends several response options and states in part, "It is recommended that a minimum acceptable fire company staffing level should be 4 members responding on or arriving with each engine and each ladder company responding to any type of fire. The minimum acceptable staffing level for companies responding in high-risk areas should be 5 members responding or arriving with each engine company and 6 members responding or arriving with each ladder company." When structural fire fighting takes place, it is recommended that backup personnel, a RIT team, and other fire fighters be in place to perform any operations needed (e.g., vertical ventilation, horizontal ventilation, forcible entry to secondary exits, etc.). If the personnel are not available, the operations and tactics can be hindered or delayed.
Recommendation #13: Fire departments should establish various written standard operating procedures, ensure record keeping, and conduct annual evaluations to monitor and evaluate the effectiveness of their overall SCBA respirator maintenance program.20
Discussion: Fire departments should ensure that SCBAs are serviced, perform properly, and are reliable. To monitor and enforce the service and maintenance of SCBAs, fire departments should establish written standard operating procedures, ensure record keeping, and conduct annual evaluations. Although there were no SCBA problems noted in this investigation, the fire department requested that NIOSH evaluate their SCBA maintenance program (see Attachment 1).
The following recommendations apply to building owners, utility providers, and municipalities.
Recommendation #14: Utility suppliers should ensure that all exterior building utilities are accessible and in working condition.
Discussion: Utility providers should ensure that the building’s exterior utilities can be turned on or shut off if necessary. Any problems with utilities that the owner may encounter should be reported to the appropriate utility when they are found to be inoperable or in need of repair. The exterior utility shut-off controls should also be in a position where fire fighters can access them. In this incident, the fire fighters made several attempts to shut off the building’s gas supply. However, the attempts were unsuccessful because the shut-off valve was stripped.
Recommendation #15: Building owners should consider placing specific building construction information on an exterior placard.21
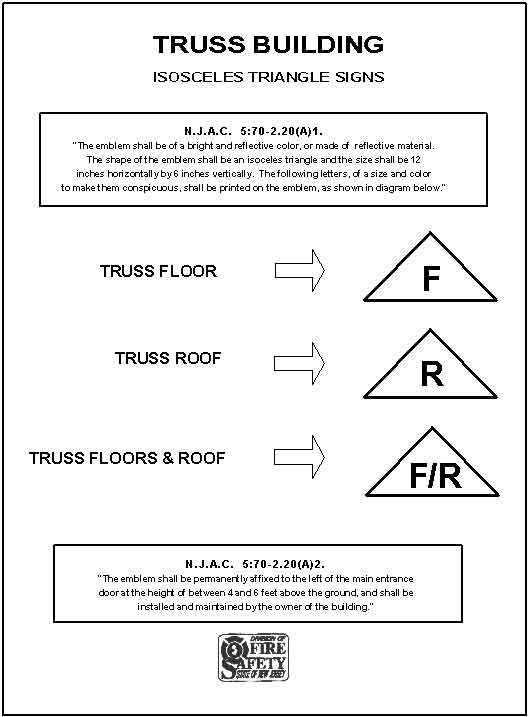
Discussion: Information regarding the building’s construction is very valuable to fire fighters if a fire would occur. The information could provide fire fighters with such information as roof type (lightweight truss, bowstring, etc.), roof materials (metal, wood, etc.), roof loads (HVAC units, displays, etc.), sprinkler system(s), standpipe location, utilities (gas or electric), occupancy, occupancy hours, chemicals on site, pressurized cylinders, contact numbers, and the interior floor layout. This information could save the Incident Commander time when planning the fire attack. Additionally, the information would provide fire fighters with important information that they might not otherwise have access to. To ensure that fire fighters are aware of structures that might have a truss roof, the state of New Jersey has passed a law requiring all building owners to place an exterior placard on structures which incorporate a truss roof (see Attachment 2).
Recommendation #16: Municipalities should upgrade or modify older structures to incorporate new codes and standards to improve occupancy and fire fighter safety.22
Discussion: There are currently building codes and standards which are used as guidelines for new building design and construction. Unfortunately, before municipalities adopted or enforced specific codes and standards, many buildings were designed and constructed without incorporating such standards. New or improved codes have been established which can improve the safety of existing structures. Sprinkler systems are one specific area of concern for older structures. It is proven that sprinkler systems reduce the loss of property and life. There is also a strong possibility that sprinklers could reduce fire fighter fatalities, since they contain, and even extinguish, fires prior to the arrival of the fire department. Sprinklers are currently the most proactive fire safety approach in building construction. The structure involved in this incident did not incorporate a sprinkler system.
REFERENCES
1. SCOTT [2000]. Important safety notice concerning Scott PAK-ALERT distress alarms. Monroe, NC: SCOTT Safety Notice.
2. Fire Department [1991]. Written Standard Operating Procedures.
3. National Institute for Occupational Safety and Health [1999]. Preventing injuries and deaths of fire fighters due to structural collapse. Publication No. 99-146. Division of Safety Research, Morgantown, WV.
4. NFPA [1997]. NFPA 1500: Standard on Fire Department Occupational Safety and Health Program. Quincy, MA: National Fire Protection Association.
5. Dunn V [1992]. Safety and survival on the fireground. Saddle Brook, NJ: Fire Engineering Books & Videos.
6. NFPA [1995]. NFPA 1561: Standard on Fire Department Incident Management System. Quincy, MA: National Fire Protection Association.
7. International Fire Service Training Association [1995]. Essentials of fire fighting, 3rd ed. Fire Protection Publications.
8. Kipp JD, Loflin ME [1996]. Emergency incident risk management: A safety & health perspective. New York: Van Nostrand Reinhold Publishing.
9. Norman J [1998]. Fire officer’s handbook of tactics. Saddle Brook, NJ: Fire Engineering Books and Videos.
10. Dunn V [1988]. Collapse of burning buildings, a guide to fireground safety. Saddle Brook, NJ: Fire Engineering Books and Videos.
11. Dunn V [1996]. Systems analysis, size-up: Part 1. Firehouse, October Issue.
12. Brunacini A [1985]. Fire command, Quincy, MA: National Fire Protection Association.
13. Brannigan FL [1999]. Building construction for the fire service. Quincy, MA: National Fire Protection Association.
14. Kirsch JA [2000]. Fighting fires at fast food restaurants. Saddle Brook, NJ: Fire Engineering, May Issue.
15. Brannigan FL [2000]. A call for fire chiefs. Saddle Brook, NJ: Fire Engineering, May Issue.
16. Dunn V [1998]. Risk Management and lightweight truss construction. New York, NY: WNYF, Official training publication of the New York City Fire Department, 1st issue.
17. Brannigan FL [2000]. Professional review of NIOSH FACE report F2000-13, September 18, 2000.
18. Corbin DE [2000]. Seeing is believing. Dallas, TX: Occupational Safety and Health, August issue.
19. Colley K [1999]. Eyes wide open. Industrial Fire World, March-April issue.
20. National Institute for Occupational Safety and Health (NIOSH) [2000]. Self-contained breathing apparatus (SCBA) maintenance program evaluation, NIOSH Reference: TN-11399. Division of Respiratory Disease Studies, Respirator Branch, NIOSH, Morgantown, WV.
21. New Jersey Uniform Fire Code [1992]. N.J.A.C. 5:70-2.20: Identifying emblems for structures with truss construction.
22. NFIP Fire Analysis Division [1987]. Automatic sprinkler systems do have an impact in industry. Fire Journal.
INVESTIGATOR INFORMATION
This incident was investigated by the following; Frank C. Washenitz II, Thomas P. Mezzanotte, Mark McFall, Safety and Occupational Health Specialists, Division of Safety Research, Surveillance and Field Investigations Branch.
The self-contained breathing apparatus maintenance program was evaluated by Tim Merinar, Engineer, and Thomas McDowell, Physical Scientist, Division of Respiratory Disease Studies, Respirator Branch.
The development of the fire model for this incident was by Dan Madrzykowski, Engineer, National Institute of Standards and Technology (NIST).
Technical review and assistance in completing this report was provided by Brad Newbraugh, Physical Science Technician, and Richard Current, Engineer, Protective Technology Branch, Division of Safety Research.
Expert review was provided by Vince Dunn, retired Deputy Chief, New York City Fire Department, and Francis L. Brannigan, fire and building construction expert.
Photograph courtesy of the City Fire and Arson Bureau.
Photo 1. Metal Gusset Plate Used on Roof System of Restaurant Note: Photo was taken of a restaurant similar to the one involved in this incident.
Photo 2. HVAC Units and Cooking Vents Positioned on the Roof of the Restaurant Note: Photo was taken of a restaurant similar to the one involved in this incident.
Photo 3. Fire’s Point of Origin Was Determined to Have Occurred in the Office of the Restaurant Note: Photo was taken of an office in a restaurant similar to the one involved in this incident.
Photo 4. Drive-Through Window of Restaurant, Located Across From the Office Door Note: Photo was taken in a restaurant similar to the one involved in this incident.
Photograph courtesy of the City Fire and Arson Bureau.
Photo 5. Early Stages of the Restaurant Fire
Photograph courtesy of the City Fire and Arson Bureau.
Photo 6. West Side Door, Entered and Exited by the Fire Fighters
Photo 7. West Side of Restaurant Note: Photo was taken of a restaurant similar to the one involved in this incident.
Photo 8. East Side of Restaurant Note: Photo was taken of a restaurant similar to the one involved in this incident.
Photograph courtesy of the City Fire and Arson Bureau.
Photo 9. Photo Depicts the Restaurant Fire at the Approximate Time the Roof Collapsed
Photo 10. Rear Door Used by Fire Fighters to Gain Access During Search for Victims Note: Photo was taken of a restaurant similar to the one involved in this incident.
Photograph courtesy of the City Fire and Arson Bureau.
Photo 11. Location of Victim #1
Photo 12. Location of Victim #1 Note: Photo was taken in a restaurant similar to the one involved in this incident.
Photograph courtesy of the City Fire and Arson Bureau.
Photo 13. Location of Victim #2
Photo 14. Location of Victim #2 Note: Photo was taken in a restaurant similar to the one involved in this incident.
Diagram 1. Interior Layout
Diagram 2. Initial Hoseline Layout
Diagram 3. HVAC and Exhaust Layout
Diagram 4. Positions of Victims #1 and #2
Respirator Maintenance Program Evaluation
Department of Health & Human Services
Public Health Service
NIOSH Reference: TN-11399
Phone: (304) 285-5907
Fax: (304) 285-6030
March 21, 2000
Dear Chief:
During our visit to the Fire Department on March 7, 2000, Tim Merinar and I had the opportunity to evaluate your fire department’s self-contained breathing apparatus (SCBA) maintenance program. The objectives of our visit were to evaluate your SCBA maintenance program and to make recommendations for improvement. This evaluation consisted of visiting the SCBA maintenance area, interviewing fire department personnel associated with the maintenance of SCBA, reviewing SCBA maintenance records, evaluating the compressed-air cylinder refilling station located at your maintenance facility, examining Mobile Breathing Air 2, and evaluating the compressed-air cylinder refilling station located at Station 11. Our evaluation process benefitted substantially from the cooperation of your staff and the technicians in the SCBA maintenance shop. Their cooperation was instrumental in providing us with information necessary for the evaluation of your SCBA maintenance program.
Your current SCBA maintenance program was evaluated and compared to the respirator and SCBA maintenance requirements listed in the following recognized national standards:
Title 29, Code of Federal Regulations (CFR) Part 1910.134 known as The OSHA Respirator Standard.
National Fire Protection Association (NFPA) 1404, Standard for a Fire Department Self-Contained Breathing Apparatus Program, 1996 Edition.
National Fire Protection Association (NFPA) 1500, Fire Department Occupational Safety and Health Program,1997 Edition
American National Standards Institute, Inc. (ANSI), American National Standard for Respiratory Protection, ANSI Z88.2-1992.
These standards specify the minimum benchmark requirements that all fire department respirator programs should strive to meet or exceed. Compliance with these standards is considered to be essential to maintain SCBA in a condition meeting the certification requirements of the National Institute for Occupational Safety and Health (NIOSH) found in Title 42, Code of Regulation, Part 84, Subpart H, as well as the National Fire Protection NFPA 1981 Standard on Open-Circuit Self-Contained Breathing Apparatus for the Fire Service, 1997 Edition. Failure to maintain your SCBA in an approved condition voids the NIOSH approval until such time as each affected SCBA can be inspected, serviced, and returned to an approved condition.
While the Fire Department SCBA maintenance program is quite good, the following areas were identified within the program as areas where improvement is needed in order to comply with the referenced national standards:
1) Records should be maintained for each SCBA regulator, facepiece, and cylinder at the department. During our visit, we were shown a system where maintenance, repair and testing information was maintained for each SCBA and filed according to company assignment. Electronic files had also been developed to help track SCBA services such as cylinder hydrostatic test schedules and service life dates. NIOSH recommends that the computerized records system be expanded to address the following standard excerpts:
NFPA 1404, Chapter 2-2.3 specifies that an individual record of each SCBA regulator and harness assembly shall be maintained. This record shall include the inventory or serial number, date of purchase, date of manufacture, date placed into service, location, maintenance and repairs, replacement parts used, upgrading, and test performance.
NFPA 1404, Chapter 2-2.4 specifies that an individual record of each SCBA cylinder shall be maintained. This record shall include the inventory or serial number date of purchase, date of manufacture, date placed into service, location, hydrostatic test pressure and dates, and any inspection and repairs. The hydrostatic test dates shall appear on each cylinder according to the manufacturer’s instructions and applicable government agencies.
NFPA 1404, Chapter 2-2.5 specifies that an individual record of each SCBA facepiece shall be maintained. This record shall include the inventory or serial number, date of purchase, location, maintenance and repairs, replacement parts, upgrading, and test performance.
NFPA 1500, Chapter 2-7.5 specifies that each fire department shall assure that inspection, maintenance, repair, and service records are maintained for all vehicles and equipment used for emergency operations and training.
The American National Standard for Respiratory Protection, ANSI Z88.2-1992, Chapter 10.2 specifies that inspection records be maintained for each respirator.
The OSHA Respirator Standard 29 CFR 1910.134(c); 1910.134(h)(3)(iv)(A and B); and 1910.134(m) specify general requirements for record keeping within a respirator program.
2) The Fire Department should establish written standard operating procedures for managing its various SCBA maintenance, repair, and testing functions. Procedures should be developed to address each of the following areas:
1. SCBA Maintenance Training
2. SCBA Inspection
3. SCBA Maintenance
4. Air Quality Program
5. Recharging Cylinders
6. Record Keeping
7. Identification of Defective SCBA and Removal from Service
NFPA 1404, Chapter 1-5.5 and 1-5.6 require the authority having jurisdiction to establish written standard operating procedures and training policies for members responsible for respiratory protection use, cleaning, and maintenance.
NFPA 1404, Chapter 1-5.7 specifies that the authority having jurisdiction shall establish written standard operating procedures for inspection, maintenance, repair, and testing of respiratory protection equipment.
NFPA 1404, Chapter 7-2.3 specifies that written policies shall be established to ensure that air is obtained only from a source that meets the requirements of CGA G7.1, Commodity Specifications for Air.
NFPA 1404, Chapter 7-2.5 specifies that proper cylinder recharging procedures and safety precautions shall be posted in a conspicuous location at each fill station.
The OSHA Respirator Standard 29 CFR 1910.134(c)(1)(v) and 1910.134(h)(4) require the employer to develop schedules and procedures for inspecting respirators and ensuring that respirators that fail inspection or are otherwise found to be defective are removed from service.
3) Annual evaluations of the SCBA Maintenance Program should be conducted to monitor and evaluate the effectiveness of the overall SCBA maintenance program.
The OSHA Respirator Standard 29 CFR 1910.134(h)(3)(1)(ix) requires the employer to develop and maintain as part of the overall written respiratory protection program, procedures for regularly evaluating the effectiveness of the program.
NFPA 1404, Chapter 8-1.1 specifies that the authority having jurisdiction shall review the organization’s respiratory protection program annually for the purposes of determining the need to upgrade or change various aspects of the program.
These recommendations are based upon the premise that all SCBA are life-saving devices which will only perform as well as they are maintained. Since they are expected to function and perform properly each time they are used, it is important that SCBA maintenance and inspection be given the utmost priority at the department level.
During our visit, we provided your SCBA maintenance personnel with a copy of the peer-reviewed document Respirator Maintenance Program Recommendations for the Fire Service developed by NIOSH and published in the Journal of the International Society for Respiratory Protection. We also provided draft copies of generic standard operating procedures and record keeping forms that may assist you in developing improvements to your overall SCBA maintenance program.
I trust this information is beneficial to your needs. If you have any questions or require additional information, please contact me at (304) 285-6337.
Sincerely yours,
Thomas W. McDowell
Physical Scientist
Respirator Branch
Division of Respiratory Disease Studies
Exterior Placard NJAC 5:70 - 2.20(a)1 and 2 This attachment was provided by the New Jersey Division of Fire Safety and is referenced as Exterior Placard NJAC 5:70 - 2.20(a)1 and 2.

Return to Fire Fighter Homepage
![]()
This page was last updated on 06/13/07